
Abstract
Background
Preoperative skin preparation (PSP) is a critical step of surgery to reduce bacteria on the skin that can cause infections. It is commonly believed that the reusable equipment method of PSP reduces environmental emissions relative to single-use options. However, no research comparing entire-life cycle environmental emissions associated with the two approaches exists.
Methods
A Life Cycle Assessment (LCA) was conducted comparing PSP in a European hospital using a single-use applicator versus a reusable equipment method.
Results
Findings highlight the superior environmental performance of a single-use antiseptic applicator method, resulting in 49% less CO2-eq emissions than the reusable method. Similar trends were observed across all categories: climate change, cumulative energy demand, water scarcity, resources, ecosystems, and human health. The single-use applicator had lower energy demand and higher resource efficiency. In addition, the single-use applicator was less sensitive to hospital and staff practice variability.
Discussion
The study challenges the assumption that reusable systems always result in lower environmental impacts. This LCA revealed that efficient manufacturing processes, optimized use of antiseptic during procedure, and reduced energy consumption throughout the single-use method life cycle can decrease the carbon footprint. This highlights the need to scrutinize the life cycle when making comparisons as part of surgical sustainability.
Keywords
Background
Hospitals and their operating rooms (OR) are in a unique juxtaposition of working to improve human health, while simultaneously creating environmental emissions (∼4.4% of global greenhouse gas emissions) that have a negative impact on human health (Hensher and McGain, 2020; Patz et al., 2014). ORs are emission hotspots, producing 21%–30% of hospital waste (Cunha and Pellino, 2023) and consuming 3 to 6 times more energy than other hospital departments (Kwakye et al., 2011). Given the rising number of surgeries globally (Weiser et al., 2015), direct and indirect healthcare environmental impacts will continue to increase. Thus, achieving environmental sustainability in surgery is emerging as a key strategy in addressing climate change.
One critical area of focus is preoperative skin preparation (PSP), which is performed prior to surgeries to cleanse skin and reduce resident and transient microbes that can cause an infection. PSP often uses a lot of consumables, and therefore, particularly considering the growing number of surgeries each year, incremental efficiency improvements in PSP can have a cumulative impact. PSP procedures typically utilize either single-use disposable antiseptic applicators or bulk antiseptic solutions with reusable components such as stainless-steel forceps and gallipots, along with disposable cotton balls and gauze (Casey et al., 2015). Use of reusable components is often seen as a lower-emission option (Keil et al., 2023). Note the Intercollegiate Green Theatre Checklist (2024) advises using reusables in surgical procedures only when this results in an overall reduction in carbon emissions. Nonetheless, no research has compared the entire life cycle environmental impact of single-use versus reusable components in PSP.
This study aimed to evaluate the sustainability performance of PSP methods in a European hospital by comparing a single-use antiseptic applicator (Single-use applicator Method (SM)) with an alternative PSP using bulk non-sterile antiseptic bottles and reusable instruments (Reusable bulk-bottle method (RM)). The goal was to compare opportunities for improving surgical environmental impacts.
Methods
Becton, Dickinson and Company (BD) commissioned EarthShift Global to conduct an ISO-conformant Life Cycle Assessment (LCA) (ISO, 2006) to provide a quantitative evaluation of the life cycle of two PSP methods: a single-use antiseptic applicator (Single-use applicator Method (SM); BD ChloraPrep™) and bulk non-sterile antiseptic bottles and reusable instruments (Reusables bulk-bottle Method (RM)), with a focus on their contributions to CO2-eq emissions and other environmental impacts.
Scope
To evaluate two methods of PSP, the functional unit (FU) was defined as a completion of one preoperative skin preparation procedure for laparoscopic surgery on the abdomen and pelvic region in a European hospital involving a skin area of 2500 cm2.
A laparoscopic procedure was chosen as it is reflective of industry trends towards less invasive, more efficient procedures with lower-cost shorter stays. PSP for laparoscopic procedures are generally consistent across a wide range of surgical procedures including gall bladder removal, appendectomy, hernia repair, gynecological procedures, and bariatric procedures.
Operating room practices with single-use antiseptic applicator
SM uses BD ChloraPrep™ Skin Preparation – an applicator with 26 mL of 2% chlorhexidine gluconate and 70% isopropyl alcohol. This single-use applicator body contains two sealed ampoules with an antiseptic solution. The pledget and foam are used to transfer solution onto the skin. The foam and two cotton swabs are included with every applicator to help distribute the solution. In Europe specifically, one applicator is indicated for coverage of a 50 × 50 cm area. After the activation lever is pressed, the solution is applied to the skin in a back-and-forth motion covering the procedural area. The applicator is then discarded after a single use along with any portion of the solution not required to cover the prep area. The overview of the process and materials used is presented in Figure 1. Single-use applicator method – preoperative skin preparation procedure using the BD ChloraPrep™ 26 mL product and single-use consumables. Reusables bulk-bottle method – preoperative skin preparation procedure using bulk antiseptic with reusable instruments and single-use consumables.
Operating room practices with reusable instruments, bulk antiseptic, and single-use components
RM uses approximately 125 mL of 10% povidone-iodine with reusable equipment (forceps, bowls) and single-use consumables. The antiseptic solution is poured into one or more stainless-steel bowls, and cotton balls are placed inside to soak up the solution. The forceps are used to pick up one PVP-I-soaked cotton ball and apply antiseptic to the skin. Additionally sterile towels and gauze are used to prevent excess antiseptic accumulation. The process is repeated until the surfaces are covered with antiseptic. Once the skin preparation has been completed, the reusable items are sent for reprocessing on-site. For preoperative skin preparation with reusable equipment and bulk antiseptic bottles, there is no “standardized” procedure inventory. The procedural steps were identified from literature and market research.
For the purpose of this comparison, utilization of single-use consumables with a bulk bottle of antiseptic and reusable stainless-steel equipment was used as the comparative process. Povidone iodine (PVP-I) solution was selected as the comparative antiseptic for skin preparation, as it is commonly used in Europe. An estimate of approximately 125 mL of 10% PVP-I is used to successfully cleanse the same skin area in the comparative procedure. While literature indicates that CHG is more effective than PVP-I, for the purposes of this study, we are assuming that both achieve equivalent cleanliness outcomes (Jalalzadeh et al., 2022). The overview of the process and materials used is presented in Figure 1.
Environmental impact comparison
To compare the LCA of two PSP methods, a life cycle inventory (LCI) was compiled for each method. The LCI covered six life cycle stages: component procurement, assembly, sterilization, distribution, use phase, and end-of-life (EoL). Each life cycle stage incorporated the resource use and emissions associated with the extraction and processing of raw materials, manufacturing processes, use phase and waste generation. For the single-use method, components are procured, processed into the final product, and ethylene oxide (EtO) sterilized. Distribution involves shipment to Europe and delivery to hospitals. The reusable method includes production of single-use and reusable components. Reusable parts are packed for sterilization and sterilized on-site in hospitals, which includes cleaning in a disinfector, reassembly, and sterilization before reuse. The use phase, for both methods, considers the sterile items’ utilization during preoperative skin prep. At EOL, single-use waste from both procedures is incinerated without energy recovery. Visual presentation of both Life Cycles is presented in Figure 2. Components and steps of the life cycle of the all-in-one applicator, and reusable material.  .
.
The LCA uses a combination of primary and secondary data. Primary data were not available for some of the procedures, and assumptions were used as substitutes. Secondary data were collected from published and peer-reviews sources, in collaboration with the assembly site team, and through a hospital site visit for the single-use method. All data used in an LCA study combines measured, estimated, and calculated data. Once all of the required data was obtained and the associated flows were calculated to the reference flows based on the chosen FU, system modeling was carried out in LCA software SimaPro 9.5 using Ecoinvent 3.10 ReCiPe Midpoint (H) method.
The assumptions are outlined in Table 1 Supplemental. While the SM applicator has clear instructions for use, there are no standard skin preparation instructions for the reusable method. Thus, products and materials may vary based on practitioner behavior, regional regulations, and clinical organizational guidelines. In this study, a conservative estimate was made for materials in the reusable method.
Results
Impact comparison of single-use versus reusables procedure
The results provide a comparative analysis of two methods of PSP in terms of their environmental impacts across multiple categories: climate change, cumulative energy demand, water scarcity, resources, ecosystems, and human health. To maintain functional equivalency, the results directly compare the usage of a single BD ChloraPrep™ applicator containing 26 mL of antiseptic solution (2% w/v chlorhexidine gluconate and 70% v/v isopropyl alcohol) with 125 mL of 10% Povidone Iodine solution to cleanse the same skin area of 2500 cm2, assuming no differences in efficacy between solutions in a clean surgical skin site.
Figure 3 outlines the impact contributors to each assessed impact category of the LCA for the single-use applicator (SM; BD ChloraPrep™) and the reusable comparator (RM). The total impact of the SM was approximately half of the total impact of the RM in all categories. Comparative life cycle analysis of the completion of one preoperative skin preparation procedure based on the SM (Single-use applicator Method) and RM (Reusables bulk-bottle Method), with RM values normalized to 100%. SM values are presented as percentages relative to RM. Graphs present the main contributors to the impacts to: (A) Global warming—Top left, (B) The human health—Top right, (C) Ecosystem impact—Middle left, (D) Resources—Middle right, (E) Cumulative energy demand—Bottom left, (F) Water scarcity—Bottom right.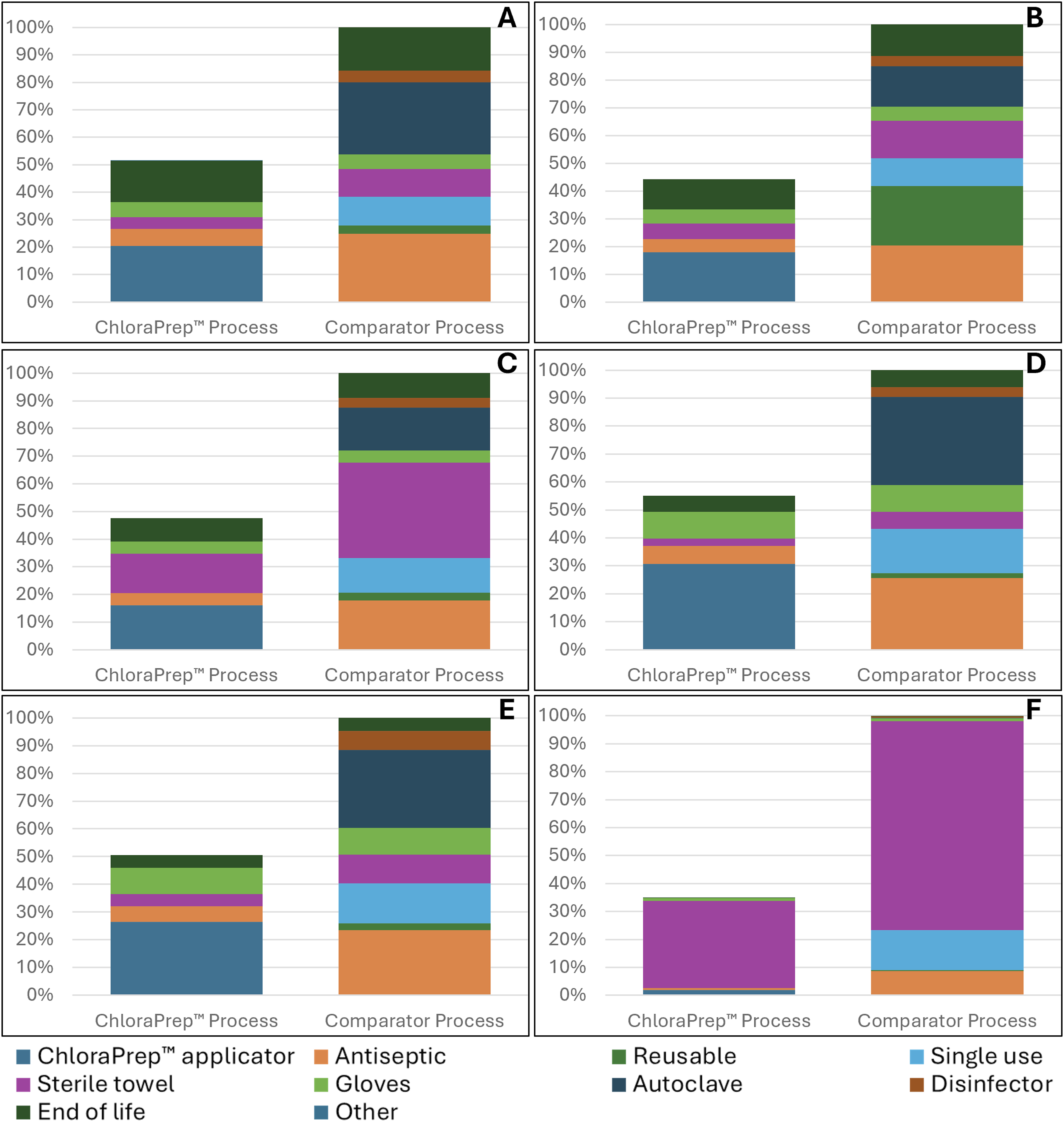
SM emitted 48.7% less CO2-eq than RM, with the main contributors being the applicator and the EoL treatment. In contrast, RM’s largest contributors were the autoclave sterilization, antiseptic, the EoL treatment, and single-use items. In terms of human health, SM had 56% lower impact than RM, following a similar trend to global warming impacts. For RM, the main contributors were reusable items, wasted unused antiseptic, autoclaves, and towels. Ecosystem impacts were 52% lower for SM, driven mainly by the applicator and EoL. For RM, the key contributors were towels, autoclaves, and the antiseptic. Resource impacts of SM were 45% lower than RM, with key contributors being the applicator and gloves. RM’s resource main impact contributors were autoclave, wasted unused antiseptic, and single-use items. Cumulative energy demand for SM was 49% lower than RM, with applicator and gloves being the largest contributors. RM’s energy demand followed a similar pattern to its resources use. For water scarcity impacts, sterile towels were the largest contributor in both methods. However, SM’s impact was 62% lower than RM.
Sensitivity analysis
Several sensitivity analyses were conducted in accordance with ISO 14044 guidelines to evaluate how key assumptions affected study outcomes including: towel usage, antiseptic type and manufacturing impacts, user performance (amounts of consumables used) and hospital sustainability efforts (e.g., electricity source, autoclave procedure, reusable items reprocessing, and EoL treatments).
The results indicated that user performance and hospital sustainability efforts had the greatest influence on the environmental performance of the PSP methods. In both methods, a hospital with a higher level of sustainability efforts has lower impacts on global warming, whereas the one with lower sustainability efforts will exhibit higher impacts for both methods. RM was more sensitive to hospital sustainability efforts than SM, due to the efficient design of the SM applicator. In terms of user performance, more efficient users reduce environmental impacts of the procedure. SM showed less sensitivity to user performance variability due to its pre-optimized material amount. Across all combinations of user performance and hospital sustainability efforts, SM outperformed RM, with two exceptions: 1. When the least efficient user in the hospital with lowest sustainability efforts uses 2 SM products due to human error. Of note, this sensitivity case tests inclusion of an unplanned additional applicator; it is not intended to represent materials needed for multiple or larger prep areas (see limitations). 2. When the most efficient user operates in the hospital with highest sustainability efforts.
The supplemental material shows a visualization of the sensitivity analyses for combination of user performance and hospital sustainability efforts (Figure 1 Supplemental).
Furthermore, the study chose an aqueous PVP- I solution as a conservative comparative case to SM, given the lesser CO2 impact of water relative to alcohol. However, alcohol-based antiseptics are commonly used by practitioners in the region. A sensitivity analysis was conducted comparing available antiseptics, such as alcohol-based PVP-I, aqueous PVP-I, and alcohol-based CHG (the antiseptic used in SM) Figure 4. The choice of alcohol-based antiseptics was found to notably increase CO2 impacts. Given that wasted unused antiseptic was one of the major contributors to CO2-eq in the RM system, it should be noted that the baseline RM CO2-eq impact is a conservative estimation and choice of alcohol-based antiseptic by practitioners in RM method will be calculated to be notably higher total emissions. Sensitivity analysis results graph based on antiseptic choice.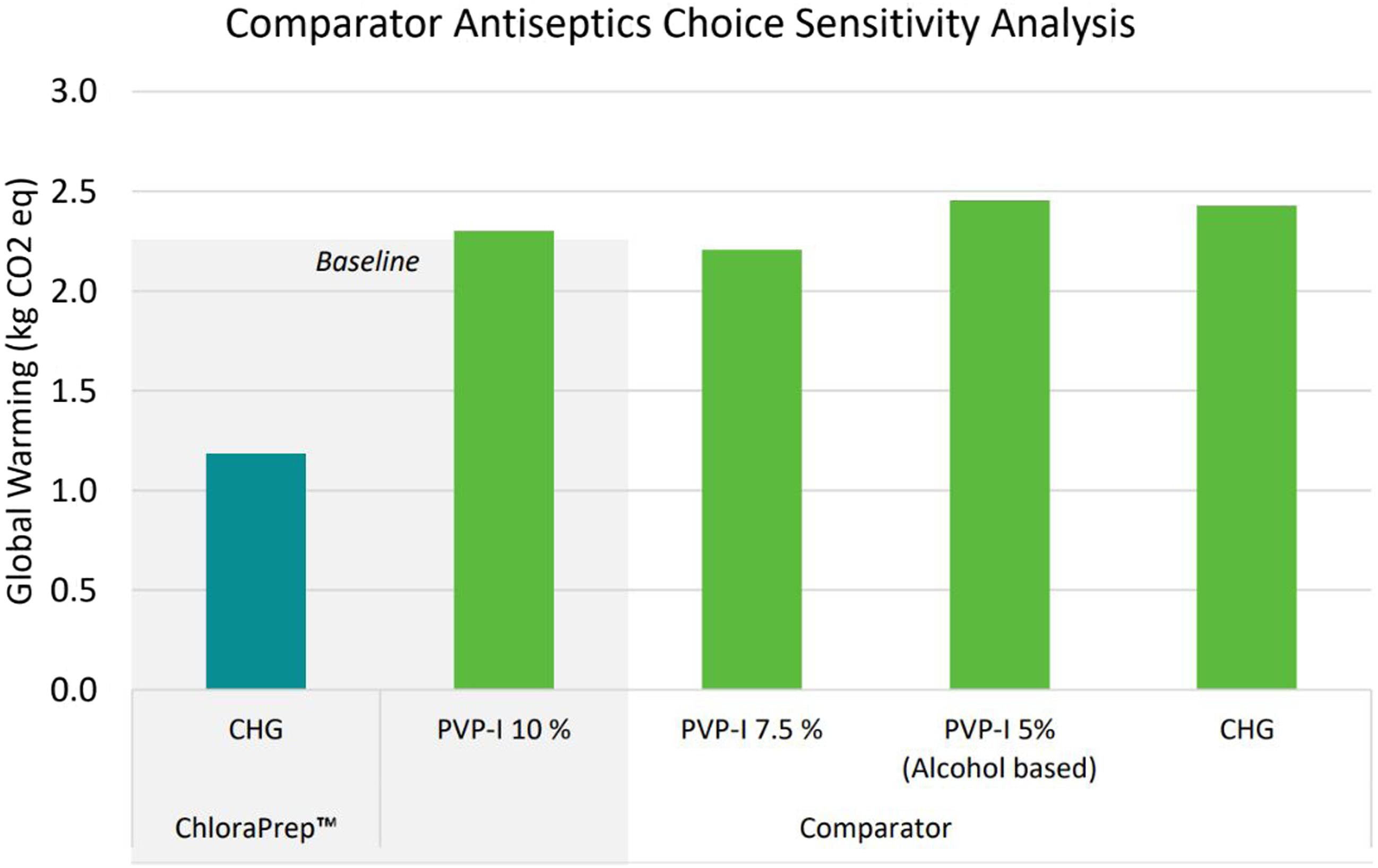
Discussion
This study examined the environmental impact of a single-use antiseptic applicator method (SM) compared to a bulk antiseptic bottle with reusable instruments method (RM) in a preoperative skin preparation (PSP) using a Life Cycle Impact Assessment. The environmental impact of SM was approximately 50% of the impact of RM in all assessed categories. The dominant emission contributor in SM was the component production of the applicator. In contrast, the key contributors in RM were the energy input for autoclaving (grid electricity and natural gas) to achieve sterility of reusables, and the quantity of excess antiseptic wasted.
Previous research has demonstrated that certain reusable medical products can reduce environmental emissions (Keil et al., 2023). However, the current study highlights the significant environmental advantages of SM in PSP within the modeled functional unit, primarily due to its lower energy consumption and greater resource efficiency. This method uses fewer additional single-use components, such as excess antiseptic and towels, which are high contributors to environmental impacts in both systems. The single-use applicator decreases antiseptic waste and towel usage by delivering a pre-optimized antiseptic volume with a controlled flow of solution to prevent pooling (Clare and Rowley, 2021). The single-use applicator can standardize the application of antiseptic and ensure compliance with the recommendations for effective PSP (Lundberg et al., 2016). In contrast, RM relies on manual antiseptic application and on-site reprocessing; impacts therefore depend strongly on sterile processing practices and can vary across facilities. Sensitivity analyses indicated that hospital sustainability efforts and user performance influence both methods and help reduce procedure impacts, but RM is more sensitive to these factors. Standardization to a single-use applicator reduces the onus on the healthcare facility to adjust practices and demonstrates consistently more resource-efficient performance across variable hospital situations, while RM displays significant variability and is highly reliant on the user. In addition, antiseptic choice affects RM results; alcohol-based antiseptics increase impacts relative to the aqueous PVP-I baseline, so RM global warming impacts are conservatively estimated under the baseline assumption.
Using single-use applicators in PSP could be one avenue for improving the carbon footprint within ORs, which are known for being high contributors to waste (Cunha and Pellino, 2023; Kwakye et al., 2011). Considering the reported annual global tally of laparoscopic pelvic and abdominal surgeries alone (Matrick, 2023), adjusted to represent the European region (Kristensen et al., 2014), the choice of SM over RM in PSP could equate to yearly savings of 1116 tons of CO2. This is approximately equivalent to the annual carbon footprint of 172 Europeans (Tiseo, 2023). Given that nearly all surgeries require PSP, the choice of lower-emission methods could yield much higher possible reductions overall.
Limitations: This study modeled European PSP practices for laparoscopic surgery, which may limit generalizability. PSP materials can vary by clinician practice and institutional policies and where primary data were unavailable, secondary assumptions were applied. Sensitivity analyses were performed to address reasonable variation in practice. While scenarios requiring multiple applicators were not modeled, the impact of both methods would both be expected to increase with prep and may experience step changes due to fixed antiseptic sizes. However, dedicated modeling would be required for these additional scenarios.
The study challenges the assumption that reusable systems always result in lower environmental impacts. Despite the perceived benefits associated with reusable items, emissions from reprocessing, single-use consumables, and reliance on user and hospital management can have a significant impact on CO2-eq emissions. In this LCA comparison, a single-use applicator showed a clear advantage versus the comparator in reducing CO2-eq emissions. This highlights the need to scrutinize the life cycle when making comparisons as part of surgical sustainability.
Supplemental material
Supplemental material—A comparative life cycle assessment of the environmental impact of preoperative skin preparation, single-use applicators versus bulk antiseptic with reusable instruments
Supplemental material for A comparative life cycle assessment of the environmental impact of preoperative skin preparation, single-use applicators versus bulk antiseptic with reusable instruments by Kinga Szalecka, Eoin Merrigan, Ryan Forrey, Vyjayanthi Kambam, Matthieu Boisson, Zeynab Yousefzadeh, Millie Calistri-Yeh, Di Lu in Journal of Infection Prevention.
Footnotes
Acknowledgments
Members of the critical review board: Richard Helling, Cassandra Thiel, Guido Sonnemann.
Ethical considerations
Data collection and life cycle assessment for BD specific products were conducted by BD associates under predefined, transparent methods. A thirdparty company independently executed all remaining analysis, assessments and the overall review. All data inputs were limited to technical and environmental parameters and were evaluated using established LCA methodologies.
Consent to participate
This study did not involve human participants, animals, or patient-level data. As a result, review by an ethics committee and informed consent were not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the BD.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors disclose the following sources of financial support and conflict of interest: Zeynab Yousefzadeh was an employee of EarthShift Global during the duration of research detailed in this paper, and her work received funding from Becton, Dickinson and Company for this project. Matthieu Boisson is a Professor of Anesthesiology and Intensive Care Medicine at the Université de Poitiers, France, who received funding from Becton, Dickinson and Company for this project. Kinga Szalecka and Eoin Merrigan were employed by Becton, Dickinson and Company during the period of this study. Ryan Forrey, Vyjayanthi Kambam, Millie Calistri-Yeh, Di Lu are currently employed at Becton, Dickinson and Company.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.