
Abstract
Aim:
This study aims to establish whether digital surveillance methods for notifiable diseases in Australia collect and report data in relation to marginalised populations.
Methods:
The literature was systematically reviewed to identify primary research studies published between January 2005 and July 2023. Studies were included if they described an Australian digital surveillance system for notifiable conditions. The results were synthesised with a focus on evaluating the collection and reporting of data in relation to marginalised populations.
Results:
A total of 13 articles reporting on seven surveillance systems were identified. Influenza and adverse events following immunisation were the two most common notifiable conditions monitored. A total of six surveillance systems encompassing 16 articles reported information on sub-populations. Of these, three surveillance systems (nine articles) included data on marginalised populations.
Conclusion:
The data collected or reported in relation to sub-groups that characterise diversity in terms of health care needs, access, and marginalised populations are minimal. It is recommended that a set of equity and reporting principles is established for the future creation and use of any digital surveillance system.
Introduction
Infectious diseases create significant health and economic burden globally including Australia, as highlighted by the COVID-19 pandemic. As of July 2023, there have been over 11.5 million cases and over 20,000 deaths in Australia due to the novel coronavirus. 1 In addition to COVID-19, three other diseases accounted for the vast majority of Australia’s notifiable disease reports in 2022: influenza with 233,369 notifications, respiratory syncytial virus with 95,776 notifications, and chlamydia with 94,222 notifications. 2 Prior to the pandemic, annual expenditure on all infectious diseases in Australia was reported as roughly $7.52 billion. 3 In 2021, the Australian government spent $7.9 billion on specific COVID-19 health programmes alone. 4
Timely and comprehensive surveillance of infectious diseases is essential for targeted public health response and prevention efforts. Currently, infectious diseases are monitored in Australia via the National Notifiable Diseases Surveillance System (NNDSS). 5 Over 70 conditions are legally required to be reported to this system by doctors and laboratories, encompassing gastrointestinal diseases, sexually transmissible infections and blood-borne viruses (BBVs), respiratory diseases, vaccine-preventable diseases, zoonoses, vector-borne diseases, and other diseases.2,5 There are also a number of other surveillance systems within Australia which collect additional data to enhance public health response, such as the New South Wales (NSW) Public Health Rapid, Emergency, Disease, and Syndromic Surveillance system which monitors unplanned visits to emergency departments and emergency triple zero calls (000), to detect any unusual emerging patterns in syndromes often related to infectious pathogens. 6
Recently, novel methods of surveillance utilising digital technologies have emerged to complement existing methods of surveillance. This includes the use of monitoring social media data,7–9 and Google trends with machine learning methods,9,10 as well as the use of electronic medical records, 11 to predict disease outbreaks. Surveillance using these types of data provides benefits over traditional data sources in that they are generally publicly available and early work has shown they can provide timelier detection of some disease outbreaks. 9
Analysis of global data has clearly linked poverty, inequality, marginalisation, and other barriers to healthcare with infectious disease burden.12,13 If implemented inequitably, digital health technologies can further increase health disparities in marginalised populations.14,15 This has been shown in Black communities across North America, UK, and Italy due to limited application of eHealth initiatives, and for those who live in rural areas due to limited access as a result of restricted Internet broadband coverage. 15 Being an older adult (over the age of 40 years), having low income, and having low levels of education have also been identified as barriers to acquiring and understanding how to use digital health technologies. 15 With the continuing adoption of digital health systems into Australian public health, the importance of limiting the disparity in marginalised populations such as Aboriginal and Torres Strait Islander people, elderly populations, and culturally and linguistically diverse (CALD) populations is evident. As there is very limited research on this in Australia, this study aims to establish whether digital surveillance methods for notifiable diseases in Australia collect and report data in relation to marginalised populations which will establish a benchmark and enable future assessment of whether these technologies improve health or create further marginalisation.
Methods
Search strategy
The methods used in this review were developed in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 16 The initial search of peer-reviewed published literature was conducted in PubMed (Medline), EMBASE, and CINAHL in January 2022. A secondary search of the literature was conducted on the 13th of June 2023 to identify additional studies published after January 2022. Initial search terms included digital health, surveillance, communicable diseases, and Australia. ‘SARS-CoV-2’[Mesh] and ‘COVID-19’[Mesh] were added to the secondary search. The full search strategy is available in Supplemental Appendix 1. All reference lists of all eligible studies were checked for additional studies for inclusion.
Inclusion and exclusion criteria
Studies were included if they met the following criteria:
Described an Australian digital surveillance system, defined as systems which utilised data from social network sites (e.g. Facebook), content sharing websites (e.g. YouTube), search data (e.g. Google), blogs and forums (e.g. Reddit) and digital polls, or studies that utilised novel methods of digital analysis, specifically machine learning methods.
Notifiable conditions were defined as any condition reportable to the NNDSS. 5
Full-text articles in English language.
Were published between January 2005 and July2023.
Studies were excluded if they met the following criteria:
Surveillance was specific to a population group (i.e. healthcare workers).
Described the methods of the system only, without reporting results.
Compared the surveillance system to another system or evaluated the system without reporting results of the surveillance system.
Screening
The titles and abstracts of articles identified through the search were extracted and uploaded to the systematic review software Covidence. Two authors (AD and ND) independently screened the titles and abstracts. The same authors reviewed full-text articles to assess their eligibility against the inclusion criteria. Reference lists from all included studies were examined to identify additional eligible studies. Any conflicts were resolved through discussion and consensus between the authors.
Data extraction and synthesis
Extraction of data was completed by one author (NDK) and cross-checked by a second author (AD) using a standard extraction form. Fields extracted included condition under surveillance, data used, study period, objective, location, sample size, overall results, study design, recruitment methods, and if any data were reported on subpopulation as well as marginalised populations specifically. Information regarding data or trends in marginalised populations was a key field for extraction to allow for an overall assessment of the equity of digital surveillance systems. Marginalised populations were defined as ‘highly vulnerable populations that are systemically excluded from national or international policy making forums’. 17 This includes, but is not limited to, Aboriginal and Torres Strait Islander people, elderly people, CALD populations, refugees, and sexual minorities. 18
Data were formulated into tables to summarise and describe the study characteristics, as well details reported about marginalised populations within the surveillance systems.
Results
A total of 3247 articles were identified from the initial search strategy, with 949 articles removed as duplicates. Screening of title and abstracts identified 35 articles for full-text review. Of these, 13 met the inclusion criteria, with 0 additional articles identified through a review of the reference lists of included articles (Figure 1). Only four of the nine available annual FluTracking reports were identified through the search. The remaining five FluTracking articles were sourced from the Australian Government Communicable Disease Intelligence website, 19 bringing the total number of included articles to 18.
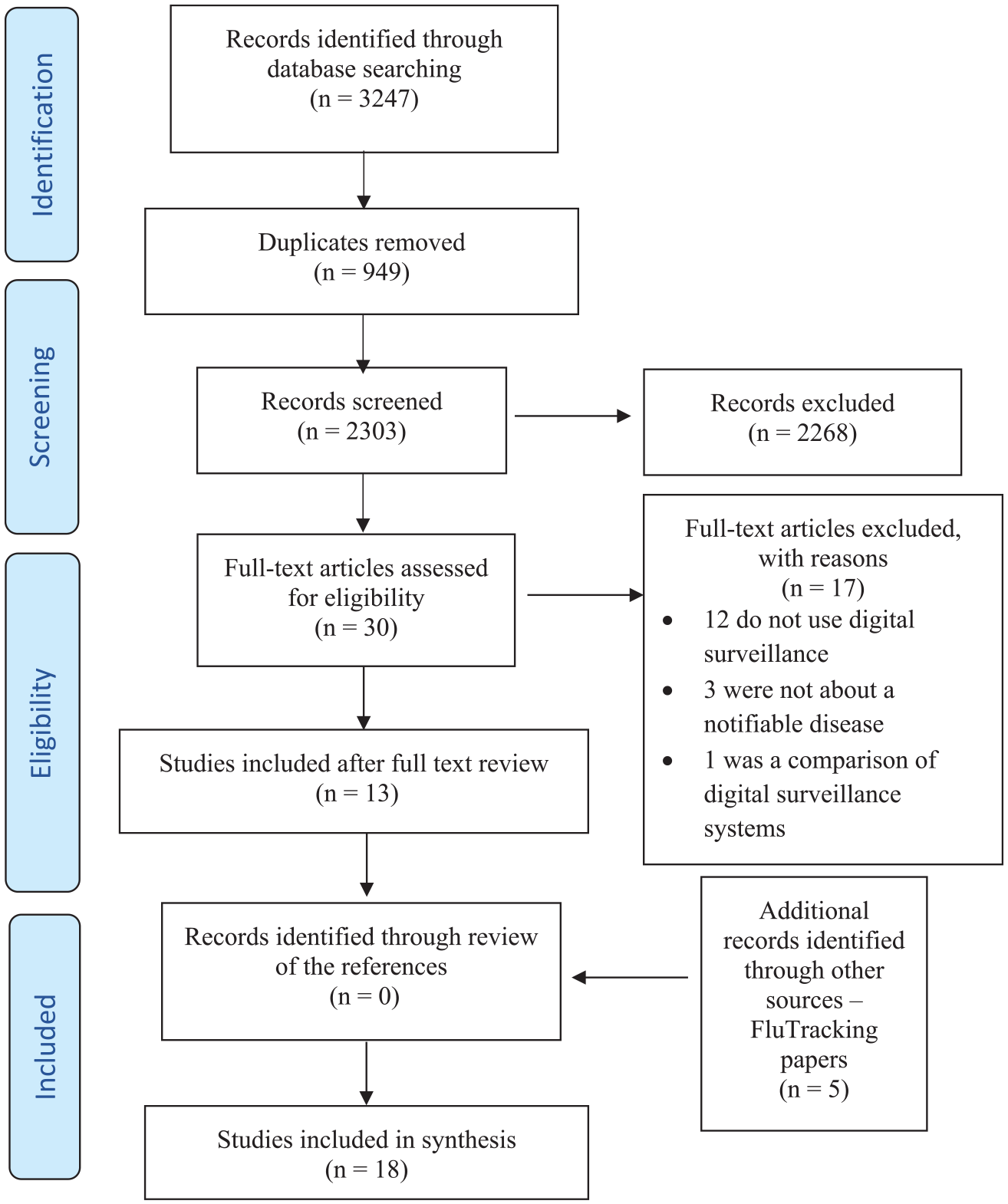
PRISMA flowchart.
The secondary search strategy including COVID-19-related documents yielded 792 articles, with 288 duplicates removed. Screening of title and abstracts identified eight articles for full-text review; however, none of these met the inclusion criteria.
A total of seven surveillance systems were studied across the 18 included articles. Nine articles correlate to the FluTracking system, with studies conducted from 2006 to 2018.20–28 One study correlates to the use of Twitter as a potential surveillance system, conducted in 2015. 29 One study correlates to the SmartVax system and was conducted in 2013. 30 Two articles correlate to the FASTmum programme, both studies conducted in 2013.31,32 The VaxTracker system has two associated studies conducted in 2013 and 2017.33,34 Two studies conducted in 2015 correlate with the AusVaxSafety programme.35,36 The final surveillance system is the STARSS system which has one associated study conducted in 2017. 37 Overall, the time period for included articles ranged from 2006 to 2018, with the majority of studies conducted from 2013 onwards (72%). This is likely as a direct result of the creation of five of the seven surveillance systems after the 2010 incident in which a particular brand of influenza vaccine caused an increase in febrile reactions (including febrile convulsions) in Australian children.30,32,33,35–37
Data extraction identified influenza (n = 10)20–29 and adverse events following immunisation (AEFI; n = 8)30–37 as the two most common notifiable conditions monitored using digital methods for surveillance in Australia. A total of 16 of the 18 articles had influenza, influenza-like-illness, or response to the influenza vaccine as their surveillance topic.20–33,35,36 The two studies that were not associated with influenza included the VaxTracker study conducted in 2016 regarding AEFI from the pneumococcal polysaccharide vaccine in the elderly 34 and the STARSS study analysing AEFI from any vaccine. 37 Seven studies were conducted nationally,23–29 and of the remaining 11 studies conducted in individual states, most collected data from digital surveillance systems implemented in health practices located in NSW (n = 8), Western Australia (WA; n = 6), and South Australia (SA; n = 4).20–22,30–37 The vast majority of included studies (n = 17) collected data from participants via online surveys linked through Short Message Service (SMS) or email, or direct response to SMS.20–28,30–37 The one remaining study collected data from an algorithm monitoring geo-tagged tweets (see Table 1). 29
Characteristics of included studies.
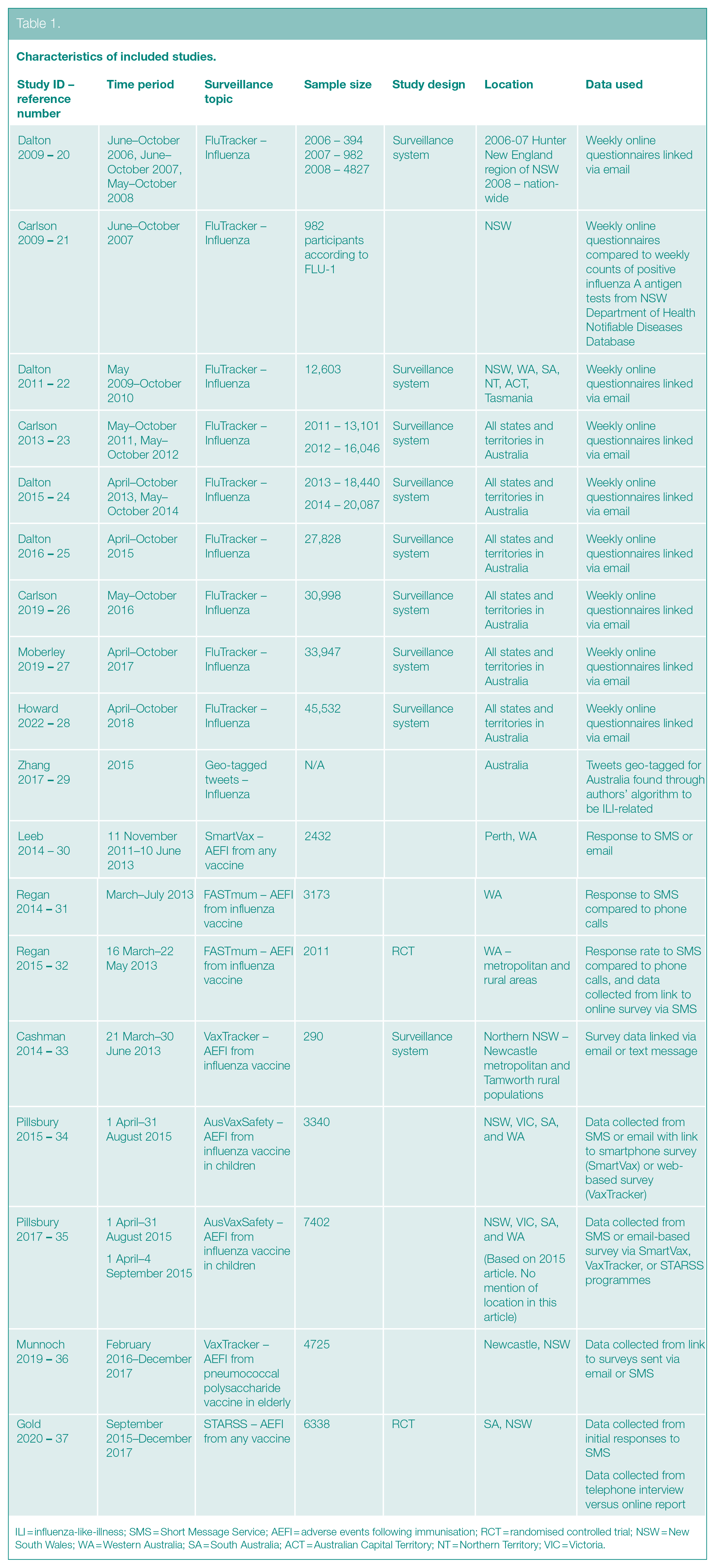
ILI = influenza-like-illness; SMS = Short Message Service; AEFI = adverse events following immunisation; RCT = randomised controlled trial; NSW = New South Wales; WA = Western Australia; SA = South Australia; ACT = Australian Capital Territory; NT = Northern Territory; VIC = Victoria.
A total of six surveillance systems (all except Twitter) encompassing 16 studies reported information on sub-populations.20,22–28,30–37 Of these, three surveillance systems (FluTracking, FASTmum, and AusVaxSafety) encompassing nine studies included data on marginalised populations.23–28,32,35,36 The FluTracking annual surveillance reports initially stratified data according to age, state/territory, vaccination status, and whether participants worked with patients.20,22 From 2012 to the most recent report, other socio-demographic characteristics have been incorporated including sex, highest educational level attained, and Aboriginal and Torres Strait Islander identity.23–28 A separate FluTracking report specific to data collected from Indigenous Australian participants was published in 2019 analysing trends in fever and cough rates and vaccination rates since 2012. 38 This information was not included in the annual reports.
Of the five digital health surveillance systems monitoring AEFI, the FASTmum programme 32 and the AusVaxSafety programme35,36 were the only ones to report and analyse data collected from Aboriginal and Torres Strait Islander participants. The initial FASTmum article did not collect socio-demographic characteristics apart from age. 31 However, the following year an Aboriginal and Torres Strait Islander status question was added to the survey and data on response rate to SMS versus phone interview were analysed and stratified according to ethnicity. 32 The AusVaxSafety programme (which encompasses STARSS, VaxTracker, and SmartVax surveillance systems) also collected data on Aboriginal and Torres Strait Islander status; however, it did not further analyse or report this within the initial study. 35 The following AusVaxSafety study analysed fever rates in Aboriginal and Torres Strait Islander participants compared to non-Indigenous participants, but did not analyse these data in accordance with other sub-populations included, such as age, sex, underlying medical conditions, and whether or not medical attention was sought. 36 VaxTracker was the only subset of AusVaxSafety that reported including a question on Aboriginal and Torres Strait Islander identity on their survey, however, did not report any findings in their results (see Table 2). 34
Data reported within included studies.
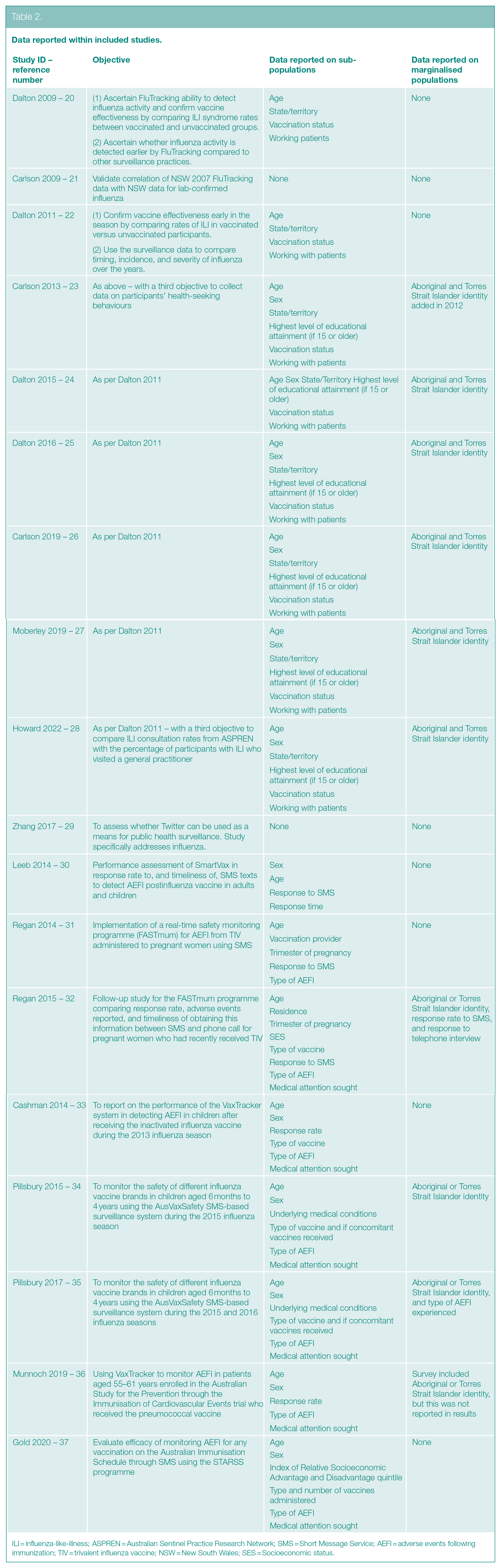
ILI = influenza-like-illness; ASPREN = Australian Sentinel Practice Research Network; SMS = Short Message Service; AEFI = adverse events following immunization; TIV = trivalent influenza vaccine; NSW = New South Wales; SES = Socioeconomic status.
Four of the nine studies, three of which are associated with FluTracking and one with AusVaxSafety, identified the percentage of participants with incomplete surveys.23,26,27,35 Of the FluTracking articles, approximately half (54.8%) of participants answered the question on Aboriginal and Torres Strait Islander status in 2012, when the question was first incorporated into the survey. 23 In 2016, 87.4% of participants had a complete survey, 26 rising to 92.3% in 2017. 27 Aboriginal and Torres Strait Islander representation by 2018 made up 1.6% of FluTracker’s sample population. 29 The 2015 AusVaxSafety article reported that 24.5% of participants did not answer the ethnicity question; however, the percentage of participants who identified as Indigenous was 4.7%. 35 It is unclear if the 2015 AusVaxSafety study recorded responses of other ethnicities apart from ‘Indigenous’. No other article included in this study recorded data on CALD populations.
Discussion
This review identified that there are a number of surveillance systems within Australia for notifiable diseases utilising digital methods, which appears to be increasing over time. In our study, the two main notifiable conditions currently monitored using these methods are influenza and AEFI.20–37 Half of the studies identified reported some information in relation to Aboriginal and Torres Strait Islander identity for the population.23–28,32,35,36 Almost all articles reported data in relation to some specific demographics including age, sex, and education.20,22–28,30–37 Despite this, the data collected or reported in relation to sub-groups that characterise diversity in terms of health care needs, access, and marginalised populations are minimal.
The majority of digital surveillance for notifiable conditions in Australia focuses on influenza and adverse events following the influenza vaccination.20–33,35,36 This is consistent with global literature with most digital surveillance systems for communicable diseases focusing on influenza. 39 Epidemics of influenza occur annually, with vaccination for some groups recommended each year. The constantly evolving nature of the spread of disease and vaccination uptake makes influenza a useful case study for this type of surveillance. This has also been the case with COVID-19, which is a constantly evolving public health situation requiring surveillance and occurred concurrently with the development of new methodologies in disease surveillance. While not captured in this review, a number of digital surveillance tools were utilised in the public health response to COVID-19 in Australia. The COVID-Safe App was implemented in Australia to assist with contact tracing, 40 and within Queensland a number of digital aspects were incorporated into the response including the Queensland response Digital Corona Virus Application and integrating data from both private and public pathology laboratories into a data lake. 41 These types of examples used in the field were not included in this study as their descriptions and results are not recorded in published research articles. This is a significant limitation of our study as many developing systems that should meet our inclusion criteria may only be documented in grey literature as yet.
Approximately, half of the studies across this review, encompassing three of the seven surveillance systems, reported data on Aboriginal and Torres Strait Islander Australians.23–28,32,35,36 However, completeness and representativeness of these data in some instances were identified as an issue.24,27,28,36 The FluTracking system has collected data on Aboriginal and/or Torres Strait Islander identity since 2012, although the number of participants was not large enough to be representative of the Aboriginal and Torres Strait Islander population. 24 The completeness of data has improved over time, increasing to 92.3% in 2017. 28 However, the proportion of participants identifying as Aboriginal and/or Torres Strait Islander remains low (approximately 1.6%) compared with 3.3% of the Australian population. 29 FluTracking credits the high completeness of the data with a small minimum data requirement. This means, only a few variables are collected from participants at registration, with a clear purpose for the collection of each field. 42
The inclusion of data in relation to Aboriginal and Torres Strait Islander Australians is important for surveillance systems to ensure that responses can be appropriately targeted where needed. Australia’s Indigenous Digital Inclusion Plan, which seeks to provide all Australians with equal access to Internet, technology, and information, identifies that Aboriginal and Torres Strait Islander’s level of digital inclusion is 7.9 points below the national score. 43 This score compares the level to which people are considered digitally included at an individual level. 43 There is a high rate of mobile phone use within the Aboriginal and Torres Strait Islander population44; however, less access to44,45–47 and affordability of digital systems and technologies compared to non-Indigenous Australians are key contributors to this inequity.43,45 Hence, levels of digital literacy,43,45 as well as age and education level, 48 can impact recruitment into use of digital surveillance systems or technologies. Making systems accessible and culturally appropriate is necessary for the inclusion of Aboriginal and Torres Strait Islander people.
As noted earlier, there are also issues with the completeness of data as well as variations in reporting. For example, in notifiable disease data there is still great variation in completeness across states and territories. 49 There are also additional requirements for the creation and use of any digital surveillance system when collecting and reporting Aboriginal and Torres Strait Islander data. System design should address the importance of data sovereignty, which is ‘the right of Aboriginal and Torres Strait Islander peoples, communities and organisations to maintain, control, protect, develop, and use data’. 50 As well, systems should be co-designed with Aboriginal and Torres Strait Islander community representatives, with results being reported back to the community openly.
Despite these challenges, evidence suggests that digital health interventions can be effective and beneficial in marginalised populations.51,52 This evidence, coupled with a disproportionate impact from communicable diseases, 53 means that funded and accessible digital health surveillance programmes are an important aspect to lessen digital health inequity. Some programmes are currently attempting to address this disparity. For example, the ATLAS Indigenous primary care surveillance network aims to monitor the STI and BBV burden in Aboriginal and Torres Strait Islander populations across Australia. 54 This network is partnered with the Aboriginal Community-Controlled Health Organisation sector and was designed to address the disparity in testing, treatment, and management of sexually transmissible infections and blood borne viruses, but as yet only a methods article has been published. 55
There are a number of other marginalised groups who are also important to consider in infectious disease surveillance. These include those who are homeless and older individuals, both groups disproportionately affected by communicable diseases and recommended to receive annual influenza vaccination. 55 The majority of studies in this review collected and reported information in relation to age of participants.20,22–28,30–33,35,36 However, no studies collected or reported data on homelessness, CALD, or other marginalised populations. Historically, surveillance of diseases within homeless populations is challenging as this information is generally not recorded in data collection systems. 56 One aspect of digital technology which is showing promise to assist with surveillance in homeless populations is data linkage. 57 However, this has not yet been used for communicable disease surveillance. There are further challenges for data collection as participation in digital reporting would require a phone or computer and homeless individuals have reduced access to digital technology. 58 Despite the challenges, the importance of surveillance to identify how best to target public health interventions remains. Further investigation into how these barriers can be overcome is warranted.
There are several limitations to this study which need to be considered in the interpretation of the findings. We restricted publications to those in English; however, as the aim was to investigate this issue in the Australian context it is unlikely that relevant articles were not included due to language. We did not incorporate grey literature into our search, which may have resulted in publication bias. There may be systems operating in Australian Health Departments which have not been part of research studies or publications. However, we believe this review provides initial evidence to highlight this issue and a follow-up study engaging the grey literature and health departments would be the next step to further this work.
Overall, there are limited research articles investigating digital surveillance for notifiable conditions in Australia. Incorporating these methods into public health practice is essential, feasible, and provides additional information which can complement existing systems. However, greater focus on the equity of these systems and the need to incorporate data for marginalised populations is essential. Issues of inequity in recruitment, varying levels of digital literacy, matters of privacy and data sovereignty, and the overall accessibility of the digital health system for inclusion of marginalised populations should be addressed, ideally prior to its use. Local data are necessary to make local decisions, and so these data should also be fed back to the communities on which they impact for further work to be done. Therefore, it is recommended that a set of principles is established for the future creation and use of any digital surveillance system.
Supplemental Material
sj-docx-1-rsh-10.1177_17579139241237101 – Supplemental material for Representation of marginalised populations in digital surveillance for notifiable conditions in Australia: a systematic review
Supplemental material, sj-docx-1-rsh-10.1177_17579139241237101 for Representation of marginalised populations in digital surveillance for notifiable conditions in Australia: a systematic review by N Dias-Karunaratne, L Whop, J Ward, C Vujovich-Dunn, J Amin, A Dakiniewich and A Dyda in Perspectives in Public Health
Footnotes
Acknowledgements
All data utilised for this review were publicly available, hence ethical approval was not sought. No funding was provided for this project, and we have no competing interests to declare.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Lisa J Whop was supported through a National Health and Medical Research Council (NHMRC) Investigator Grant (#2009380).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.