
Abstract
Aims:
Social prescribing continues to grow and change across healthcare services in Wales; however, research of the day-to-day performance of social prescribers is limited. This study aimed to explore which roles are perceived to be the most important and frequently used by social prescribers in Wales and compare these results to reports in studies of services in other countries in order to support future role development and potential standardisation.
Methods:
This study used the Group Concept Mapping via the Concept Systems Global Max™ software to collect and analyse all data from both participants and literature.
Results:
There was a total of 101 statements generated (119 participants, 84 literature) ranging from generic interpersonal skills to specialised training (cognitive behavioural therapy). These statements were then sorted by conceptual similarity into seven clusters (Providing a Specialist Service, Working in a person-centred way, Skills, Connecting Clients with Community, Collaborative Working, Evaluating and postprogramme duties, and Networking/Community). Statements were rated based on their perceived importance and frequency, with the ‘Skills’ cluster having the highest overall average and ‘Providing a Specialist Service’ having the lowest.
Conclusions:
Reports indicate that in general there is variation in the roles performed by individual participants in Wales; however, greater variation was observed between participants and literature suggesting geographical divergence in practice. In the top 12 highest rated statements for both frequency and importance, individualistic traits such as empathy and ‘being a listener’ are favoured over specialised methods such as cognitive behavioural therapy and behaviour change taxonomy. Results suggest that local need plays a part in the choices and performance of social prescribers and as such should be considered in future standardisation.
Introduction
Social prescribing has been a part of UK healthcare policy and procedure since the early 1990s, but a recent growth in popularity has resulted in new services from a range of UK providers. 1 Service aims vary from targeting specific mental2,3 or physical health conditions 4 to offering a ‘holistic’ approach to wellbeing. 5 They generally focus on the biopsychosocial factors that affect health using non-clinical interventions. Services are aimed at people living with long-term physical health conditions, mental health diagnoses or social isolation. Enthusiasm from commissioners and health care professionals for social prescribing has grown as services are perceived to increase patient self-management and reduce healthcare use.6,7 The increased focus on intersectoral ‘joined-up working’ in the NHS 8 means social prescribing may be seen as a mechanism for social, third and health sector collaboration given the establishment of the Social Prescribing Academy in England. There is a need, however, for a greater understanding of how and for whom these services are effective throughout the UK. 9
Social prescribing in Wales is a collaborative process mostly between statutory health services and the third sector, with staff management being the responsibility of third-sector organisations. 10 This has led to a variety of service models with decisions made to meet local and organisational need/demands, resulting in variation in staff performance whose day-to-day roles may include community development, counselling and/or signposting. 11 Various terms are used to describe front-line workers in social prescribing, for example, social prescribers, link workers and community connectors. In this article, we will use the term social prescribers to cover the range of terms. Social prescribers are often cited as a vital component of the social prescribing process,12–14 and the variety in social prescriber roles is indicative of the lack of standardisation in the United Kingdom. 15
Despite the increase in social prescribing research, there is a knowledge gap about the impact of services and how the service components contribute to the outcome. Systematic reviews have found inconclusive results due to lack of study rigour, participant adherence rates, small sample sizes and inconsistency in research methods use, for example, absence of validated outcome measures and control groups.16,17 Few published studies address the black-box nature of interventions. They lack detail on service configuration and participant interaction with services, for example, number of appointments. Previous studies’ results highlight the importance of social prescriber/client interaction to service success; however, there is limited research on social prescriber performance at local level.
This study sets out to answer the question, ‘What are the roles and day-to-day activity of social prescribers in Wales?’. It aims to explore the social prescriber role from the role-holder perspective. Group Concept Mapping (GCM) methodology 18 is used in a mixed-methods consensus design to explore the frequency of use and perceived importance of daily roles and activities of social prescribers in Wales and compare their performance with that reported internationally. The results of this study will contribute to the development of a competency framework for social prescribing practitioners in Wales.
Methods
Setting and design
GCM consensus methods were used at each stage of inquiry via Group Wisdom™ online software. 19 The rationale for using GCM was its ability to engage geographically diverse participants, its short time scale from design to completion and its ability to present complex data in an accessible manner. Many of the recruited participants were also familiar with the study design, having participated in previous GCM studies.
The study steering group (C.W., C.L., D.P., M.W.) was drawn from members of the Wales Social Prescribing Research Network University of South Wales, PRIME Centre Wales, Public Health Wales and Cwm Taf University Health Board. It was funded by the KESS 2 Knowledge Economy Skills Scholarship and forms one part of a PhD project.
Ethical approval
Ethical approval was granted by the University of South Wales Research Ethics Committee (approval number 19TR0901LR).
Participants
The study recruited participants from across Wales, all of whom were currently performing the social prescriber role (other terms used to describe participants’ roles include link worker and community connector). Due to the low numbers of potential participants, a total population sampling method was applied. Participants were recruited using existing connections through the Wales Social Prescribing Research Network. The study information sheets were sent to organisations and were then disseminated to social prescribers. Participants who were interested in participating were asked to request a consent form for completion and return. If participants failed to return consent forms following this initial expression of interest, they were reminded at two fortnightly intervals. Recruitment took place from September 2019 to November 2019. Although recruitment was initially proposed via a single health board (Cwm Taf University Health Board), low recruitment figures prompted the study team to widen the recruitment area to the remaining six health boards. In total, 16 participants were assigned to the study, with 7 completing each stage in full.
Procedure
All three phases of participant data collection were completed using the Group Wisdom™ online platform. An email invitation was sent to prospective participants before the study start and on receiving informed consent, individuals were sent a unique login code. Participants were able to personalise this after initial login. Each phase took 30–40 min to complete. The phases ran sequentially and were completed over a 14-week period, and participants were offered telephone support and prompts to complete tasks to time.
Phase 1 – brainstorming
Brainstorming in GCM usually consists of participants generating statements in response to a focus prompt. In this study, the focus prompt was:
As a link worker/social prescriber/community connector my role includes …
This was completed by participants over 2 weeks during November 2019, at which point statements were cleaned – checked for spelling and/or grammar errors, conjoined statements were separated and duplicates removed, leaving n = 46 statements produced by participants. Duplicate statements were confirmed by steering group member consensus.
Following Stoyanov et al., 20 the GCM process was altered to include focus prompts derived from social prescribing studies published between January 2016 and April 2019. These were identified by TR from a recent systematic review 17 using Squire et al.’s method 21 for inclusion. This resulted in a broad representation of social prescribing across peer-reviewed studies and grey literature of services in England, Scotland and the Netherlands. Of these studies, 30 reported on social prescriber activity and were searched for declarative statements in response to the focus prompt. Statements were generated through in vivo coding and were subject to the same cleaning and duplicate removal process as those created by participants. Where literature statements were duplicated by participants, the participant-generated statement was used. This resulted in 84 unique statements from the literature confirmed by the steering group.
Phase 2 – sorting
All cleaned statements were made available to participants for the sorting phase in mid-December. This involved grouping statements using a drag-and-drop interface. Participants sort statements based on their perceived similarity. The metric by which similarity is defined is left to the individual participant. Statement groups have no upper size limit, so long as they have a minimum of two statements per group. No group may consist of one statement. Each group is labelled by each participant with a phrase that best describes their perceived similarity. The final group label is the most frequently used term by the participants.
Phase 3 – rating
Statements are de-grouped in the rating phase, and participants rate each statement using two 5-point Likert-type-style scales. In this case, participants rated the frequency of role/activity performance and their perceived importance. This took place during a 2-week period in January 2020, and all data collection was complete by 24 January 2020.
Analysis
GCM analysis is completed in three steps using the Group Wisdom™ software:
All statements are plotted in a similarity matrix. This charts the frequency of statements being grouped together.
A point map is generated from the similarity matrix. Each statement is given an XY coordinate. This is achieved using multidimensional scaling analysis.
Finally, hierarchical cluster analysis is applied to the point map. A series of diagrams and reports including a cluster map, a cluster rating map and go-zone analysis are generated.
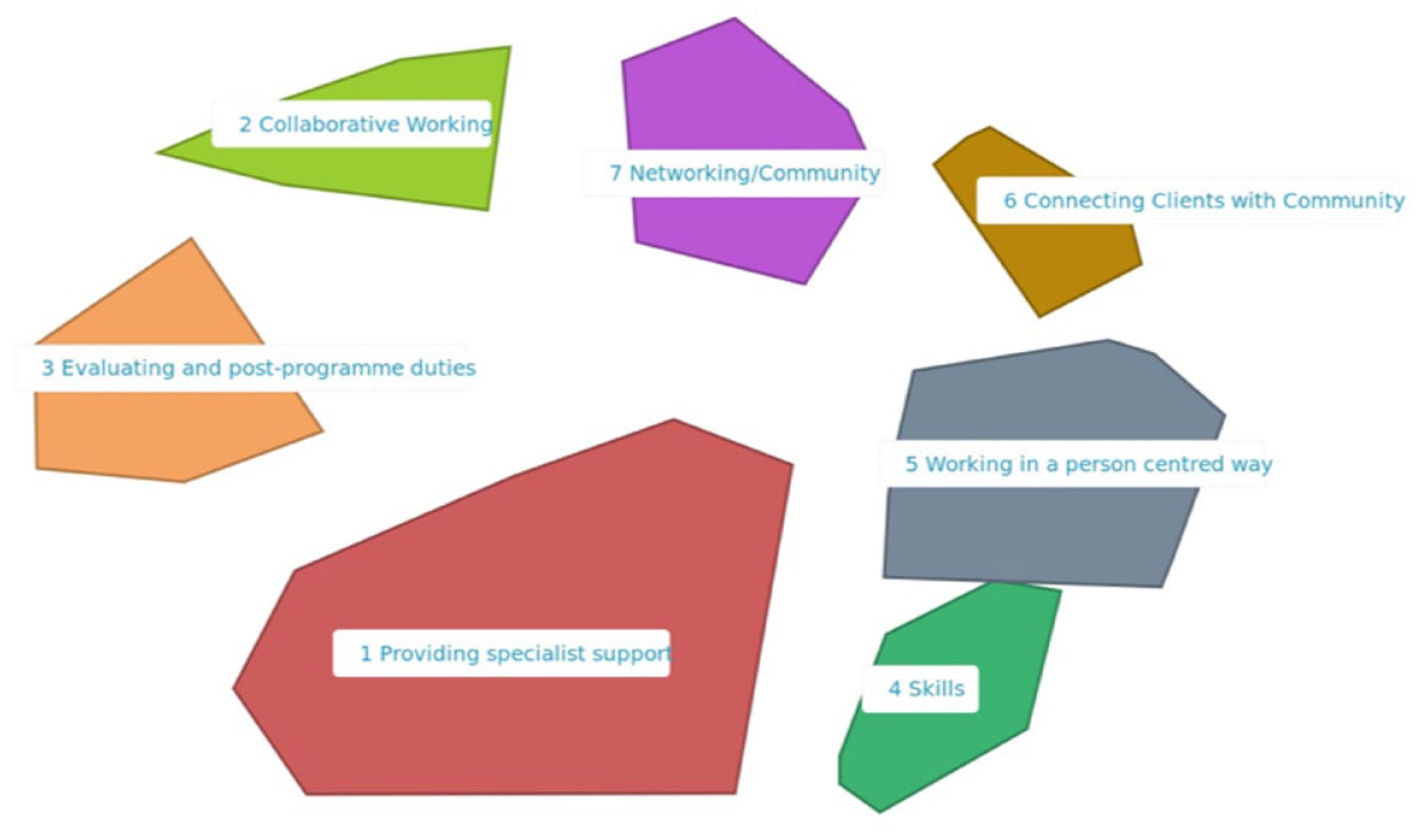
The point map is generated by the Group Wisdom™ software, but the final configuration of clusters is decided upon by the user, that is, the study steering group. The software generated a range of cluster configurations from fifteen clusters to three (Figure 1); the chosen map contains seven (Figure 2). A number of factors are taken into consideration in this decision, and Kane and Trochim 18 recommend that the final arrangement should be informed by context and practicality.
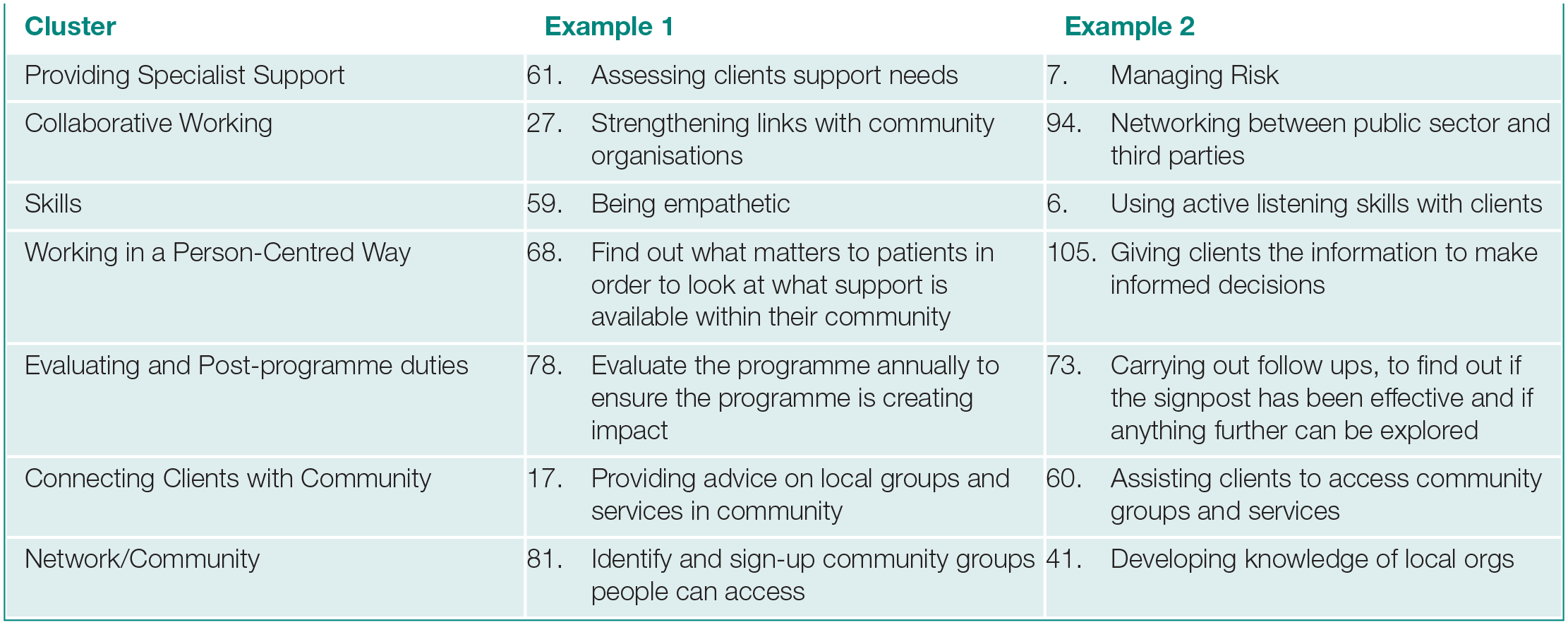
Clusters and example statements (full list of statements available in Appendix A in Supplemental material)
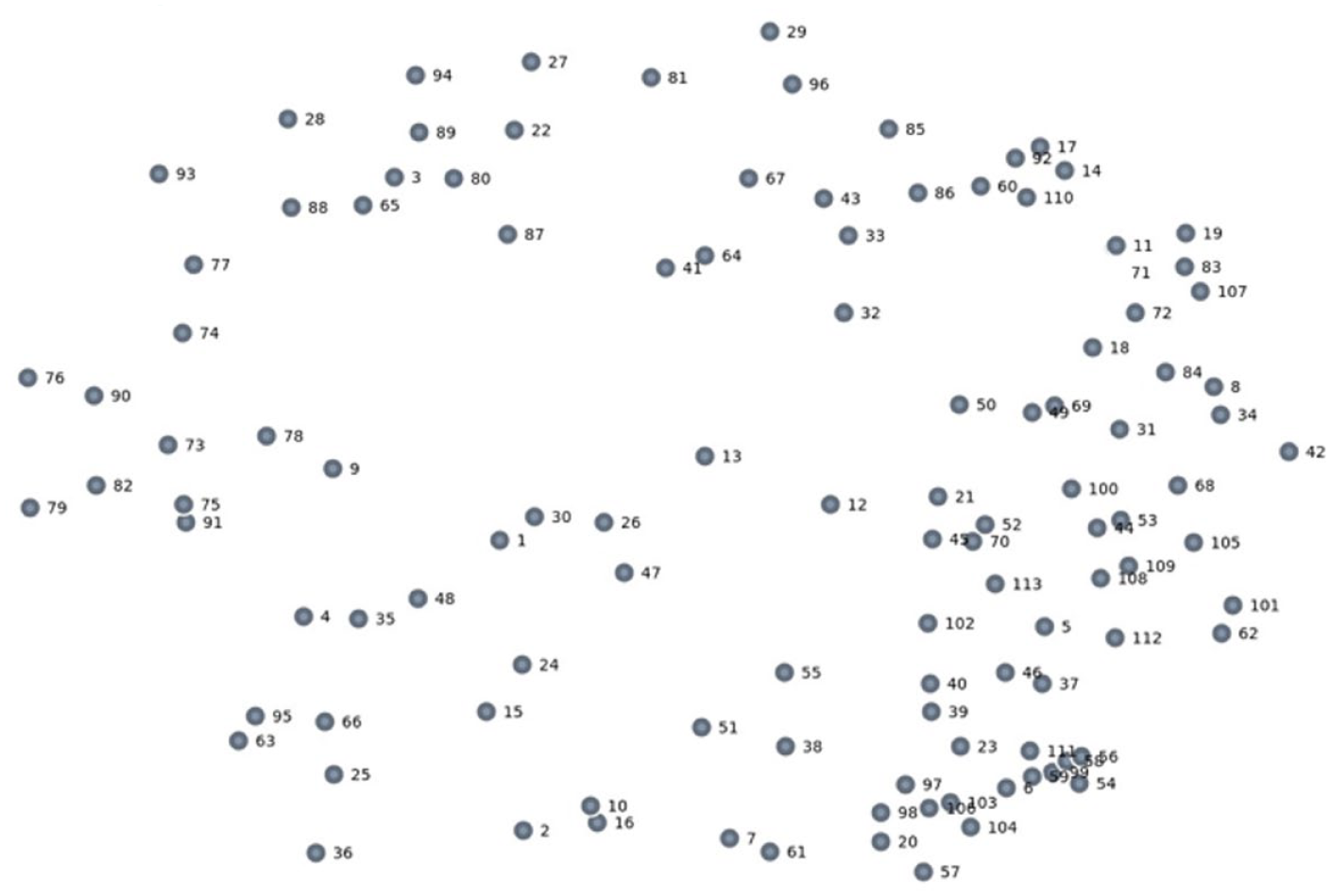
Point Map
At each stage, the results were discussed with the study steering group and consensus was sought at each stage of interpretation.
Results
Brainstorming – generating statements
Participants identified 46 unique statements during the brainstorming phase. Initially, 40 statements were produced but the steering group considered that a number of these needed splitting as they contained multiple statements in response to the focus prompt. For example, the statement: ‘Capturing all the data, to complete a quarterly report and service evaluations’ was separated into two statements – ‘Capturing all the data to complete a quarterly report’ and ‘Capturing all the data to complete service evaluations’ (see Statements 75 and 76). A similar process was applied to the 84 statements derived from analysing 30 studies gathered in the literature review. Both sets of statements were cross-referenced for duplicates which were removed, leaving a total of 113 statements. Where duplicates existed between the two groups, the statement generated by participants was used. All of the resulting statements were then used to populate a point map plotting statements on an XY axis based on their similarity (Figure 2). The map has a stress value of 0.3048, which is within the suggested range of 0.205–0.365. 18 Despite being on the higher end of the scale, the map implies a good relationship between the results of the points’ placement on the map and the sorting exercise, suggesting internal validity. 22
Cluster maps
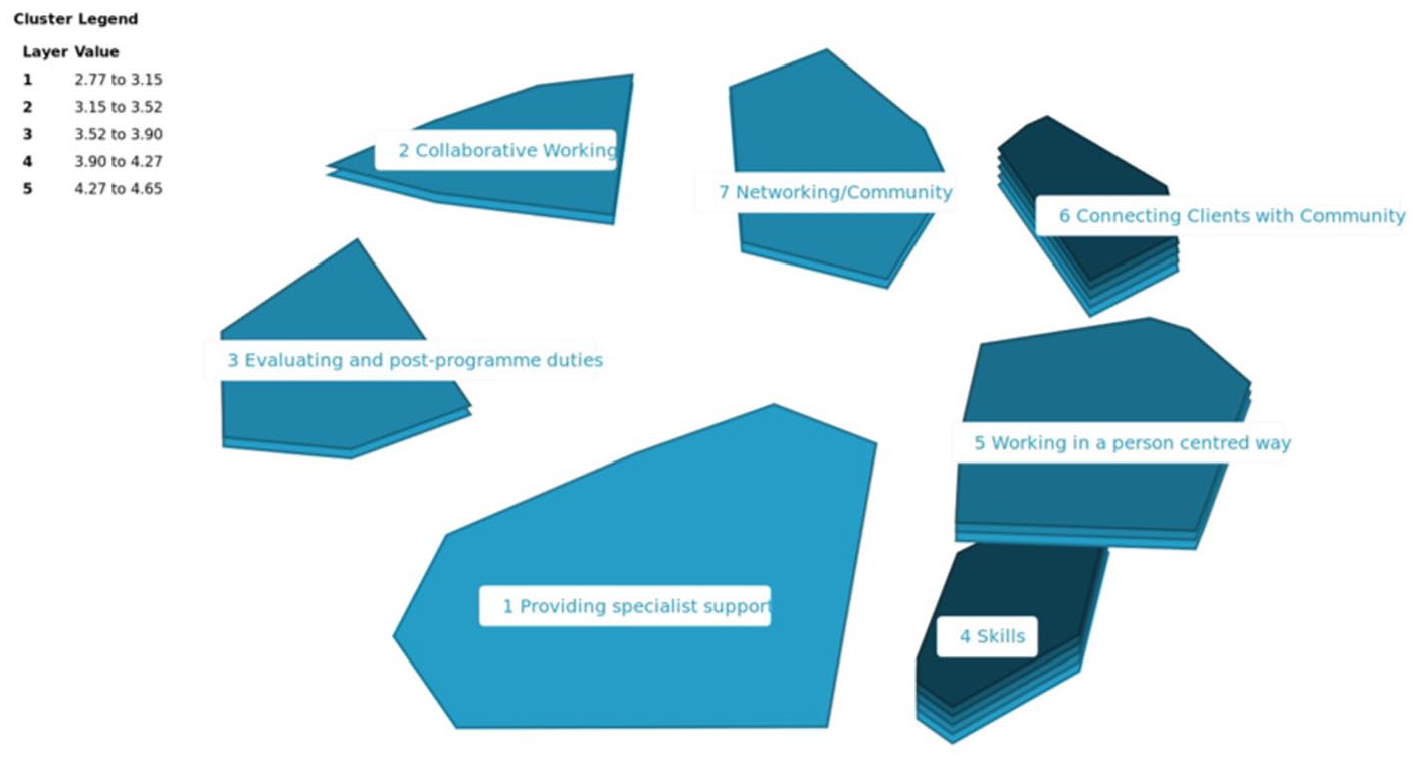
The cluster with the highest number of statements is ‘Providing Specialist Support’ (n = 24) followed by ‘Working in a person-centred way’ (n = 23), ‘Skills’ (n = 21), ‘Connecting Clients with Community’ (n = 12), ‘Collaborative Working’ (n = 11) and ‘Evaluating and post-programme duties’ (n = 11) and ‘Networking/Community’ (n = 11).
The XY placement of clusters on the map (Figure 3) represents their contextual similarity. For example, ‘Collaborative Working’ and ‘Networking/Community’ are adjacent while ‘Skills’ and ‘Collaborative Working’ are on opposite sides of the map. The distribution of participant statements and literature derived statements is consistently even except for two clusters: ‘Providing Specialist Support’ and ‘Evaluating and Postprogramme Duties’. The ‘Providing Specialist Support’ cluster is almost entirely composed of literature-only statements (96%), serving as a cluster for roles considered less relevant to participants’ daily activity. In contrast, the ‘Evaluating and Postprogramme Duties’ only contained one literature derived statement, with 10 participant statements. Of these 10, three statements were duplicated in the literature and 7 were unique to participants, making this cluster the most unique to participants.
Cluster map
The cluster rating results (Figures 4 and 5) show the most frequently performed roles were found in the ‘Skills’ cluster, followed by ‘Connecting Clients with Community’ and ‘Working in a person-centred way’. The most important clusters were these three clusters and ‘Evaluating and Postprogramme Duties’. The least frequently performed and important cluster was ‘Providing Specialist Support’, while ‘Evaluating and Postprogramme Activities’ was reported as having a higher importance than frequency of performance. There is a perceived parity between cluster importance and frequency with which the corresponding roles are performed.
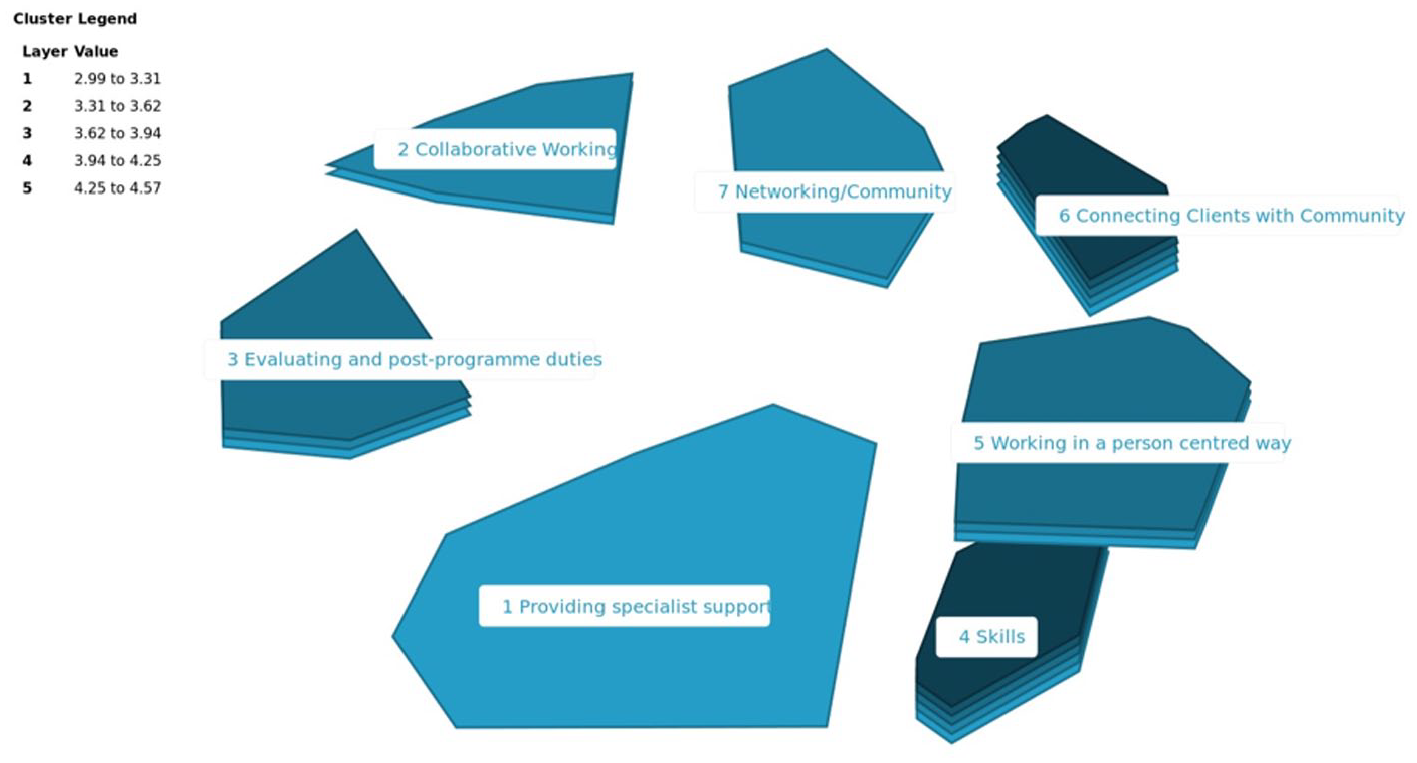
Cluster rating map – importance
Cluster rating map – frequency
Go-zone
The Go-Zone report (Figure 6) charts the individual rating data of each statement on an XY axis. The mean for both rating scales intersects the graph creating quadrants. The four zones may be interpreted as: Top Right: Most important and most frequently performed – Core job roles Bottom Right: Important but not as frequently performed – Roles for further integration Top Left: Frequently performed but not as important – Roles for reconsideration Bottom Left: Least important and least frequently performed – Unrelated roles

Go-zone map
The top 12 statements of the top right Go-Zone were split 5:7 between literature-only and participant statements based on their combined average score. Conversely, the 12 lowest scoring statements in the bottom left Go-Zone were split 10:2 between literature-only and participants’ statements. The most highly represented cluster within the top right Go-Zone was ‘Skills’, whereas ‘Providing Specialist Support’ featured most prominently in the bottom left Go-Zone. ‘Evaluating and Postprogramme Duties’ was the most common cluster in the bottom right Go-Zone, while the most common cluster in the top left Go-Zone was ‘Working in a person-centred way’.
Discussion
The study results outline the roles and skills used in everyday social prescriber practice in Wales. It gives insight into the role from their perspective by asking them to identify the most important aspects of their day-to-day praxis. The inclusion of literature-derived statements allows us to compare and contrast roles that are most consistent and most disparate between social prescribers working in Wales and those represented in literature.
Results suggest there is variety in the social prescribing role in Wales consistent with previous research. 17 These range from highly specified roles and knowledge, such as Cognitive Behavioural Therapy and Behaviour Change Taxonomy to more general professional attributes, including displaying empathy or ‘being a listener’. This variety is apparent when comparing the results of participant generated statements with literature-derived statements; however, it still exists among the groups themselves. This can be seen in the ‘Providing Specialist Support’ cluster which has the largest share of literature-only statements (96%), relating to specialised techniques or knowledge (psychotherapy, cognitive behavioural therapy) and localised service features. In the participant statements alone, there is variation in social prescriber engagement with clients and organisations. Some participants take a more direct role by providing activities, while others pre-audit organisations before referral; other social prescribers report taking responsibility for public health messaging, while some report writing case studies. There exists a perceived flexibility even on a local scale, which may be due to the professional background of social prescribers, the organisational perspective, or specific requirements of local populations.
This study’s results indicate a clear trend that the most important and most frequently performed roles are related to the individual traits demonstrated in performance. The statements in the top right of the Go-Zone map (core job role) are more likely to originate in ‘Skills’ (29%) or ‘Connecting Clients with Community’ (22%) clusters, which contain a mixture of performance descriptors and duties. In the top 12 highest rated statements, 50% originate in the ‘Skills’ cluster, suggesting that the most vital aspects of the role are individual attributes such as ‘Being Empathetic’ and ‘Being a listener’, as well as skills and approaches such as ‘Delivering a flexible service’ and ‘Building trust’.
It is interesting to note that 62% of the ‘Skills’ statements found in the top right Go-Zone were exclusively found in the literature. It may be that social prescribers did not recognise the value of these traits in their performance during the brainstorming phase despite their perceived importance and frequency of performance. It may also be a response to the phrasing/interpretation of the focus prompt as personal attributes may not have been considered by participants as a valid response, instead favouring statements describing activity. In contrast, the least important and frequently performed statements found in the bottom left Go-Zone were mostly from the ‘Providing Specialist Support’ (41%) and ‘Working in a Person-Centred Manner’ (20%) clusters. This pattern is echoed in the 12 lowest rated statements; 67% were found in the ‘Providing Specialist Support’ cluster and 83% were exclusively found in the literature. Unlike the top right zone statements, these mostly focused on specific training, knowledge or service delivery, for example, ‘Coordinating care’, ‘Having expertise in psychotherapy’ and ‘Acting as a case manager for patients’. On this end of the scale it may be interpreted that statements represent localised needs that are unrelated to the performance of social prescribers from Wales included in this study.
When comparing the results of literature-derived statements and participant generated statements, a number of issues are apparent. First, some statements are shared between the literature and participants in the original data (n = 13). These focus on procedural roles including ‘collecting data’, ‘conducting face-to-face meeting’ or ‘signposting clients to community organisations’. It was expected that there would be differences related to specified knowledge or skills, for example, psychotherapy or counselling. It was unexpected to note the difference in statements including attribute declarations such as ‘building trust’ and ‘being empathetic’. These statement types appeared more frequently in literature, despite being recognised as some of the most important during the rating exercise. This suggests that social prescribers perform these roles without self-recognition or that the focus prompt structure did not elicit this type of response.
Other differences include the greater detail provided by the literature on the location of appointments and the type of information on offer. Despite the low overall percentage of duplicate statements, some statements may share contextual meaning but remain separate due to the coding method and language used. For example, the statement from a participant ‘Connecting individuals into their community’ and the statement ‘Supporting patients access to community organisations’ from literature may describe the same process, despite being coded as separate statements; especially when considering their mutual placement in the same cluster and similar importance and frequency scores. Conversely, other statements with a perceived similarity are separated in their rating scores. ‘Making connections between third sector and primary care/health’, ‘Networking between public sector and third parties’ and ‘Improving intersectoral working’ are all rated differently between the top left and top right Go-Zones. This may highlight the local prevalence of certain phrases, resulting in a greater perceived value and relevancy. In this case, the divergent terminology is ‘intersectoral’, which was perceived as frequently performed but less important than ‘networking’.
This is not surprising as reports of services indicate a fluctuation in language even in the most fundamental attributes of services including the title given to social prescribers and service procedures. 17 Further enquiry into social prescribing terminology use and how it changes on a local scale could provide valuable insight into the differences between UK services. There appears to be a level of parity in the practice reported by the participants and in literature, particularly in roles considered the most frequently performed and important. Statements from the literature account for 42% of the top right Go-Zone total. The greatest deviation exists in the bottom left Go-Zone (least important and least frequently performed), which mostly consists of literature statements (83%).
In light of recent calls for social prescriber role standardisation, 9 the study results raise the issue of how standardisation may proceed. Certain elements of social prescriber performance are tied to local need, client group and service, including the skill sets/techniques employed by social prescribers, their interaction with other healthcare staff and the use of local services. Arguably, the success of many social prescribing services is ascribed to their flexibility 17 to meet need. While these local elements may not be relevant for most services, their inclusion retains value in that it suggests a greater sense of personalisation for a particular service and its clients. It may be argued that the standardisation of these elements could have an overall negative impact on services. However, where consistency already exists, further standardisation could improve services already being delivered. When comparing these results to social prescribing training needs as reported by Wallace et al., 11 similarities are visible in the value and consistency placed on delivery and interpersonal skills. Wallace et al. suggest that the most important learning needs were related to ‘Compassion’, such as ‘Building rapport’ and maintaining ‘Professional Boundaries’, while training was simultaneously unavailable. These specific outcomes may benefit from inclusion in training courses and future standardisation, especially as these attributes were consistent in statements generated by participants and literature in this study.
Conclusion
This study offers a number of valuable insights into the current social prescribing landscape in Wales. First, it identifies roles and activities regularly performed by social prescribers that are often flexible and diverse, demonstrating similarities in approach and person specification while demonstrating distinct differences in practice. It gives insight into the perceived value of these roles by those performing them. In particular, the study demonstrates that social prescribers consider interpersonal skills to be more important skills than specialised techniques, and knowledge of local community organisations is considered fundamental. Finally, it offers an initial comparison of social prescribers practice reported in literature (including projects in England, Scotland and the Netherlands) with that of Wales, demonstrating similarities in approach but variety in experience and expected skill levels and areas. These results suggest future value in conducting similar research to generate primary data in alternative UK locations with social prescribers.
Strenghts & Weaknesses
Although not comprehensive, due to the limited sample size and use of literature as opposed to primary data collection, this study offers an initial comparison of third-sector managed social prescribing services (Wales) with alternative designs such as those run by the NHS. This comparison is often neglected in research, with the majority of studies focusing only on NHS-commissioned and -operated services.16,23 The study has a small sample size; however, it remains within range for the GCM method, and its stress value (measuring validity) is within the recommended range. 18
There are potential limitations to using literature to generate statements as studies are reported from a third-party perspective, which may result in mis-interpretation of roles due to their complex interaction with statutory and third-sector organisations and the primary-care focused representation of social prescribing’s definitions. 15 As such future research comparing these results with primary data collected in other locations would potentially provide more direct comparison between the groups and would allow for greater exploration of general and local roles. More research is also needed to understand the justifications for difference in service provision and the factors that inform service design. It is envisaged that utilising this and similar data could provide a platform for the bottom-up development of a competency framework, which may aid the process of link workers’ professional development and/or standardisation.
Supplemental Material
sj-pdf-1-rsh-10.1177_1757913921990072 – Supplemental material for The role of social prescribers in wales: a consensus methods study
Supplemental material, sj-pdf-1-rsh-10.1177_1757913921990072 for The role of social prescribers in wales: a consensus methods study by T Roberts, C Lloydwin, D Pontin, M Williams and C Wallace in Perspectives in Public Health
Footnotes
Author Contributions
T.R. took overall responsibility for all areas including data collection, analysis and production of final manuscript. C.L., D.P., C.W., and M.W. provided input throughout the review process, contributing to the final manuscript. All authors approve the final version and T.R. is the guarantor.
The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, a world-wide licence to the Publishers and its licencees in perpetuity, in all forms, formats and media (whether known now or created in the future) to (1) publish, reproduce, distribute, display and store the Contribution; (2) translate the Contribution into other languages, create adaptations, reprints, include within collections and create summaries, extracts and/or abstracts of the Contribution; (3) create any other derivative work(s) based on the Contribution; (4) exploit all subsidiary rights in the Contribution; (5) the inclusion of electronic links from the Contribution to third party material where – ever it may be located and (6) licence any third party to do any or all of the above.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. All authors have completed the ICMJE uniform disclosure form at ![]() and declare no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years and no other relationships or activities that could appear to have influenced the submitted work.
and declare no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years and no other relationships or activities that could appear to have influenced the submitted work.
Data Sharing Statement
All available data can be obtained from the corresponding author.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper has been funded by the Kess2 Economy Skills Scholarship as part of a PhD with the University of South Wales.
Transparency Declaration
The lead author, Tom Roberts, affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.