
Abstract
Aims:
To evaluate evidence on loneliness interventions that have been assessed and found effective, both for remediation and addressing fundamental causes of loneliness; to consider why population-level primary prevention strategies targeting fundamental causes are necessary, and determine areas for future research; and to outline an integrated approach to prevention considering roles for the Public Health system.
Method:
We conducted a review of systematic reviews to identify effective loneliness interventions and classified them in our Population-Prevention Matrix according to public health impact, amount of individual effort required, and level of prevention. We also highlighted emerging interventions that have yet to be formally evaluated.
Results:
We identified a range of preventive or therapeutic approaches, and a dearth of population-level primary prevention interventions targeting fundamental causes of loneliness. Filling this gap will be essential in addressing the loneliness epidemic, and we provided emerging examples of population-level primary prevention interventions that may inform future efforts.
Conclusion:
Based on evidence to date, we suggest an integrated approach to prevention with significant roles for the US Public Health system, including its function as Chief Health Strategist to lead and guide multisystem approaches to loneliness prevention, with a particular focus on population-level primary prevention strategies.
Background
Loneliness, the subjective feeling of inadequate meaningful connection to others, is prevalent throughout the US. In 2019, pre-COVID, 61% of Americans over the age of 18 years were lonely. 1 While most loneliness research focuses on older adults, loneliness is not restricted to one stage of life. In comparison to the roughly 50% of adults over the age of 80 years who experience loneliness, the proportion of adolescents and young adults who experience loneliness reaches 71%. 2 Notably, such widespread loneliness is a 21st-century problem. In contrast with today’s estimates, the prevalence of loneliness in the US in the 1970s was estimated to be as low as 11%. 3 The increase in prevalence over time appears related to a multiplicity of ways that loneliness has become socially constructed in 21st-century America, 4 with some shared and some differential drivers by age group. Late 20th- and 21st-century factors – including changes in family structure and location, longer lives with high rates of loss of significant others in old age, a built environment fostering independence and isolation, weakening of local institutions that strengthened social capital, and the ways the Internet is used by young adults – appear to be major contributors.
While feeling lonely at times is a normal and perhaps necessary part of being human, 5 chronic loneliness adversely affects health and wellbeing. Research on the effects of loneliness at the cellular level indicates that chronic loneliness elicits an immune response that promotes inflammation, and chronic inflammation can facilitate the onset of chronic diseases, including cardiovascular diseases, cancer, cognitive decline, Alzheimer’s disease, and frailty.5,6 There is also evidence that chronic loneliness leads to adverse mental health outcomes, such as increased rates of anxiety and depression. 7 More broadly, loneliness appears to be a driver of ‘deaths of despair’ 8 – deaths due to alcohol, drugs, and suicide.
High rates of chronic loneliness also have an impact on healthcare utilization beyond what is expected from effects on health. Older Americans who are chronically lonely visit their doctors more often than those who are less frequently lonely, controlling for illnesses and self-rated health. 9 While evidence is lacking on whether this trend extends to more frequent utilization of other healthcare services, many primary care providers and systems report an escalation of patients coming to alleviate loneliness. Anecdotally, medical care systems find a dearth of programs in the community to which patients at high risk of loneliness may be referred.
A public health perspective on chronic loneliness is raised by the need for primary prevention strategies targeting causal factors in a heavily contextually induced condition. It is further necessitated by evidence on how loneliness spreads through populations. Occurring in clusters and spreading through a ‘contagious’ process in which individuals who feel lonely induce feelings of loneliness in their contacts, 10 chronic loneliness may require population-based solutions, as with infectious disease, to contain the contagion and resolve population-level causes.
Each of the points above contributes to a perspective that loneliness is a 21st-century social determinant of health, indicating a need for primary prevention at a population level, as well as for individuals, with high potential from interventions that create 21st-century social infrastructure to build anew social connection, cohesion, and capital. 4 All three types of loneliness (Table 1) would be amenable to structural interventions, from connectors of transportation and the Internet to the social infrastructure of the built environment and community-based organizations. 4 Sustainable primary prevention could well be led or co-led by the US Public Health system, through community programming and by fostering all-of-society approaches. This article therefore aims (1) to evaluate evidence on loneliness interventions that have been assessed and found effective, both for remediation and addressing fundamental causes of loneliness; (2) to consider why population-level primary prevention strategies targeting fundamental causes are necessary, and determine areas for future research; and (3) to outline an integrated approach to prevention considering roles for the Public Health system. Given cross-country heterogeneity in how the loneliness epidemic may manifest and be resolved, these aims are specifically considered in the context of the US, but findings may inform broader discussions globally if supplemented with the appropriate cultural nuances.
Types of loneliness
This table summarizes the three types of loneliness according to Cacioppo et al. 11
The Current State Of Loneliness Interventions In The Us
To assess the landscape of interventions for loneliness in the US, we conducted a systematized umbrella review of the MEDLINE database, including systematic reviews and/or meta-analyses published in English between 2010 and 2020 that focused on interventions for loneliness. From these articles, we extracted and reviewed interventions from the US that were deemed effective in preventing or treating loneliness. The search terms, flow chart, and summary table of effective interventions identified in this review are in Supplementary Appendix 1.
From the 22 systematic reviews included in our analysis, we identified 17 unique interventions to prevent or treat loneliness that were evaluated and found effective. Of the three main types of loneliness (Table 1), all of the interventions identified addressed either relational or collective loneliness. These included community-based programs (i.e., peer support communities and structured community recreational activities), as well as tailored therapeutic individual interventions prescribed for use at home (i.e., animal-assisted therapy) or administered in a clinical context (i.e., relationship and social skills training and small group cognitive–behavioral therapy). We analyzed these interventions along two axes: (1) the five tiers of Frieden’s Health Impact Pyramid 12 and (2) the three levels of prevention, thereby assigning each intervention a spot in our Population-Prevention Matrix. The five tiers represent interventions delivered in different contexts to: (1) alter social and economic determinants of chronic loneliness and precarity; (2) design structural and environmental conditions that serve as a community’s social infrastructure, and thus facilitate human connection and diminish population-level risk for loneliness; (3) offer long-lasting protections against chronic loneliness by direct intervention, such as via community resources or programs to remain connected around shared interests or needs; (4) engage individuals with clinicians or care coordinators to regularly screen for loneliness and recommend protections against chronic loneliness; and (5) use health education or counseling services to therapeutically support cognitive and behavioral changes that provide skills for individuals to diminish their loneliness. As in Frieden’s original design, moving from Tier 1 to Tier 5 requires increasing levels of individual effort and produces decreasing levels of population impact.
The three levels of prevention represent primary, secondary, and tertiary prevention interventions to: (1) provide skills, programs, resources, or environments that enable connection and reduce the likelihood of chronic loneliness broadly and specifically in vulnerable populations; (2) screen for early cases of chronic loneliness and prevent progression; and (3) treat chronic loneliness, respectively. However, an important inadequacy of the existing literature is that interventions are typically described with no indication of whether the loneliness under study is chronic or acute.
In representing the evidence in our matrix, we allowed categories of interventions to span multiple tiers and/or levels of prevention. Our placement of the identified interventions in this matrix is shown in Figure 1 and summarized here.
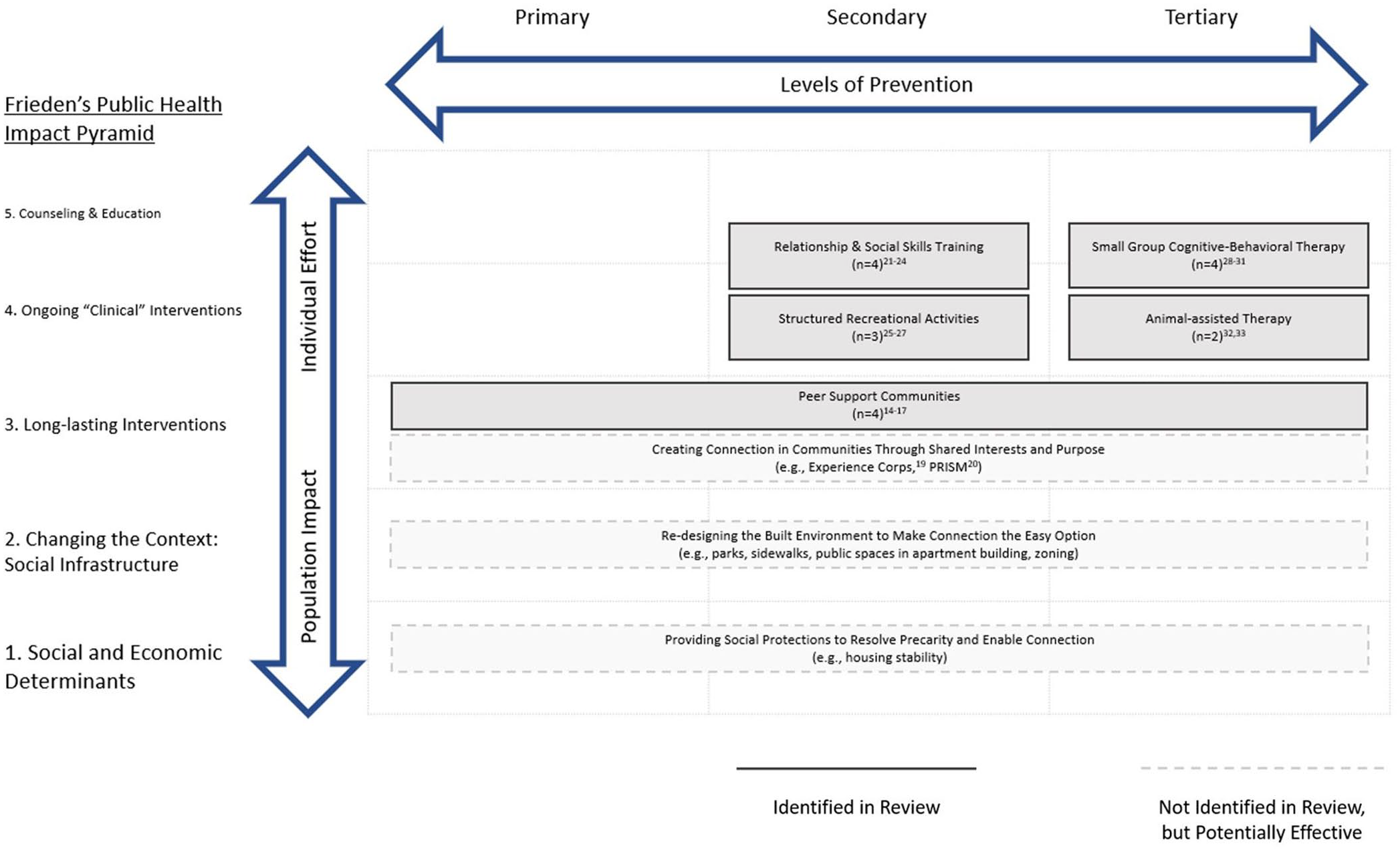
Effective loneliness interventions identified through systematized umbrella review. This figure shows the matrix of Frieden’s Public Health Impact Pyramid and the three levels of prevention. Interventions at the top of the matrix require the most individual effort and produce the least population impact. Interventions at the left of the matrix are primary prevention efforts and interventions at the right of the matrix are tertiary prevention efforts. Each box represents a distinct category of intervention and notes the number of interventions included in that category (n). US interventions that have been shown effective are allocated to the box indicating their type of prevention, by Frieden’s pyramid level. Boxes are allowed to span multiple cells of the matrix if interventions in that category can be implemented at multiple tiers of Frieden’s pyramid and/or levels of prevention. Boxes with dashed borders indicate categories of interventions that were not identified in our formal review but may be effective based on emerging evidence.
Tiers 1 and 2: Socioeconomic and Structural Interventions
Loneliness is a painful individual state resulting from an interaction between a vulnerable host, societal predisposing conditions, and – potentially – a precipitating life event,3,4 such as retirement, financial precarity, or a pandemic. A range of 20th-century conditions and norms emphasizing independence over community – along with the fraying of social capital, civic organizations, and social protections – have led to decreased opportunities for meaningful connection in the 21st century. The absence and deterioration of social infrastructure which facilitate connection and cohesion extend across the built, social, and economic environments. 4 Examples of the former include lack of public transport or public spaces in apartment buildings or Internet connectivity; the social environment includes declines in societal institutions that foster social capital and cohesion, 13 media portrayals of stereotypes that marginalize certain groups, and inadequate social protections that lead to precarity and preclude trusting relationships; 14 and the economic environment includes the lack of jobs or economic protections that enable stability and resulting positive social connections.
Interventions in the bottom two tiers of Frieden’s pyramid would address these modifiable socioeconomic or structural drivers of chronic loneliness that bias the system toward creating and perpetuating loneliness. We did not identify any interventions effectively targeting such drivers. However, there are approaches that have not been formally evaluated or have only been preliminarily evaluated that we should consider. For example, the precarity of daily life accompanying socioeconomic instability often precludes individuals from taking advantage of opportunities for social engagement. 14 In this regard, provisions for stable housing, design of public spaces to foster connection, violence prevention, and other social protections are likely preconditions for loneliness prevention. Furthermore, social circumstances in the 2020–2021 pandemic reveal root causes for heightened loneliness, such as the need for draconian social isolation in nursing homes.
Tier 3: Long-Lasting Interventions
In the third tier of Frieden’s pyramid, we identified peer support communities, which offer physical or virtual environments where people with similar health or other conditions that limit social connection can come together to mitigate loneliness, without addressing its fundamental social capital causes.15–18 This type of intervention included primary prevention for general community members, 18 secondary prevention for at-risk individuals, 15 and tertiary prevention for those who are already chronically lonely. 17 As with Tiers 1 and 2, we recognize there are emerging opportunities for Tier 3 interventions not identified in current review articles. For example, the evidence indicates that lonely people prefer solutions that are not about solving loneliness per se, but about bonds with people with shared interests. 19 So, community-based or online programs that create connection through shared interests, like Experience Corps – an intergenerational volunteer program providing older adults with opportunities to build meaningful relationships and serve in local elementary schools – may prevent chronic loneliness. 20 The reach of such efforts may be broadened if efforts are made to enable individuals to connect with their surrounding communities by increasing accessibility of technology – for example, by expanding programs like Older Adults Technology Services that increase computer literacy. In the COVID-19 pandemic, it has become clear that Internet connectivity is essential and should be delivered as a public utility. New technological approaches that foster online connections with new social networks for older adults – such as the Personal Reminder Information & Social Management System (PRISM) – show effectiveness in recent trials. 21 If broadly implemented, these interventions may span primary to tertiary levels of prevention by creating the conditions that help prevent individuals from becoming chronically lonely while also making recovery easier for those who are at-risk of becoming or already are chronically lonely.
Tier 4: Ongoing Clinical Interventions
In the fourth tier of Frieden’s pyramid, we identified four types of therapeutic interventions that could help resolve or prevent loneliness and were prescribed by or required ongoing engagement with clinicians or care coordinators: relationship and social skills training for care recipients and providers,22–25 structured recreational activities,26–28 small group cognitive–behavioral therapy,29–32 and animal-assisted therapy.33,34 The first two types of interventions are secondary prevention because they facilitated or enabled connection among individuals who were at-risk of chronic loneliness (e.g., children with difficulties communicating), while the remaining two are tertiary prevention specifically aimed at treating loneliness. For secondary prevention, one study found that a friendship training intervention consisting of 12 weekly 60-min sessions designed to equip children with social skills needed to form meaningful connections also reduced loneliness. Using scores from 16 items on the Children’s Loneliness and Social Dissatisfaction Scale, those who received the training experienced a 3-point decrease in scores (indicating less loneliness) at the end of the 12-week intervention while those who did not receive the training experienced a 1-point increase in scores. 23 For tertiary prevention, a study of blind older adults who were believed to have been lonely for an extended period of time found that follow-up scores on the 20-item University of California, Los Angeles (UCLA) Loneliness Scale for those who received therapy were 40% of the maximum possible score, while scores for the control group were 55% of the maximum possible score, compared to an average baseline score of 55% for both groups. 29
Tier 5: Health Education and Counseling
In the fifth tier of Frieden’s pyramid, we identified two types of interventions that could use health education and counseling to encourage cognitive or behavioral changes to protect against loneliness for those at risk: relationship and social skills training and small group cognitive–behavioral therapy. As previously described, both of these types of interventions also qualified as ongoing clinical interventions (Tier 4), and relationship and social skills training took the form of secondary prevention while cognitive–behavioral therapy took the form of tertiary prevention. Compared to interventions in other tiers, these interventions produced the greatest effect, with the four cognitive–behavioral therapy interventions showing 12- to 34-point reductions in 20-item UCLA loneliness scores among those who received therapy versus 0- to 9-point reductions among those who did not receive therapy.29–32 As tertiary prevention efforts, these interventions were highly targeted toward individuals with pre-existing chronic loneliness or related mental health conditions (e.g., people who scored exceptionally high on the UCLA Loneliness Scale at baseline, Navy recruits at-risk for depression) and were specifically designed to treat loneliness. Therefore, while they appear greatly effective, in alignment with Frieden’s conceptualization of this tier of the pyramid, they have limited population-level impact.
Overall, our review highlighted a dearth of interventions for primary prevention of loneliness, such as those addressing the socioeconomic, structural, normative, social capital, and environmental drivers of chronic loneliness. However, there are programmatic community-based interventions designed to create connection and cohesion which have not been evaluated specifically for effectiveness in loneliness prevention but have high potential. In contrast, we identified numerous interventions targeting individuals that were effective for secondary or tertiary prevention but capable of producing only low-moderate levels of population impact. To end the loneliness epidemic, it is important to realize the availability of these interventions does not obviate the need for interventions that address the fundamental causes of chronic loneliness by changing the context, social infrastructure, and social capital of society.
Primary Prevention At The Population Level Is Key
To understand the necessity of primary prevention interventions across Tiers 1–3, even when other treatment strategies are effective, it is important to recognize the value of primary prevention in the context of loneliness. To illustrate this, consider the Hawkley and Cacioppo 5 model of loneliness, which suggests a ‘self-reinforcing loneliness loop’ in which individuals who feel lonely are likely to adopt behaviors and perceptions that exacerbate feelings of loneliness. This vicious cycle highlights the challenges of waiting to intervene until loneliness is chronic. In addition, the high prevalence of loneliness in the population necessitates population-level primary prevention. Moving to solutions, it is therefore also important to consider where primary prevention is enacted.
Critically, primary prevention ranges from individual approaches aiming to prevent chronic loneliness in those who are at the greatest risk to population approaches aiming to remove the fundamental drivers of chronic loneliness. The value of primary prevention varies according to how, where, and on whom it is enacted. The seminal epidemiological work by Geoffrey Rose 34 lays out criteria for the ‘high-risk’ strategy for prevention, which targets individuals who are likely to develop an undesirable outcome, as well as its limitations: notably, this approach offers only palliation or therapy for the individual, but does not remove the underlying causes of the outcome. Conversely, the population strategy for prevention has the potential for increased impact because it aims to reduce or eliminate determinants of the outcome throughout the population. This is particularly salient in loneliness prevention, since one-person-at-a-time interventions do not offer the structural or programmatic solutions for a problem of interpersonal connection and shared interests and purpose. Therefore, prevention strategies for chronic loneliness at the population level are expected to be more impactful in the long term than those targeting ‘high-risk’ cases.
Together, these points highlight the importance of not only focusing on primary prevention generally but also specifically focusing on population-level primary prevention that alters the fundamental drivers and contexts that create chronic loneliness. The inadequacy of social infrastructure to counter 21st-century drivers of loneliness makes this a prime target for solutions, to foster community-level bonds of reciprocity and trust essential to social capital and likely critical to diminishing rates of loneliness in the population. This is the unmet and critical approach needed to diminish the 21st-century epidemic of loneliness. Accomplishing this will require investment in interventions at the intersection of the first column and Tiers 1–3 of Figure 1, and allocation of implementation responsibility.
The Potential Roles Of Public Health In The Prevention Of Loneliness
While population-level primary prevention is key, multiple factors influence loneliness at various levels. For example, personal traits and life transitions facilitate or hinder feelings of connection among individuals while socioeconomic and structural factors – such as housing security and designs that facilitate connection, neighborhood safety and walkability, public transportation accessibility, media influences, precarity, and neighborhood social capital – simultaneously determine if feeling connected is attainable. Therefore, integrated, multilevel approaches to chronic loneliness prevention will likely produce the synergistic effects necessary to end the loneliness epidemic. The three core functions of public health 36 – assessment, policy development, and assurance – provide a framework for how the US Public Health system may enact key solutions effectively and equitably (Figure 2).
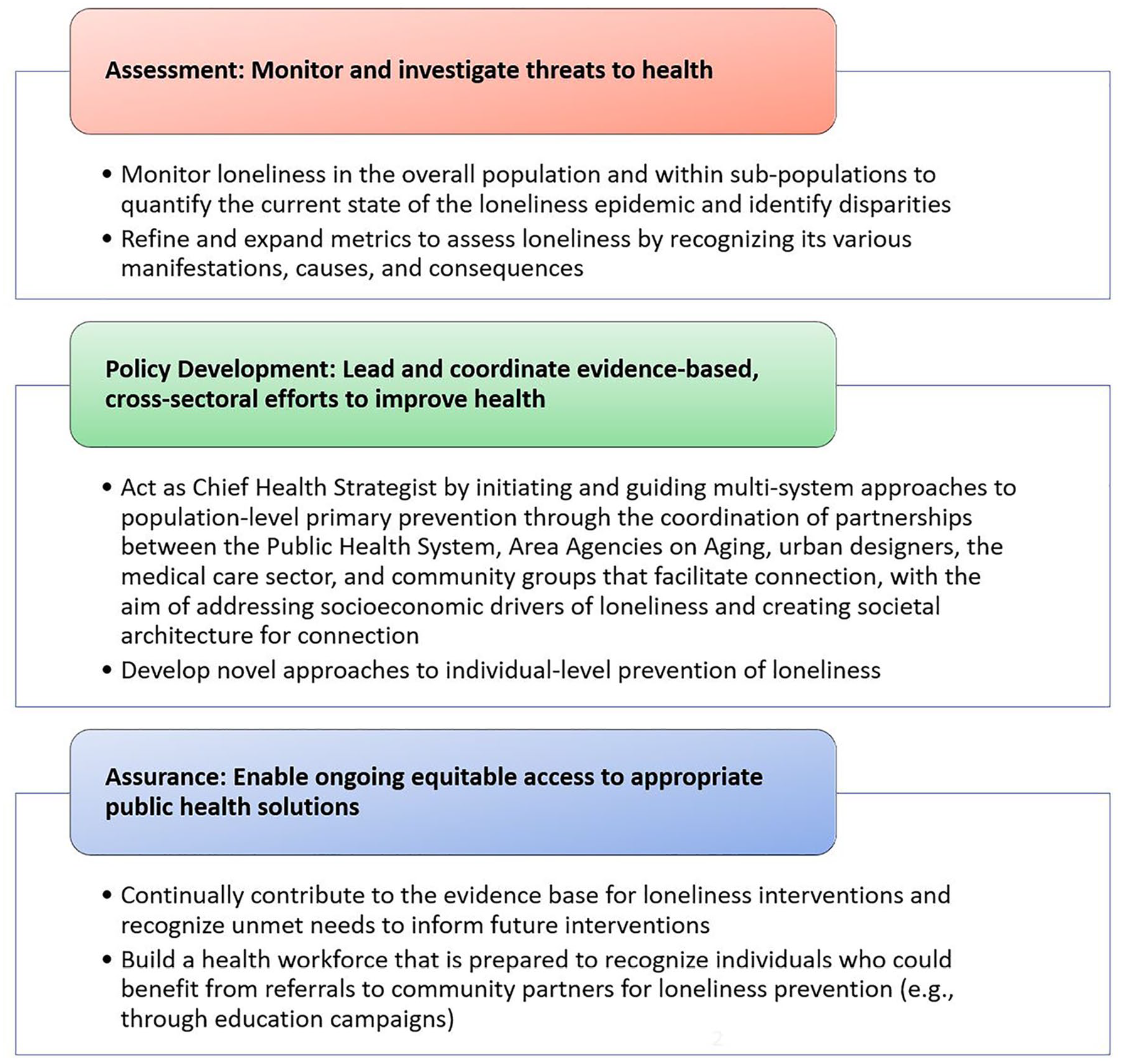
Core functions and tasks for the Public Health system to mitigate the loneliness epidemic
Assessment
The first function of the Public Health system, assessment, is to monitor and investigate threats to health. One key form of assessment is the surveillance of loneliness across the country, which calls for data on indicators of loneliness and types of loneliness in the general population as well as data disaggregated by sociodemographic characteristics that allow for identification of disparities. In support of surveillance efforts, the Public Health system should provide leadership in developing and/or implementing metrics that robustly measure loneliness in all of its manifestations, understanding that different types of loneliness may have different causes and consequences. Having clear, shared, evidence-based guidelines describing who should be considered lonely, how people become lonely, and how loneliness affects their lives and surroundings will facilitate the surveillance of loneliness while also laying the foundation for thoughtful design and evaluation of loneliness interventions needed to fill out the Population-Prevention Matrix. 37
Policy development
The second function of the Public Health system, policy and program development, is to lead and coordinate evidence-based, cross-sectoral efforts to improve health. Given the paucity of interventions that offer population-level impact, the US Public Health system should build policies from programs already in existence that, although not formally evaluated in terms of their abilities to prevent loneliness, provide a starting point for the population-level primary prevention strategies we are lacking. This includes Tier 1 attention to diminishing precarity and isolation through policies and regulations, Tier 2 development of social infrastructure to support connection and cohesion, and Tier 3 building of programs that foster social capital – at scale.
In addition to pioneering primary prevention policies, efforts are needed to expand effective secondary prevention policies and synergize clinical and population-based interventions across Frieden’s pyramid to fortify the integrated approach to prevention. If individuals are identified in clinical settings as being chronically lonely, structures and programs must be in place to link them to opportunities for connection within their communities. 38 Having public health leaders who champion policies to bolster community organizations with evidence-based loneliness prevention strategies is also critical from the population prevention perspective in that, if appropriately implemented, these strategies will be widely accessible to all members of the community regardless of loneliness status. This means everyone may reap the benefits of a reduced likelihood of developing chronic loneliness. Examples of such community-based approaches to loneliness prevention can be seen in the United Kingdom’s LinkAge Hub programs that aim to broadly facilitate connection through community members’ shared needs and interests. 39
Importantly, throughout all elements of policy development, the US Public Health system could embrace its role as the Chief Health Strategist for communities by initiating and guiding cross-sectoral collaborations with the aim of creating conditions to address the causes of loneliness.37,38 This could involve leading partnerships between the Public Health sector, Area Agencies on Aging, urban designers, the medical sector, and community and civic organizations to create programs that foster social capital and meaningful connection. Building on evidence suggesting the policies needed to achieve this aim – whether they are related to civic organizations, community-based programming, education, housing, public spaces, technology, transportation, volunteerism, the workplace, or any other sector – public health leadership can provide convening opportunities, programs, and education to build cross-sectoral partnerships to design, implement, and evaluate these policies. In preparing for these collaborations, the US Public Health system may turn to examples of partnerships already underway, such as The Loneliness Lab in the United Kingdom, which was ‘created to bring together business, government and civil society to explore how we can reshape and reimagine our cities to design out loneliness’, 40 as well as the needs experienced in the medical care system in the US that require community-based programming solutions.
Assurance
The third function of the Public Health system, assurance, is to enable ongoing equitable access to public health solutions. A primary component of this function is the continual accumulation and application of research to ensure public health practice is rooted in evidence. This would include, for example, ongoing evaluation of the evidence for loneliness interventions to highlight gaps between the types of interventions available and the types of interventions needed, as we have done in this article. Others have also made progress on this task, 38 but broader recognition of this gap and the opportunities for solutions are necessary. Another component of assurance is the provision of education and training to ensure a competent health workforce. In this regard, the Public Health system should lead the development of evidence-based education campaigns around loneliness for the health workforce, so care providers may be prepared to recognize individuals who could benefit from referrals to community partners for loneliness treatment or prevention, 38 and public health practitioners and leaders can learn about opportunities for population-based solutions.
Conclusion
Chronic loneliness meets criteria for a prevalent 21st-century social determinant of health. Our review of the loneliness intervention literature found sparse evidence for effective interventions that change the socioeconomic and structural conditions that make loneliness the default option in American society, but background knowledge indicates their importance and the opportunities of programmatic approaches in communities. While strategies focusing on treating chronic loneliness in those who are already affected or preventing it in those who are at ‘high-risk’ are of import, and there are successful models for this, population-level primary prevention strategies are key to reducing chronic loneliness sustainably, and further research is needed to provide an evidence base for such interventions. Recognizing the complex system of factors that cause loneliness, we will benefit from an integrated approach to prevention, utilizing both population-based and individual strategies. The US Public Health system must stand at the center of efforts to combat loneliness by fulfilling its three core functions: assessment, policy development, and assurance. With this leadership, we can build the conditions to end the 21st-century loneliness epidemic.
Supplemental Material
sj-docx-1-rsh-10.1177_17579139221106579 – Supplemental material for Loneliness prevention and the role of the Public Health system
Supplemental material, sj-docx-1-rsh-10.1177_17579139221106579 for Loneliness prevention and the role of the Public Health system by CL Crowe, L Liu, N Bagnarol, LP Fried and N Bagnarol in Perspectives in Public Health
Footnotes
Author Note
N Bagnarol is now affiliated to SUNY Downstate Health Sciences University, New York, NY, USA.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: As this manuscript is based on a review of published literature in which informed consent was obtained by primary investigators or from which only de-identified data were analyzed, ethical approval was not required. C.L.C. was supported by a fellowship from the National Institute of Mental Health (5T32MH013043).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.