
Abstract
Objectives
We examined associations between extreme weather events (EWE), resource insecurities, and HIV vulnerabilities among a purposive sample of adolescent girls and young women (AGYW) aged 16 to 24 in Nairobi and Kisumu, Kenya.
Methods
We conducted multivariable logistic/linear regression on cross-sectional survey data to assess associations between EWE exposure, food insecurity (FI), water insecurity (WI), and sanitation insecurity (SI) with HIV vulnerabilities (transactional sex [TS], intimate partner violence [IPV], sexual relationship power [SRP], and preexposure prophylaxis [PrEP] awareness and acceptability).
Results
Among participants (n = 597; mean age: 20.13 years; standard deviation = 2.5), in adjusted analyses, SI and WI were associated with increased TS. Increased cumulative EWEs and eco-anxiety were associated with increased IPV. EWE frequency, FI, and SI were associated with reduced SRP. EWE frequency and SI were associated with reduced, and WI with increased, PrEP awareness. EWE frequency and SI were associated with PrEP acceptability.
Conclusion
Resource scarcities and EWEs were associated with HIV vulnerabilities and PrEP acceptability among AGYW.
Plain Lanugage Summary
What is the issue we addressed? There is increased focus on relationships between extreme weather events (EWE), resource scarcities, and HIV vulnerabilities, yet this is understudied in adolescent girls and young women (AGYW).
What did we do? We examined associations between these factors among AGYW in Nairobi and Kisumu, Kenya. We collected cross-sectional data (April-June 2024) with AGYW aged 16-24 years in Nairobi and Kisumu. We conducted analyses to examine associations between socio-demographics, resource insecurities (food, water, sanitation), and EWE (past-year EWE types and frequency, eco-anxiety) with HIV vulnerabilities (past 12-month transactional sex; past 12-month intimate partner violence; low sexual relationship power) and biomedical HIV prevention outcomes (pre-exposure prophylaxis [PrEP] awareness, use, and acceptability).
What did we find? There were 597 participants (the mean age was 20.13 years; standard deviation=2.5). Our findings showed that sanitation insecurity and water insecurity were associated with increased transactional sex odds. Increased number of past-year EWE and eco-anxiety were associated with higher intimate partner violence odds. Food insecurity, sanitation insecurity, and increased EWE frequency, were associated with reduced sexual relationship power. Sanitation insecurity and increased EWE frequency were associated with reduced PrEP, and water insecurity with increased, PrEP awareness. Sanitation insecurity and increased EWE frequency were associated with PrEP acceptability.
What does this mean? Resource scarcities and EWE were associated with HIV vulnerabilities as well as PrEP acceptability among AGYW. Future climate-informed HIV prevention research can integrate EWE and resource insecurity-related priorities.
Introduction
Regions most severely impacted by climate change and extreme weather events (EWEs) are also disproportionately affected by HIV.1,2 Recent evidence reviews have conceptualized potential pathways linking EWEs to HIV vulnerabilities and poorer HIV prevention outcomes, including via increased poverty, transactional sex (TS), sexual and gender-based violence (SGBV), and disrupted healthcare access.3–5 Among adolescents aged 10 to 24 years in Sub-Saharan Africa (SSA), HIV prevalence among girls is over three-fold higher than among their male counterparts.6,7 Yet knowledge gaps persist regarding pathways from EWEs to HIV vulnerabilities among adolescent girls and young women (AGYW) in climate- and HIV-affected contexts such as Kenya.
Drought is associated with increased HIV prevalence among women in multiple SSA countries.8–11 It contributes to food and water insecurity (WI), 12 which increases engagement in sexual practices10,12 such as TS10,13 and reduced condom use. 14 Similarly, a study in 21 SSA countries 15 found that heavy rainfall was associated with elevated HIV and STI infection risks, potentially due to food insecurity (FI)-related TS and reduced healthcare access.
Kenya is an important context to examine EWEs and HIV vulnerabilities among AGYW. The country's adult HIV prevalence rate is 3.2%, 16 and in 2023, 38% of new adult infections occurred among youth aged 15 to 24. 6 Kenyan youth face sexual health challenges including SGBV and early pregnancy,17–19 and climate change may be associated with increased gender inequities. 20 Kenya is experiencing increasingly frequent and severe EWEs21,22 as part of broader cyclical climate shocks affecting the Horn of Africa. 23 These have included severe rains and floods in 2019 to 2020, a prolonged drought from 2020 to 2023, and a return to widespread flooding in 2023 to 2024. 23
The nexus of EWEs, resource insecurity, and HIV vulnerabilities is understudied with AGYW in Kenya. To address this knowledge gap, we examined associations between EWEs, resource insecurities (food, water, sanitation), and HIV vulnerabilities and biomedical HIV prevention outcomes among AGYW in Nairobi and Kisumu, Kenya.
Methods
Study Setting and Design
We analyzed baseline data collected in April to June 2024 in the context of the cohort study (“Rada ya Weather” [“what's up with the weather” in Swahili) with AGYW aged 16 to 24 in two climate-affected 21 and HIV-affected locations: 24 Nairobi informal settlements (Majengo, Mathare) and Kisumu fishing communities (rural and periurban communities along Ogal and Rota Beaches). Nairobi's informal settlements, 25 and Kisumu, located along with Lake Victoria, are affected by EWEs such as heavy rainfall, flooding, drought, and heatwaves.26,27 Nairobi's HIV prevalence of 5.6% for women aged 15 and older, and Kisumu's HIV prevalence of 18.7% for women, 24 are higher than Kenya's national prevalence of 4.3% among women. 16
We conducted purposive sampling with recruitment conducted by 16 AGYW peer navigators aged 16 to 24 in each study location, including in-person outreach with study coupons, word-of-mouth, social media, and venue-based recruitment at community agencies/clinics. 28 Eligibility criteria: living in Nairobi (Mathare, Majengo) or Kisumu fishing communities (periurban/rural); aged 16 to 24; self-identified woman; owned/had access to a mobile phone; self-reported HIV-negative serostatus at baseline; experienced ≥1 resource insecurity (food, water, and/or sanitation) and/or EWE (eg, flood, drought) in the past 14 days; reported any HIV vulnerability in the past 14 days (eg, young motherhood, TS, intimate partner violence [IPV], condomless sex, multiple sex partners); able to speak English, Swahili, or Luo; and able to provide informed consent. Additional inclusion criteria in Kisumu were engagement with the fishing industry (eg, buying, selling, cleaning), and in Nairobi were motherhood, due to the high HIV acquisition risks experienced in Kenya's fishing industry 29 and by young mothers in East and South Africa. 30
We used SurveyCTO, 31 a secure, multilingual tablet-based application for trained data collectors to conduct survey interviews at community-based partner agencies. Prior to implementation, we pilot tested the survey tool (Supplemental File 1) with peer navigators, data collectors, and local collaborators and translated survey and consent documents into Swahili and Luo. We aimed to collect data from a cohort study of n = 500 to fulfill sample size requirements for advanced statistical analyses (eg, latent class analyses),32,33 longitudinal analyses with future data collection timepoints, and analyses stratified by location. 34
Research ethics board approval was received from the University of Toronto, Amref Ethics and Scientific Review Committee (Kenya), and the National Commission for Science, Technology and Innovation (Kenya) (NACOSTI). All participants provided written informed consent prior to study enrollment.
Measurement
EWE and resource insecurity exposure variables: Based on past research,35–39 we designed context-specific questions to assess EWE exposure. Participants were first asked to report if they had experienced any EWE in the past 12 months with a range of response options which were summed and categorized (1 EWE; 2-5 EWE, ≥5 EWE). Past-year EWE frequency was then assessed with the question “Have you faced any of the weather event(s) more than once in the past year?” using response options: “1 type of EWE, once in last year,” “1 type of EWE, >once in last year,” “>1 type of EWE, all only once in the last year,” and “>1 EWE, at least 1 >once in last year.” We assessed EWE-related anxiety with the Hogg Eco-Anxiety Scale 40 (Cronbach's alpha = 0.90). We assessed past 4-week WI (Household Water Insecurity Experiences scale) 41 (Cronbach's alpha = 0.92); past 4-week FI (Household Food Insecurity Access Scale) 42 (Cronbach's alpha = 0.90); and past 30-day sanitation insecurity (SI) (Sanitation Insecurity Scale) 43 (Cronbach's alpha = 0.94). We also assessed sociodemographic variables (eg, gender, age, education level, relationship status, young motherhood).
HIV vulnerability outcomes: Past 12-month TS (sex in exchange for money or resources) was assessed using a single binary item (yes/no) developed for this study. Past-year physical, sexual, or emotional/control IPV was assessed using 8 items from the World Health Organization abuse scale 44 (Cronbach's alpha = 0.88). Sexual relationship power (SRP) was assessed with the 15-item Relationship Control subscale from the Sexual Relationship Power Scale. 45 (Cronbach's alpha = 0.89).
Biomedical HIV prevention outcomes: Preexposure prophylaxis (PrEP)-related questions were developed specifically for this study. Preexposure prophylaxis awareness was assessed as a binary outcome (yes/no), and lifetime (ever) use was dichotomized into two categories: “never used” versus “lifetime use” that combines previous PrEP use (past use, but not current use) and current use. There was an insufficient sample size currently using PrEP to include as a separate outcome in analyses. Preexposure prophylaxis acceptability (willingness to use PrEP in the future) was assessed among participants who had never used PrEP. 46 Response options included: definitely yes, probably yes, maybe, probably no, and definitely no. For analysis, responses were categorized as binary: yes (definitely yes and probably yes) and no (maybe, probably no, and definitely no).
Statistical Analysis
We calculated descriptive statistics, including means and standard deviations for continuous variables and proportions for categorical variables. To compare differences between the two study locations, we used χ2 tests for categorical variables and independent samples t tests for continuous variables. Binary logistic regression was used for binary outcome variables such TS, PrEP awareness, PrEP uptake, recent IPV experience, and PrEP acceptability, while linear regression was used for continuous outcomes such as SRP. We first conducted univariable analyses, adjusting for study location, to examine associations between each independent variable and the outcome. Variables with a P-value ≤.20 in the univariable models were considered for inclusion in the multivariable models. Final multivariable models were further refined using backward stepwise regression, with variables removed sequentially if their P value exceeded 0.10, and retained if P ≤ .05. 47 The selection process was guided by significance levels and overall model fit, evaluated using the Akaike Information Criterion and adjusted R-squared (for linear models) or Pseudo R-squared (for logistic models). All models were additionally adjusted for study location to account for potential confounding.
Statistical analyses were two-tailed, with a significance level of P < .05, and we report adjusted odds ratios (aORs) or beta coefficient (aβ) with 95% confidence intervals (CIs). We conducted sensitivity analyses stratified by location. As there were no significant outcome differences by location, we present findings combined across locations. Data were analyzed using Stata version 18.0 (StataCorp). The reporting of this study adheres to the STROBE guidelines for reporting observational studies 48 (Supplemental File 2).
Results
Among participants (n = 597; mean age: 20.13 years; standard deviation [SD] = 2.5), most reported experiencing multiple past-year EWE types; 16.2% (n = 97) reported one type of past-year EWE, approximately half (51.9%; n = 310) encountered 2 to 4 types, and nearly one-third (31.8%; n = 190) reported ≥5 types (see Table 1).
Baseline Characteristics of Rada Ya Weather Study Participants in Kisumu and Nairobi, Kenya by Study Location (n = 597).

Abbreviation: PrEP, preexposure prophylaxis.
Findings are reported below and in Table 2.
Multivariate Analysis for Factors Associated With HIV Vulnerability and Prevention Outcomes Among Adolescent Girls and Young Women Participants in the Rada Ya Weather Cohort Study in Nairobi and Kisumu, Kenya (N = 597).
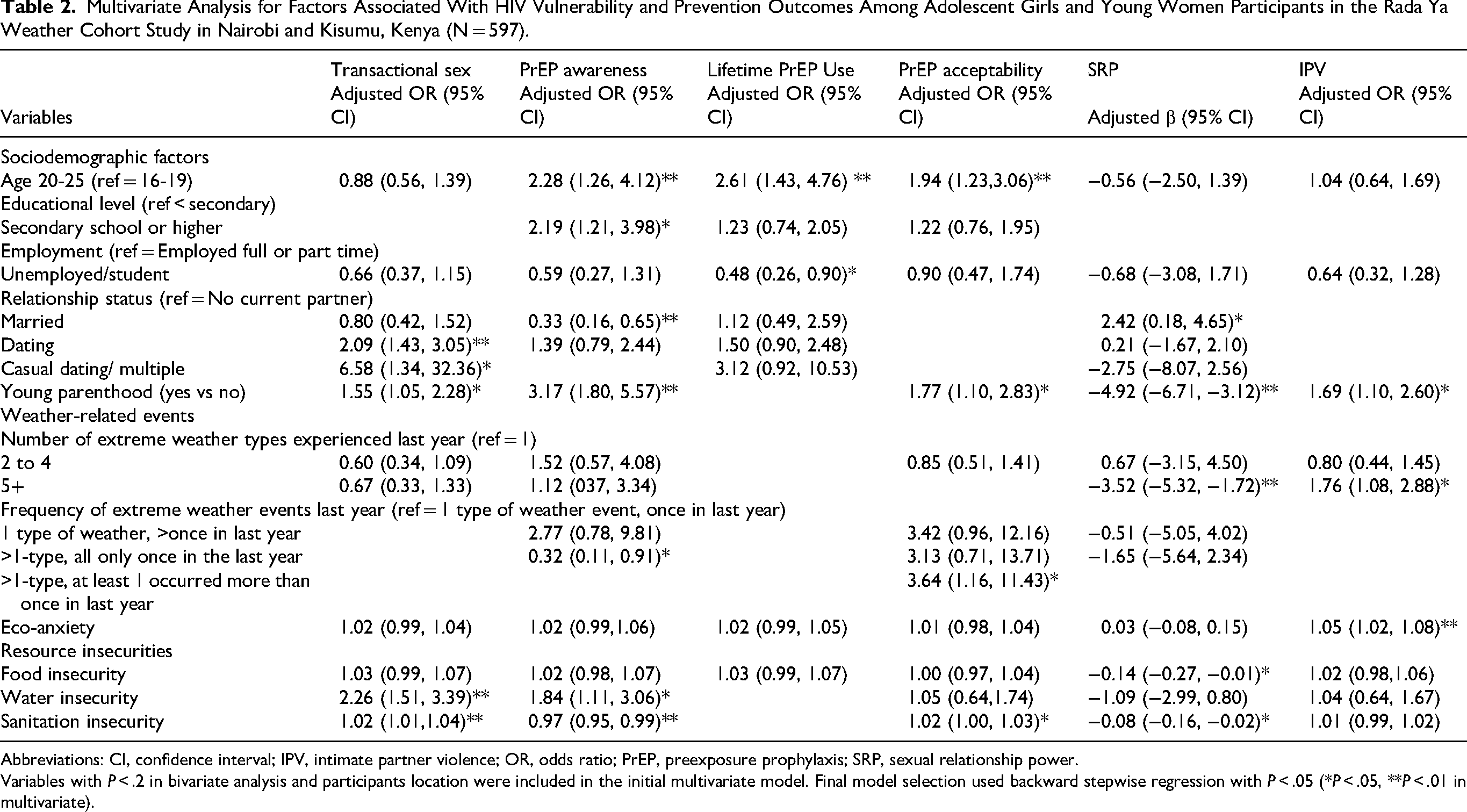
Abbreviations: CI, confidence interval; IPV, intimate partner violence; OR, odds ratio; PrEP, preexposure prophylaxis; SRP, sexual relationship power.
Variables with P < .2 in bivariate analysis and participants location were included in the initial multivariate model. Final model selection used backward stepwise regression with P < .05 (*P < .05, **P < .01 in multivariate).
Past 12-month TS: Relationship status (dating vs single: aOR = 2.09, 95% CI: 1.43-3.05, P < .001; casual dating/multiple partners vs single: aOR = 6.58, 95% CI: 1.34-32.36), P = .021) was associated with increased odds of recent TS, as was motherhood (aOR = 1.55, 95% CI: 1.05-2.28, P = .028). Water insecurity (aOR = 2.26, 95% CI: 1.51-3.39, P < .001) and SI (aOR = 1.02, 95% CI: 1.01-1.04, P = .002) were associated with higher odds of recent TS.
Past 12-month IPV: Motherhood (aOR = 1.69, 95% CI: 1.10-2.60, P = .015) was associated with higher recent IPV odds. Higher number of EWE types (≥5 vs 1) (aOR = 1.76, 95% CI: 1.08-2.88, P = .024) and eco-anxiety (aβ = 1.05, 95% CI: 1.02-1.08) were associated with increased likelihood of recent IPV.
Sexual relationship power: Relationship status (married vs no current partner) was associated with higher SRP (aβ = 2.42, 95% CI: 0.18-4.65, P = .034), while motherhood was associated with reduced SRP (aβ = −4.92, 95% CI: −6.71 to −3.12, P < .001). Food insecurity (aβ = −0.14, 95% CI: −0.27 to −0.01, P = .042), SI (aβ = −0.08, 95% CI: −0.16 to −0.02, P = .014), and EWE frequency (≥5 vs 1) (aβ = −3.52, 95% CI: −5.32 to −1.72, P < .001), were associated with lower SRP.
Preexposure prophylaxis awareness, lifetime use, and acceptability: In adjusted analyses, older age (20-25 years vs 16-19 years) (aOR = 2.28, 95% CI: 1.26-4.12, P = .007), higher education (>secondary school vs <secondary school) (aOR = 2.19, 95% CI: 1.21-3.98, P < .010), and motherhood (aOR = 3.17, 95% CI: 1.80-5.57, P < .001) were associated with higher odds of PrEP awareness, while relationship status (married vs no current partner) (aOR = 0.33, 95% CI: 0.16-0.65, P = .002) was associated with reduced PrEP awareness. Sanitation insecurity (aOR = 0.97, 95% CI: 0.95-0.99, P = .002) and increased EWE frequency (>1 EWE type vs 1) (aOR = 0.32, 95% CI: 0.11-0.91, P = .032) were associated with lower odds of PrEP awareness. Water insecurity was associated with increased odds of PrEP awareness (aOR: 1.84, 95% CI: 1.11-3.06, P < .05). Older age (20-25 years vs 16-19 years) (aOR = 2.61, 95% CI: 1.43-4.76, P < .001) was associated with higher, and unemployment with reduced (aOR = 0.48, 95% CI: 0.26-0.90, P = .024), odds of lifetime PrEP use.
Factors associated with increased likelihood of PrEP acceptability included: older age (20-25 years vs 16-19 years) (aOR = 1.94, 95% CI: 1.23-3.06, P = .004); motherhood (aOR = 1.77, 95% CI: 1.10-2.83, P = .018); increased EWE frequency (>1 vs 1) (aOR: 3.64, 95% CI: 1.16-11.43, P < .05); and SI (aOR: 1.02, 95% CI: 1.00-1.03, P < .05).
Discussion
Among this sample of AGYW in Kenya, sociodemographic, weather, and resource insecurity-related factors were associated with relational-level HIV vulnerabilities49–51 and lower biomedical HIV prevention awareness. Yet EWEs and resource insecurities were also associated with increased willingness to take PrEP, signalling opportunities for engaging climate-affected AGYW in the HIV prevention cascade.52,53 Our findings underscore the importance of examining relational-level factors as pathways connecting EWEs, resource insecurities, and HIV prevention outcomes.52,53 Preexposure prophylaxis is understudied in relation to EWEs, and our findings point to the need to increase access for AGYW in climate-affected Kenyan contexts. Our study also indicates the importance of assessing multiple EWE types and frequencies to assess cumulative exposure and associated HIV vulnerabilities.
Our findings align with evidence that drought and WI are associated with TS3,8,10,13 and also show the importance of examining SI and TS. The concept of SI43,54 is understudied in relationship to HIV, and our findings signal the need for additional research. While we found associations between EWEs and lower SRP, and EWEs are linked with increased SGBV55–57 and gender inequities, 57 scant research has looked at EWEs and SRP. Our finding that FI is associated with reduced SRP aligns with youth research in Uganda 13 and Kenya 58 whereby unmet basic needs can reduce sexual agency and SRP. We identify SI as another important consideration for SRP. We found EWE associated with recent IPV, aligning with growing evidence on EWEs and IPV risks55–57 possibly due to exacerbated household stressors and inequitable gender norms. We found eco-anxiety—mental distress due to deteriorating environmental conditions59,60—associated with IPV; it is likely that relationships between EWEs and household-level stressors that exacerbate IPV55–57 are bidirectional. This warrants further investigation.
To date, PrEP is understudied in EWE and resource insecurity research. 3 Our findings that EWEs and SI were associated with reduced PrEP awareness align with prior findings that EWEs can disrupt HIV service delivery.3,61–63 Higher PrEP acceptability among EWE- and resource insecurity-affected AGYW may signal higher risk perceptions and in turn motivation for prevention engagement. 53 Water insecurity was associated with increased, and SI with decreased, PrEP awareness; the potentially different lived experiences of resource insecurities64,65 warrant further exploration. While young mothers were more likely to report PrEP awareness and acceptance, there were no lifetime PrEP use differences by motherhood status. This signals an important intervention target. 30
Study limitations include a nonrandom sample, limiting generalizability; a cross-sectional design, limiting the ability to determine causality; and self-reported outcomes, introducing potential bias. Our sample was limited to those who had experienced some EWEs and HIV vulnerability, which reduced variability and may have reduced power. Despite these limitations, our study is unique in identifying shared findings across two different climate-affected locations and two different HIV-affected AGYW populations in Kenya. Together, our findings highlight the importance of assessing EWEs alongside multiple material need insecurities in HIV prevention research with AGYW in climate-affected Kenyan regions.
Supplemental Material
sj-pdf-1-jia-10.1177_23259582251362938 - Supplemental material for Associations Between Extreme Weather Events and Resource Insecurities With HIV Vulnerabilities and Biomedical HIV Prevention Outcomes Among Adolescent Girls and Young Women in Kenya: A Cross-Sectional Analysis
Supplemental material, sj-pdf-1-jia-10.1177_23259582251362938 for Associations Between Extreme Weather Events and Resource Insecurities With HIV Vulnerabilities and Biomedical HIV Prevention Outcomes Among Adolescent Girls and Young Women in Kenya: A Cross-Sectional Analysis by Carmen H Logie, Zerihun Admassu, Aryssa Hasham, Humphres Evelia, Julia Kagunda, Beldine Omondi, Clara Gachoki, Mercy Chege, Lesley Gittings, Caetano Dorea, Janet M Turan, Mumbi Mwangi and Lawrence Mbuagbaw in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-doc-2-jia-10.1177_23259582251362938 - Supplemental material for Associations Between Extreme Weather Events and Resource Insecurities With HIV Vulnerabilities and Biomedical HIV Prevention Outcomes Among Adolescent Girls and Young Women in Kenya: A Cross-Sectional Analysis
Supplemental material, sj-doc-2-jia-10.1177_23259582251362938 for Associations Between Extreme Weather Events and Resource Insecurities With HIV Vulnerabilities and Biomedical HIV Prevention Outcomes Among Adolescent Girls and Young Women in Kenya: A Cross-Sectional Analysis by Carmen H Logie, Zerihun Admassu, Aryssa Hasham, Humphres Evelia, Julia Kagunda, Beldine Omondi, Clara Gachoki, Mercy Chege, Lesley Gittings, Caetano Dorea, Janet M Turan, Mumbi Mwangi and Lawrence Mbuagbaw in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
The authors would like to acknowledge all of the participants, research team, and support from the Centre for the Study of Adolescence and Elim Trust in Nairobi, Kenya.
Ethical Considerations
Research ethics board approval was received from the University of Toronto (Canada) (43514), Amref Ethics and Scientific Review Committee (Kenya) (ESRC P1408/2023), and the National Commission for Science, Technology and Innovation (Kenya) (NACOSTI) (NACOSTI/P/23/30358).
Consent to Participate
All participants provided written informed consent prior to study enrollment.
Author Contributions
Study design: CHL, LM, HE, JK, and CD. Data collection: HE, JK, BO, CG, MC, and MM. Data management and analysis: CHL, ZA, AH, JK, HE, BO, and CG. Manuscript writing: CHL, ZA, and AH. Manuscript editing and critical review: CHL, ZA, AH, HE, JK, BO, CG, MC, LG, CD, JMT, MM, and LM.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canada Research Chairs (Tier 2: Logie), New Frontiers in Research Fund (NFRFR-2021-00192), Canadian Institutes of Health Research (CIHR) Project Grant (Institute of Gender and Health) (202109PJT-468896-GSH-CEAA-187455), and the Social Sciences and Humanities Research Council of Canada (SSHRC) (PDG: 880-2020-080).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data will be shared upon reasonable request and obtaining required ethics approvals to corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.