
Abstract
Aims:
As a result of climate change, extreme weather events have increased in frequency, representing one of the most pressing concerns to physical and mental health globally, especially for children. Research suggests that extreme weather events uniquely and adversely affect children in low- and middle-income countries due to developmental and contextual factors. Given the advantages of early intervention, it is critical to aggregate and evaluate current interventions to support this population. This review aims to synthesise evidence on the impact of interventions targeting the development, mental health or wellbeing in early childhood (ages 0–8 years) following extreme weather events in low- and middle-income countries.
Methods:
This review was preregistered with PROSPERO (CRD42023479342). Literature available on seven scientific databases (PsycINFO, Embase, MEDLINE, CINAHL, Web of Science, ERIC, and Cochrane) until February 2024 were reviewed and 744 articles were identified. A grey literature search via Google Scholar, ProQuest, and international agency websites (e.g. Oxfam, UNICEF, Save the Children) identified an additional 48 sources for screening. None of the sources met the inclusion criteria.
Results:
The current review is an empty review with no interventions included.
Conclusion:
The lack of eligible publications within this review indicates an absence of evaluations of interventions in early childhood that may support a population disproportionately vulnerable to the adverse effects of increasing extreme weather events. Research and policy efforts to address this significant gap should prioritise this critical area, focusing on rigorous evaluations and transparent reporting.
Keywords
Key Messages
Children in low- and middle-income countries experience unique adverse effects of extreme weather events and, therefore, require specific and effective psychosocial interventions following these events.
We reviewed the literature and found that there are no evaluations of interventions that address early childhood development, mental health or wellbeing in low- and middle-income countries post-extreme weather events.
The research gap identified within this review may indicate a lack of interventions, evaluations, or of dissemination of current efforts.
There is an urgency to intervene in early childhood to prevent the cascading adverse effects of extreme weather events on mental health and lifelong functioning.
Introduction
Climate change is predicted to intensify the frequency and magnitude of extreme weather events (EWEs). 1 In the past 50 years, the number of EWEs – defined as climate-related disasters excluding geophysical events such as earthquakes and avalanches – has surged by an alarming 456%. 2 While these events have been felt globally, their impacts are unevenly distributed. Research suggests that children in early childhood (aged 0–8 years) and in low- and middle-income countries (LMICs) may experience EWEs and their adverse effects uniquely. 3 The most substantial burden of disease of climate change – nearly 90% of the total – affects children under the age of 5.4,5 Despite contributing the least to carbon emissions that exacerbate climate change, LMICs face the greatest risk from its impacts.6–8 Children in LMICs face additional disadvantages such as a lack of disaster-resistant infrastructure, lack of disaster preparedness, resource limitations, disproportionate impacts of the developed world’s greenhouse emissions on the developing and under-prepared world, fewer support and services as well as delayed or inadequate relief.9–12 Consequently, addressing children's needs is paramount amid the disproportionate burden of climate change on LMICs. This review responds to a call for developmental scientists to help inform and implement evidence-informed policies and strategies to promote early childhood development in the face of this looming threat. 13 In this review, we define EWEs as acute, climate-related disasters such as floods, heatwaves, extreme rainfall or storms, and wildfires. This focus excludes slower-onset climate impacts, or chronic climate change, like rising sea levels, prolonged droughts, long-term changes in temperature and rainfall, and environmental degradation.
Extreme weather events and children
Children in early childhood (0–8 years old 14 ) are at the greatest risk of adverse health and wellbeing outcomes associated with climate change.15–17 This age range represents one of the most sensitive periods for development with processes such as immune, neurobiological, and psychosocial development vulnerable to disruption.18–20 In addition, young children depend on adults for care and protection, who themselves may be negatively affected by the same EWE. 21 Mental health or psychological effects of climate change, especially on children and adolescents, are a growing area within scientific inquiry.22–27 However, there is limited research on the specific mental health effects of EWEs on child survivors,12,28,29 and what does exist tends to focus on children living in high-income countries, rather than those in LMIC settings, leaving the vast majority of the world’s children under-represented and under-served.30,31 As one billion children globally are at extremely high risk from climate change and repeated exposure to EWEs, 3 the associated effects of climate change need further monitoring and research.
Children and adolescents exposed to a single EWE can experience mental health issues like increased post-traumatic stress, anxiety, and depression.25,32,33 Such experiences also heighten negative emotions, including worry, fear, and anxiety about climate change and worsen with repeated exposure. 33 Evidence syntheses of the effects of climate change-related events on children and adolescents reveal high rates of depression, anxiety, and post-traumatic stress disorder, as well as negative cognitive impacts, and sleep and learning problems.34–36 These psychological effects also manifest as difficulties in emotion regulation, behaviour, language development, and academic performance due to displacement or disruptions in children’s environments and social networks, family stress, neurobiological sensitivities to stress and trauma, and limited adaptive capacities.34,35,37 Furthermore, evidence from the USA and Argentina links early childhood EWE exposure to long-term consequences, including increased risk of poor mental health, anxiety, reduced educational attainment, and greater socioeconomic vulnerability in adulthood.38,39
Despite these risks, most investigations into the impacts of EWEs on children typically focus on physical health rather than mental health, and rarely include LMICs.40–42 This is despite evidence indicating that climate change is likely to hinder the mental health and overall development of affected children, especially in LMIC settings. 31 In addition, previous research integrates findings on EWEs with natural hazards in general and aggregates age groups and outcomes,34,35,43 which further obscures effects specific to early childhood and EWEs. In reviews focused on specific geographic regions, researchers note a dearth of primary studies, especially those that include early childhood samples. 44 Therefore, the pathways through which EWEs interact with children’s psychological, socio-emotional, and cognitive development need further exploration.
The first 1000 days of life represent a period of high neuroplasticity.45,46 Experiences in this window critically shape developmental trajectories, have long-lasting adaptive or maladaptive consequences, and influence lifelong health and wellbeing.47,48 This makes early childhood a crucial period to establish and reinforce health and developmental supports.14,45 Alongside broader bio-ecological factors, parents play a central role in determining child outcomes. 45 During and after disasters, caregivers may have less time or capacity to foster attachments with their children, 49 exacerbating issues of hunger and malnutrition that combine to threaten children's learning and development. 50 Parental distress following EWEs may further reduce parental investment in children.51–56 Moreover, parental sociodemographic characteristics, practices, behaviours, and resources are associated with how children experience and recover from trauma,57,58 implying that parents mediate the association between EWEs and child development. Parents also play an important role in protecting children from the adverse impacts of climate-related events 59 and moderating children’s experiences and stress responses. 60 Therefore, understanding caregiver-related factors in disaster contexts aligns with psychosocial, bio-ecological, and dynamic systems models that view the post-disaster environment as a modifiable risk factor in children’s developmental trajectories.61,62
Early childhood development (ECD) interventions are crucial during this sensitive period 14 and typically rely on parent involvement and engagement. Key aspects of parenting interventions include caregiver training on consistent cognitive stimulation, sensitivity, responsiveness, and emotional warmth. 45 Britto et al. 14 have highlighted significant benefits of ECD interventions in LMICs. Specifically, evidence shows that parenting interventions targeting early child learning or parent-child relationships are more beneficial for child development than interventions centred solely on physical health and nutrition.14,63 Similarly, Jeong et al. 62 reported that parenting interventions in the first 3 years improve outcomes across cognitive, language, motor, socio-emotional, attachment, and behaviour outcomes. In sum, these findings reinforce the central role of parents in promoting optimal development in early childhood.
Consistent access to comprehensive early childhood programming – including health, nutrition, and early learning – substantially enhances children’s developmental outcomes,64,65 even in humanitarian and disaster settings.66–68 Providing targeted interventions to children in disadvantaged and vulnerable settings is congruent with the United Nations Convention on the Rights of the Child, 69 which asserts every child’s right to health, education, and protection from harm, starting from birth. Ensuring vulnerable children receive the necessary support to overcome the adverse effects of EWEs is a child rights issue, as it fulfils their entitled rights to health, development, and protection, as stipulated by the Convention.
Applying theories to extreme weather events
In post-climate disaster settings, pregnant women face heightened physical stress, compromised nutrition, and increased exposure to environmental toxins, significantly impacting maternal health and foetal and child development (foetal programming hypothesis).20,70,71 Psychosocial stressors from climate change, including economic downturns and forced displacement, further exacerbate maternal stress and adverse perinatal outcomes, affecting child development.72,73 EWEs also undermine caregiving practices, such as breastfeeding, alter family roles, and disrupt healthcare and social support networks.74–76 Poor maternal mental health further compromises nurturing care and stimulation,77–79 emphasising that EWEs present complex direct and indirect threats to child development.
Bronfenbrenner’s bio-ecological systems theory highlights that child development is shaped by direct interactions with and within environments and broader ecological systems. 80 In the context of climate-related disasters, disruptions are not limited to the microsystem (e.g. caregivers, schools), but also extend to the mesosystem (interactions between home, community, and services), exosystem (community infrastructure, aid availability, family livelihoods), macrosystem (cultural or religious practices, disaster response), and chronosystem (the timing and recurrence of such disasters). This model has informed interventions in humanitarian settings 75 and climate change.12,62 Cuartas et al. 13 expand on this framework by elucidating how both acute climate shocks (such as EWEs) and chronic stressors (socioeconomic disadvantage, displacement) interact across these systems to threaten children’s developmental environments and the adaptability of family systems. Consequently, humanitarian interventions require multi-level approaches that both support children’s individual capacities and address broader systemic factors, 81 which will increase the likelihood of effectively addressing the complex and interacting needs of children affected by EWEs.
Exposure to EWEs, particularly in contexts characterised by limited resources and widespread devastation, is anticipated to be profoundly traumatic for young children. There is consensus that childhood adversity alters the developing brain and body 82 and that it has long-term effects on physical and mental health and wellbeing. 83 EWEs can also be viewed through the lens of the adverse childhood experiences framework 84 due to their potential to engender significant emotional and psychological distress, disruption of support structures, and long-term developmental vulnerabilities. 85 Accordingly, this framework further highlights the importance of interventions that safeguard child development and promote resilience in the face of disaster-related trauma.
This review
While evidence from implementation research on interventions to enhance child development and adaptation outcomes in humanitarian settings is growing, 67 it has not yet fully addressed or evaluated programming related to climate change and climate-related disasters. As far as the authors are aware, there is no systematic synthesis of evidence on interventions aimed at promoting or protecting early childhood development, mental health and/or mental wellbeing following exposure to EWEs. In this review, we will synthesise the existing evidence on the implementation and outcomes of interventions targeting children in LMICs aged 0–8 years who have experienced EWEs.
Methods
The review protocol was preregistered with PROSPERO (CRD42023479342) and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 86 ) guidelines for reviews.
Review scope
All terms as considered in this review are defined in Table 1. The search process utilised the PICOS framework where the Population included children (aged 0–8 years); the Intervention comprised any intervention, programme or activity, with or without a Comparator; the Outcomes were child development, mental health, or mental wellbeing, and the Setting was post-EWEs in LMICs.
Operational definitions
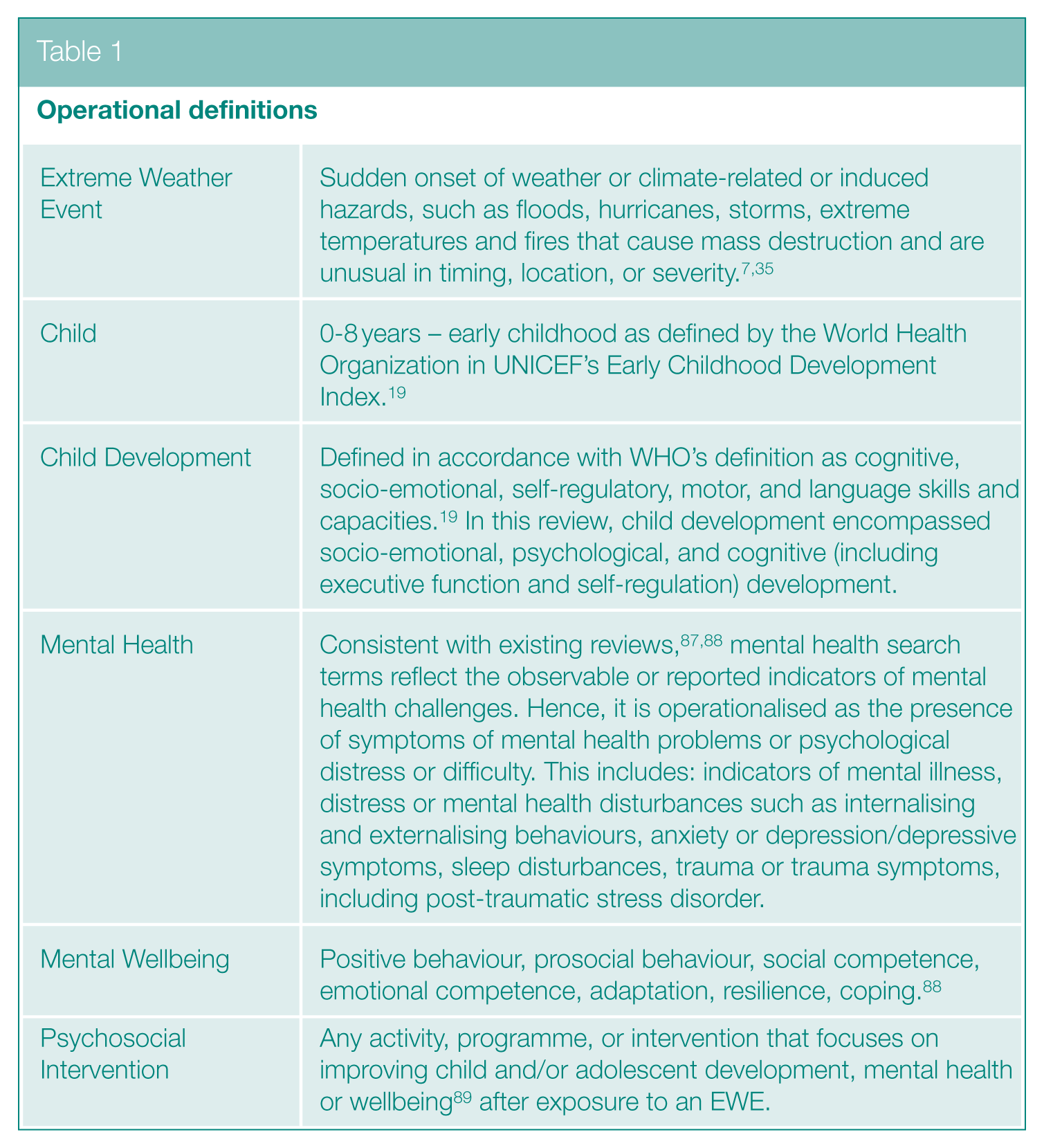
Eligibility criteria
Any publication that reported on early childhood development, mental health, or mental wellbeing as primary or secondary outcomes of an intervention was considered for inclusion. Eligible literature included peer-reviewed and grey literature publications. Only articles published in English were considered for inclusion. Excluded study types included conference proceedings, books, newspaper articles or blog posts, opinion pieces, editorials, and interventions focusing solely on physical health and growth.
All articles published from September 1990, when the UN Convention on the Rights of the Child was ratified, to 1 February 2024 were considered for inclusion. Eligible designs included pilot, implementation, feasibility, or efficacy studies or trials, randomised controlled trials, quasi-experimental, experimental, or pre-post designs, process evaluations, or case studies. Intervention evaluations using quantitative, qualitative, and/or mixed methods were eligible, while interventions without evaluation of outcomes were ineligible. Interventions were eligible if they had been provided to children aged 0–8 years. If the sample covered a wider age range, it was eligible if one of the following conditions was met: (1) 75% of the sample was within 0–8 years, or (2) the data allowed for age-specific analysis. Eligibility was restricted to this age range to retain our focus on early childhood, to capture the vulnerabilities and support needs of this developmental stage, and allow our findings and recommendations to be more homogeneous. Furthermore, in terms of context, the interventions must have been provided up to 12 months after EWEs and in an LMIC; multi-country investigations were considered if all included countries were LMICs, or if the data allowed for country-specific segregation. LMICs were determined using the World Bank classification 90 and included countries on the Development Assistance Committee list of Official Development Assistance in 2023. 91 To account for shifts in country classifications over time and minimise the risk of omitting relevant data, our search strategy also included countries that were LMICs at any point since the Convention’s ratification.
Search strategy
The search strategies were developed by the authors under guidance from a subject librarian and in accordance with existing reviews on similar topics.89,92 The search strategy was modified for each database and combined the following domains using Boolean operators, and where necessary, proximity operators: child AND (development OR mental health OR mental wellbeing) AND intervention AND extreme weather event AND LMIC. A sample search strategy is available as Supplementary Information. Additional search strategies are available upon request.
Searches were run on seven scientific databases: PsycINFO, Embase, MEDLINE on EBSCO Host, CINAHL, Web of Science, ERIC, and the Cochrane Library. The grey literature strategy included searches on Google Scholar and ProQuest where a simplified search string was used with quotation marks and Boolean operators. Titles and abstracts appearing on the first 10 pages were screened and where possible, date and language restrictions were applied to narrow the scope. Eighteen international agency websites were also searched manually to identify primary research or service evaluation reports: BRAC, Children in a Changing Climate, InterAcademy Partnership, International Federation of Red Cross and Red Crescent Societies, Mental Health Innovation Network, Oxfam, Prevention Web, ReliefWeb, Research for Health in Humanitarian Crises, Save the Children, the Alliance for Child Protection in Humanitarian Action, the Mental Health and Psychosocial Support (MHPSS) Collaborative, the United Nations Children's Fund, the United Nations Development Programme, the United Nations Relief and Works Agency, United Nations Office for Disaster Risk and Resilience, the World Health Organization, and World Vision International. We also manually reviewed reference lists of all publications that underwent full text screening. All searches and retrieval were carried out between December 2023 and February 2024 and exported to Covidence (www.covidence.org).
Review procedure
Two authors [TNA and NM] jointly screened 10% of the titles and abstracts on Covidence to ensure consistent application of the eligibility criteria. Next, TNA performed full-text screening of 101 publications, with NM independently reviewing 10% of the full texts. Discrepancies were resolved in consultation with the last author.
Publication details for all grey literature were added to a spreadsheet. The spreadsheet included columns for each component of the eligibility criteria, with options for yes, no, or unsure. During full-text screening, each criterion was assessed individually. Where a publication did not meet any criterion (indicated by a ‘no’ response), it was excluded from further consideration.
Outcomes
Our main focus was on the outcomes of interventions on child development, mental health or wellbeing after exposure to an EWE. An extraction sheet was created capturing the following:
EWE (duration, time since exposure),
Study (design, funding source, comparators),
Sample (recruitment strategy and site, method of engaging children, sample sizes at baseline and completion, gender breakdown, other individuals involved, age range, mean and standard deviation, and eligibility criteria),
Intervention (theoretical orientation, delivery agents, training of delivery agents, intervention dosage, incentivisation, tailoring),
Implementation (barriers, facilitators, outcomes, effect sizes and means, relative risks, odds ratios, risk and mean differences).
Results
The review process is presented in Figure 1. Titles and abstracts of 629 publications were screened, of which 101 advanced to full-text screening. At full-text, no studies met the eligibility criteria and the reasons for exclusion were recorded. The most common reason for exclusion was that interventions were provided to children older than 8 years, or data could not be disaggregated by age (n = 33), followed by no or wrong intervention (n = 26) such as disaster preparedness or disaster risk mitigation interventions. All excluded publications are available as Supplementary Information.
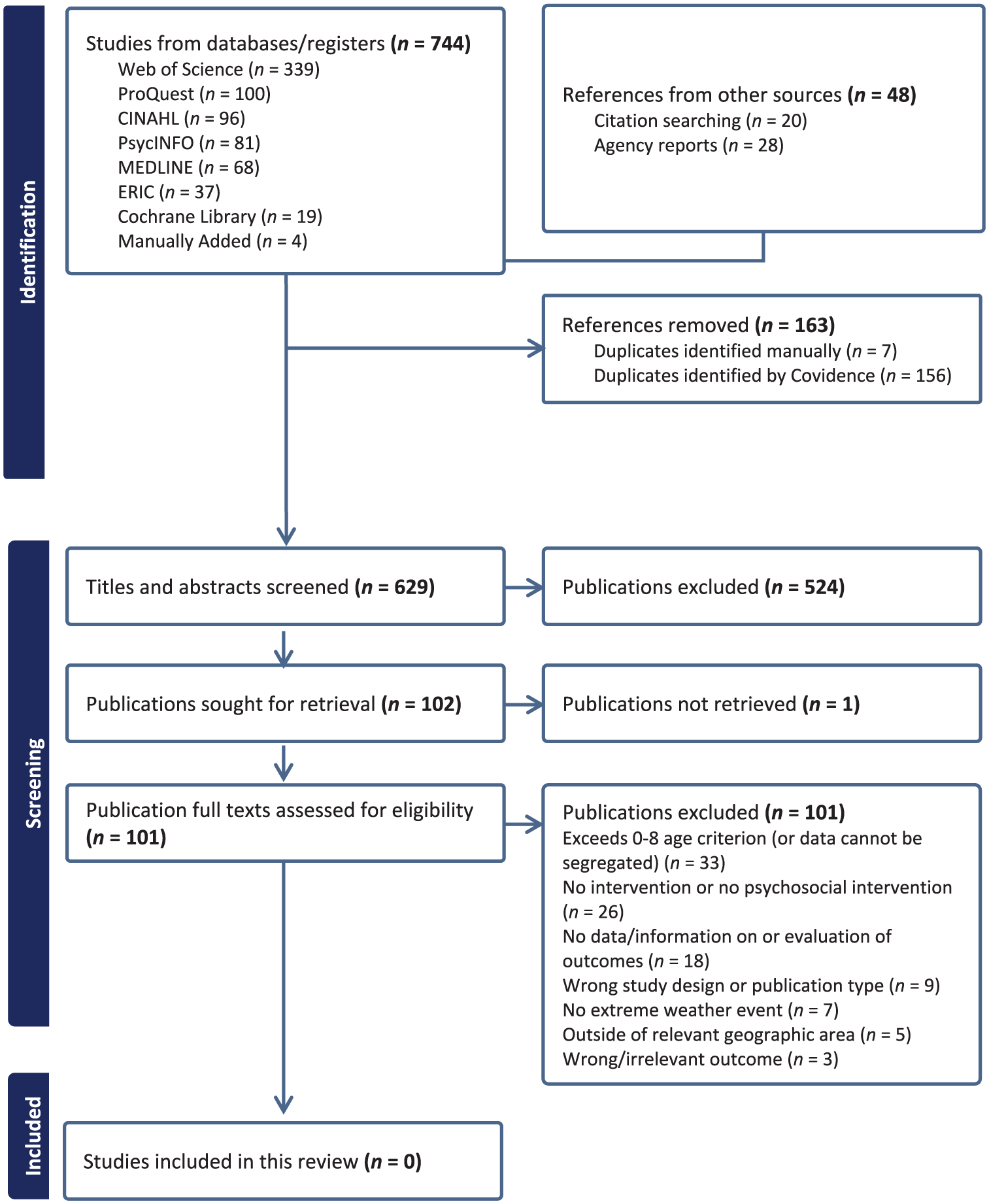
PRISMA flow diagram
Discussion
Our systematic review aimed to identify and evaluate the impact of psychosocial interventions that promote early childhood development, mental health or mental wellbeing in post-EWE settings within LMICs. No studies met our inclusion criteria. Despite our thorough search strategy, encompassing both peer-reviewed and grey literature and considering diverse study designs, our systematic review is an ‘empty review’. This finding suggests that there is either a genuine absence of such interventions, or that evaluations of such programmes have not been made publicly available. More than a lack of evidence, this represents a critical paucity and calls for urgent action.
This evidence gap is exacerbated by a broader lack of studies examining the associations between EWEs and ECD outcomes with only a few studies focusing on this age group or providing age-disaggregated data. This finding is congruent with reviews on climate change-related topics 93 and mental health and psychosocial support in LMICs 89 that highlight ECD as the most under-researched area in global mental health and reflects a broader shortage of clinical guidance for early childhood support in humanitarian settings. 1
The lack of documented interventions from LMICs may reflect a genuine absence of such interventions, but could also be due to barriers in evaluation, dissemination, and publication, 94 especially in humanitarian contexts. In some situations, immediate survival needs may take precedence and leave limited capacity or resources for psychosocial programming for young children. Alternatively, where programmes do exist, challenges such as funding, research capacity, and difficulties in conducting evaluations may impede the ability to generate robust evidence. Furthermore, publication-related obstacles, such as English language and peer review standards, and biases against negative or null results, contribute to persistent evidence gaps.62,95–97 Importantly, these challenges are situated within a broader oversight of child and adolescent mental healthcare and interventions in LMICs. 98
The dearth of evaluations also means a lack of evidence on the barriers, facilitators, and unique mechanisms linking EWEs with early childhood development and wellbeing in LMICs. Comprehensive evidence on associations and underlying mechanisms is essential to identify intervention targets and develop effective interventions. 99 Programmes with demonstrated benefits for young children in other humanitarian and disaster settings include those involving parents or caregivers, 100 physical touch, 101 nurturing care, 102 stimulation, 103 or baby-friendly spaces. 104 These approaches should be rigorously evaluated to establish their effectiveness in post-EWE contexts. 105
Given that climate change is the foremost global health challenge,106–108 neglecting ECD compromises the long-term wellbeing of vulnerable individuals. Existing literature that connects unaddressed childhood adversity with significant and long-term physiological and psychological consequences109–111 suggests that similar impacts are likely to result from adversity and trauma caused by EWEs. This neglect of early childhood research and interventions undermines progress in global health 18 and incurs substantial economic costs due to poor health outcomes.83,107,112,113 Furthermore, this shortfall indicates that Sustainable Development Goals 3 and 13 (ensure healthy lives and promote wellbeing for all at all ages and take urgent action to combat climate change and its impacts respectively) 114 are not being addressed comprehensively. This evidence gap points to the urgent need for coordinated, systematic research and strategic investment in early childhood interventions in LMICs facing EWEs, along with a commitment to transparent reporting.
Despite robust theoretical frameworks advocating for ECD in contexts prone to disadvantage, adversity, or trauma, their real-world application and evaluation in post-EWE contexts remain limited. This disconnect impedes the ability to align practical efforts with theoretical insights, whereas evidence of impact, or a lack thereof, is essential for promoting more evidence-based humanitarian efforts.95,96 Nevertheless, literature reviewed herein provides clear guidance for interventions: timed within the first 1000 days, delivered with or through caregivers, and across multiple levels. The established importance of early childhood means interventions in this period can yield substantial and enduring benefits. Moreover, evidence consistently identifies parenting and the caregiving environment as central influences. Therefore, programmes that strengthen caregiver mental health, promote responsive and nurturing parent-child relationships, and provide stable routines are likely to support child recovery and resilience. Furthermore, frameworks such as that proposed by Cuartas et al. emphasise the need to reinforce broader environmental supports across family, community, service, and policy levels to address both acute shocks and cumulative, chronic stressors. Even in the absence of direct evaluation data, these avenues offer an evidence-informed base for future efforts.
In light of the above, we encourage research and policy efforts to focus on developing, implementing, and evaluating psychosocial interventions to foster development, mental health and wellbeing in early childhood, especially in post-EWE settings within LMICs. While it is likely that work is being done on the ground, the lack of accessible research is a disservice to the children, parents, and wider communities living in LMICs who could benefit from such support. Therefore, intervention developers and providers should commit to open science and ensure that interventions are not only robustly evaluated but also shared widely and transparently. This will ensure that the findings are accessible to both academic and humanitarian sectors, and that evidence syntheses are more comprehensive, conclusive, and beneficial. Finally, this gap signals an opportunity for donor agencies to support the development, adaptation, and evaluation of interventions combining ECD with post-EWE humanitarian efforts. Policymakers should prioritise the vulnerability of children during the first 1000 days and ensure that multisectoral interventions are embedded in national agendas. 115 Climate resilience programming must also address the needs of pregnant women, newborns, and young children. 105 There is also a strong rationale for incorporating ECD and mental health supports with sectors already prioritised in humanitarian settings such as Water, Sanitation and Hygiene (WASH), Maternal, Newborn and Child Health (MNCH), and Mental Health and Psychosocial Support. 4 Following Cuartas et al.’s recommendations, 13 this integrated approach will allow stakeholders to leverage existing resources, reputation, and reach to deliver interventions that are multi-level, comprehensive, and tailored to the needs of the most vulnerable.
Strengths and limitations
This review’s strength lies in its expansive and comprehensive search procedures, including the number of databases searched. However, even with a rigorous review process, there is a risk of missing relevant studies; we attempted to minimise this by designing a comprehensive and inclusive search strategy. Nonetheless, the following limitations necessitate consideration: first, our focus on English-language sources limits the coverage of our review by excluding relevant studies published in other languages. Second, we focused exclusively on post-EWE exposure interventions, which may have excluded preventive measures (such as caregiver preparedness or vulnerability reduction prior to climate-related disasters). Third, our review focused on early childhood psychosocial interventions while acknowledging that immediate disaster recovery efforts primarily focus on addressing basic needs such as safety, shelter, nutrition, and healthcare.116,117 To account for this, we applied a 12-month criterion to allow time for recovery efforts and programming to expand beyond basic needs. Fourth, we excluded studies that did not specify participant ages or that included children over the age of 8 years but data could not be segregated by age. While this method may have led to the exclusion of relevant articles, it was necessary to ensure the specific developmental age group of early childhood was captured in this review. Future research may include a comparator research question incorporating older children as this can extend the evidence base and support the application of post-EWE psychosocial interventions beyond the early childhood period. Finally, our focus was limited to acute climate-related disasters, and excluded slower-onset or chronic climate conditions which may also disrupt children’s environments and developmental experiences 118 but fall outside the scope of this review. Nevertheless, the focused nature of our search ensured relevance while also underscoring an alarming gap in available literature on psychosocial interventions in post-extreme weather event settings for this specific age group.
Conclusion
This review found no evaluations of psychosocial interventions for young children in post-extreme weather event settings. This lack of evaluation is a clear gap for humanitarian programming and policy efforts and highlights the need for more research about and for early childhood in post-EWE settings. Addressing these gaps is essential for supporting early childhood development and wellbeing in LMICs affected by EWEs. Effective approaches should be developed, evaluated, and shared widely. The climate crisis is a child’s rights crisis, and we owe it to future generations to prioritise their needs and wellbeing to ensure they can thrive, lead healthy lives, and realise their full potential even in the face of these threats. As the climate crisis intensifies and exposes more children to these events, the need for robust evidence-based strategies is increasingly urgent. Prioritising children’s rights and wellbeing in this context will not only advance academic understanding but also directly benefit vulnerable children, families, and communities worldwide.
Supplemental Material
sj-docx-1-rsh-10.1177_17579139251371589 – Supplemental material for A review of early childhood psychosocial interventions following extreme weather events in low- and middle-income countries
Supplemental material, sj-docx-1-rsh-10.1177_17579139251371589 for A review of early childhood psychosocial interventions following extreme weather events in low- and middle-income countries by TN Akhtar, N Maiorano, A Cosma and K Hadfield in Perspectives in Public Health
Supplemental Material
sj-docx-2-rsh-10.1177_17579139251371589 – Supplemental material for A review of early childhood psychosocial interventions following extreme weather events in low- and middle-income countries
Supplemental material, sj-docx-2-rsh-10.1177_17579139251371589 for A review of early childhood psychosocial interventions following extreme weather events in low- and middle-income countries by TN Akhtar, N Maiorano, A Cosma and K Hadfield in Perspectives in Public Health
Footnotes
Acknowledgements
The authors would like to express their gratitude to Ms Geraldine Fitzgerald, the subject librarian at the School of Psychology, Trinity College Dublin, for her expert contributions to this review’s search strategy and procedures.
Author Contributions (Credit)
Conflict Of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: TNA is a recipient of the Trinity Research Doctorate Award by Trinity College Dublin that supports her PhD research. The funder has no involvement in the design or findings of this review.
Ethics Approval
Not required.
Consent To Participate
Not applicable.
Consent For Publication
Not applicable.
Data Availability
A search string is available as Supplementary Information. Additional strategies are available upon request. All excluded publications are also available as Supplementary Information.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.