
Abstract
Background
A clean healthcare environment is the foundation of both antimicrobial stewardship and delivery of sustainable healthcare. Clinical staff are responsible for cleaning medical equipment and some aspects of the healthcare environment.
Aim
To improve the clinical cleaning on a busy PICU in a tertiary referral hospital in England.
Methods
This was an educational continuous Quality Improvement (QI) project using opportunistic and targeted one-to-one education and training for clinical staff. Cleaning audits were conducted weekly throughout the study period and the results mapped against monthly bed occupancy data. The PDSA cycle (plan, do, study, act) was used to review actions, outcomes, and impact and consider further work every month by the study team.
Results
Key themes emerged for improvement around the training delivered on cleaning, both formally through mandatory study days and informally through the cascade of knowledge to new starters. The cleaning ‘hotspotsʼ identified via audit and how these were communicated to the team were also targeted. The multi-mode interventions, delivered by both Infection Prevention link nurse unit staff and a Clinical Auditor/ Educator, were successful in building and maintaining excellent cleaning standards within the ward.
Discussion
Co-creation of cleaning interventions enabled a supportive environment to be developed with staff demonstrating a high level of understanding and commitment to environmental cleanliness. This approach would be scalable across multiple areas of the hospital with the short-term support of a Clinical Educator or Infection Prevention Nurse.
Background
Recognised by Florence Nightingale as an important aspect of the patient’s safety and recovery pathway, clinical cleaning of the healthcare environment has long underpinned good care and is the cornerstone of sustainable healthcare. By ensuring the patient environment is clean, particularly in high acuity areas of the hospital delivering invasive care such as the Intensive Care Unit (ICU), the clinical team reduces the risk of healthcare-associated infection (HCAI) occurring. This is key to both reducing healthcare carbon emissions and supporting antimicrobial stewardship as HCAIs are associated with more antibiotic use, more single-use plastics, more personal protective equipment (PPE), longer hospital stays, higher acuity care, and poorer patient outcomes (Lee et al., 2024). The financial cost of HCAIs to the NHS each year has been estimated at over £1 billion (Mackley et al., 2018) but this does not include the social impacts of the loss of education attendance and contributions to the community, the economic cost of loss of earning potential (for the patient and for family), or the personal impact for families when a loved one is disabled or dies from preventable infections (Mo et al., 2019). The Epic3 guidelines for prevention of HCAI in the NHS (Loveday et al., 2014) are clear that every healthcare professional has a part to play in ensuring the cleanliness of the healthcare environment and clinical equipment.
The continuous improvement project reported here used the PDSA cycle to improve clinical cleaning in a paediatric ICU (PICU) in a no-cost way that would be self-sustaining. The area had historically performed well in cleaning audits, but at the point of intervention design there had been several consecutive cleaning audit failures. The key members of staff were two infection prevention (IP) link nurses and a Clinical Auditor/ Educator (CAE) with a remit for supporting clinical teams across the hospital with cleaning. The aim was to understand the drivers of poor performance and factors contributing to previous strong performance, and to co-design a bespoke programme of educational support which would enable greater cleanliness to be achieved consistently, beyond the time frame of intervention.
Methods
Audit methodology
The cleaning audits were conducted by a team internal to the Trust but external to PICU. The team consisted of three trained auditors and one CAE, and the composition of the team was consistent throughout the study period. The weekly audit was randomly assigned to one of the four auditors. The audit was based on the National Standards of Healthcare Cleanliness (2021), with elements assigned to either the clinical or domestic team. It was only the clinical cleaning that was used for this project. The software used for recording the audit was FM First (v.2024.1, Asckey Data Services Ltd). Ethical consent for the project was not required as it falls under the continuous quality improvement processes of the Trust and the standard audit cycle.
Educational interventions
The opportunistic education sessions delivered on the unit were written up as field notes immediately following intervention. The AfC band of the staff spoken to and a summary of topics raised by staff were recorded, along with broad themes of the educational content delivered by the CAE. The IP link nurses requested the education interventions started with nurses who had been on the unit for less than 2 years, and subsequently expanded to include clinical staff from all bands. The informal conversations typically lasted around 15 minutes, partly guided by clinical staff asking questions and demonstrating current knowledge. The aspects covered included those identified by the IP link nurses and CAE as important – namely the clinical and domestic responsibilities for cleaning the ward, the timing of cleaning, and the hotspots that were frequently identified on the audits. These sessions were conducted approximately fortnightly over a period of 6 months. Signage about the environmental and social impacts of a clean, sustainable hospital was promoted locally and at Trust level.
IP link nurses’ interventions
The IP link nurses on the unit identified the frequency and content of mandatory training as one aspect that could be changed to improve visibility of cleaning to the clinical team. They implemented more frequent training with a greater emphasis on cleaning. Additional signage was designed and used to highlight hotspots for cleaning and reminding staff what clinical cleaning responsibilities were. Celebratory emails were used as positive feedback.
Results
Co-creation of the programme
The partnership started in November 2023 following some low cleaning audit scores and was initiated by the CAE. At the time the partnership commenced, senior staff identified a junior skill mix and staffing pressures as being factors for consideration. One of the Senior Sisters of the unit, who was also an Infection Prevention (IP) link nurse, was the key contact, and they agreed to work together on a programme of education and raising awareness of the importance of cleaning as part of the IP measures deployed in an acute care setting. This team expanded to include a Band 5 IP link nurse, and the three met regularly throughout the programme to assess progress and discuss ongoing work. The desired outcome was clearly articulated and the drivers and potential restorative actions were identified for implementation (Figure 1). Driver diagram for the programme of interventions aimed at increasing effectiveness of clinical cleaning as part of the hospital sustainability plan.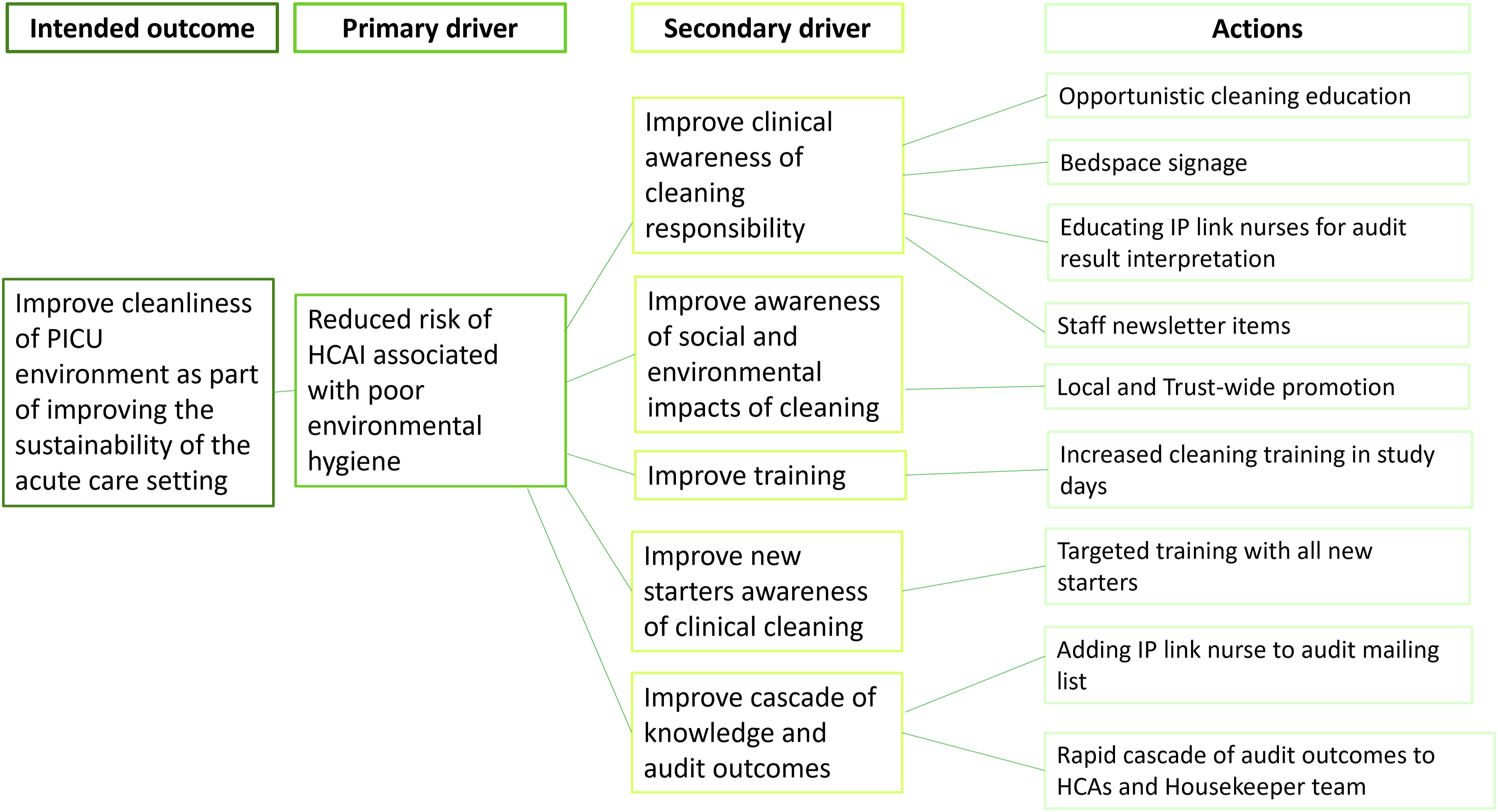
Clinical Auditor/ Educator support time
A Summary of the Staff Groups Spoken to During CAE Interventions, the Number of Times Groups Were Spoken to, and the Topics That Were Raised and Discussed.
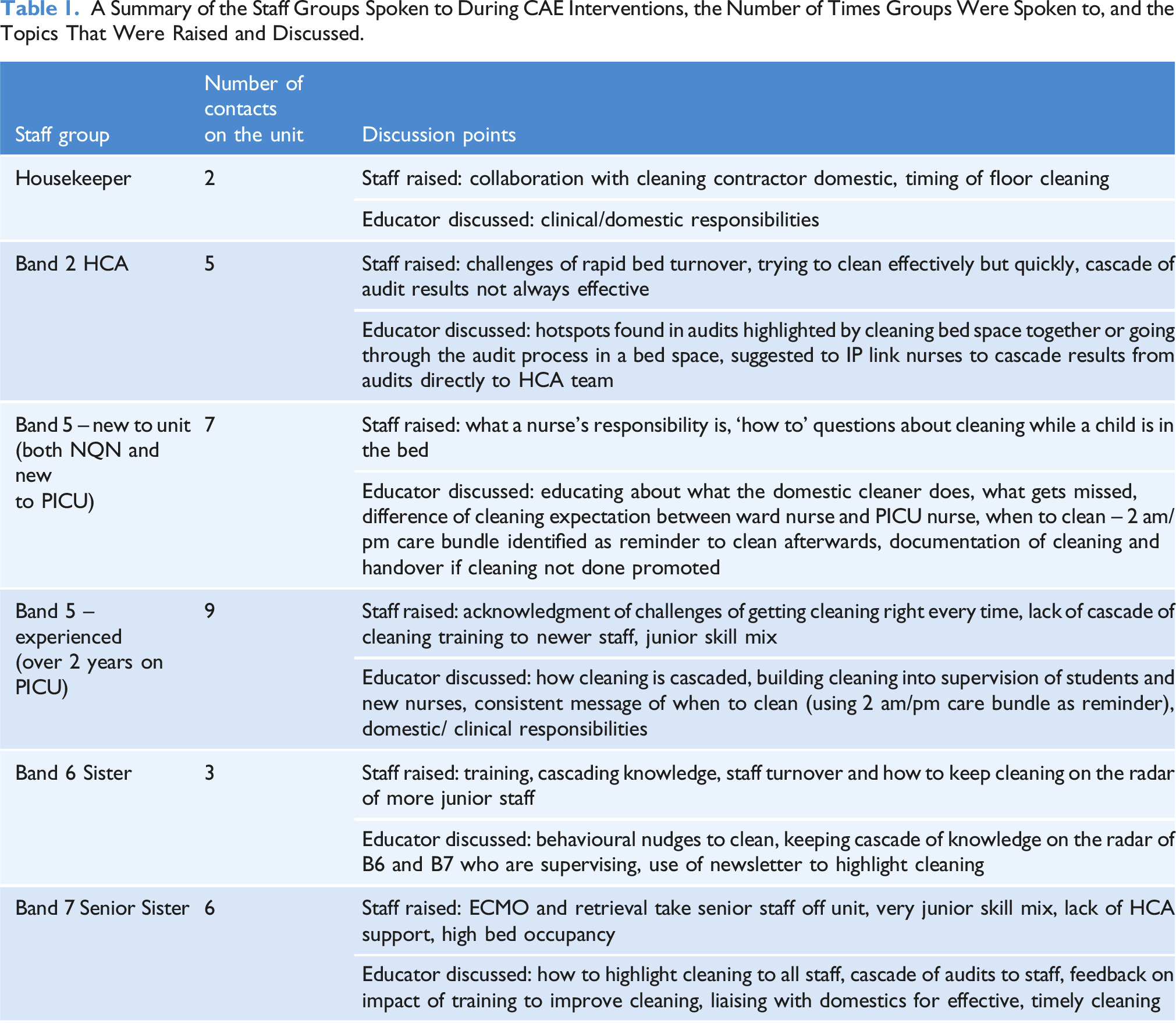
One of the key themes that emerged from experienced staff was the perception of a fractured cascade of training and learning around clinical cleaning responsibilities. As well as delivering routine Level 2 and Level 3 care to both medical and surgical patients, the trial unit had the capacity to perform extracorporeal membrane oxygenation (ECMO) and supported a retrieval service from other hospitals across a wide geographical area. Both of these services had the potential to take senior staff off the floor, leaving a more junior skill mix in the main body of the unit. There was a shared desire to increase education about cleaning during the probation training delivered to new nurses and junior staff. Students and newly qualified nurses (NQNs) were identified as being receptive to teaching about the importance of cleaning in the PICU and the specific role of the nurse in cleaning the bed space and associated equipment. Experienced PICU staff reported that nurses moving from a paediatric ward to PICU found the change in expectation more difficult as the majority of cleaning on wards is undertaken by housekeepers and healthcare assistants, whereas occupied bedspaces in PICU are the nurse’s responsibility to clean. The use of behavioural nudges, such as offering to supply cleaning equipment, to promote cleaning was described as a technique used by senior staff alongside more direct supervision such as asking if cleaning had been done, holding a tidy bedspace competition, and offering to do the cleaning while covering junior staff breaks.
Changes made as a result of new learning and interventions
The changes implemented by the team are summarised in Figure 2. These included increasing the frequency of IP training and delivering this to smaller groups. This ensured that if staffing levels required the training to be cancelled, the impact on the whole team was smaller and there were more opportunities to join another group. The IP training continued to be delivered as part of the ‘Statutory and Mandatory’ training required within the Trust but had more focus on cleaning, and both documentation and handover of cleaning were promoted during training and staff interactions. The exact duration, specific content and delivery were flexible to meet the training needs of the group, and the overall hours given to the IP link nurses did not change. The role of the CAE and cleaning audit team were promoted via the staff newsletter, and joint emails from the implementation team celebrating milestones of good audit results (for example, a month, 2 months of audit success) were used to build an appreciative feedback culture. The CAE also highlighted a spell of good audit performance to staff in person when she was visiting the unit, which was always well received. The successful multi-modal approach taken to secure consistent clinical cleaning.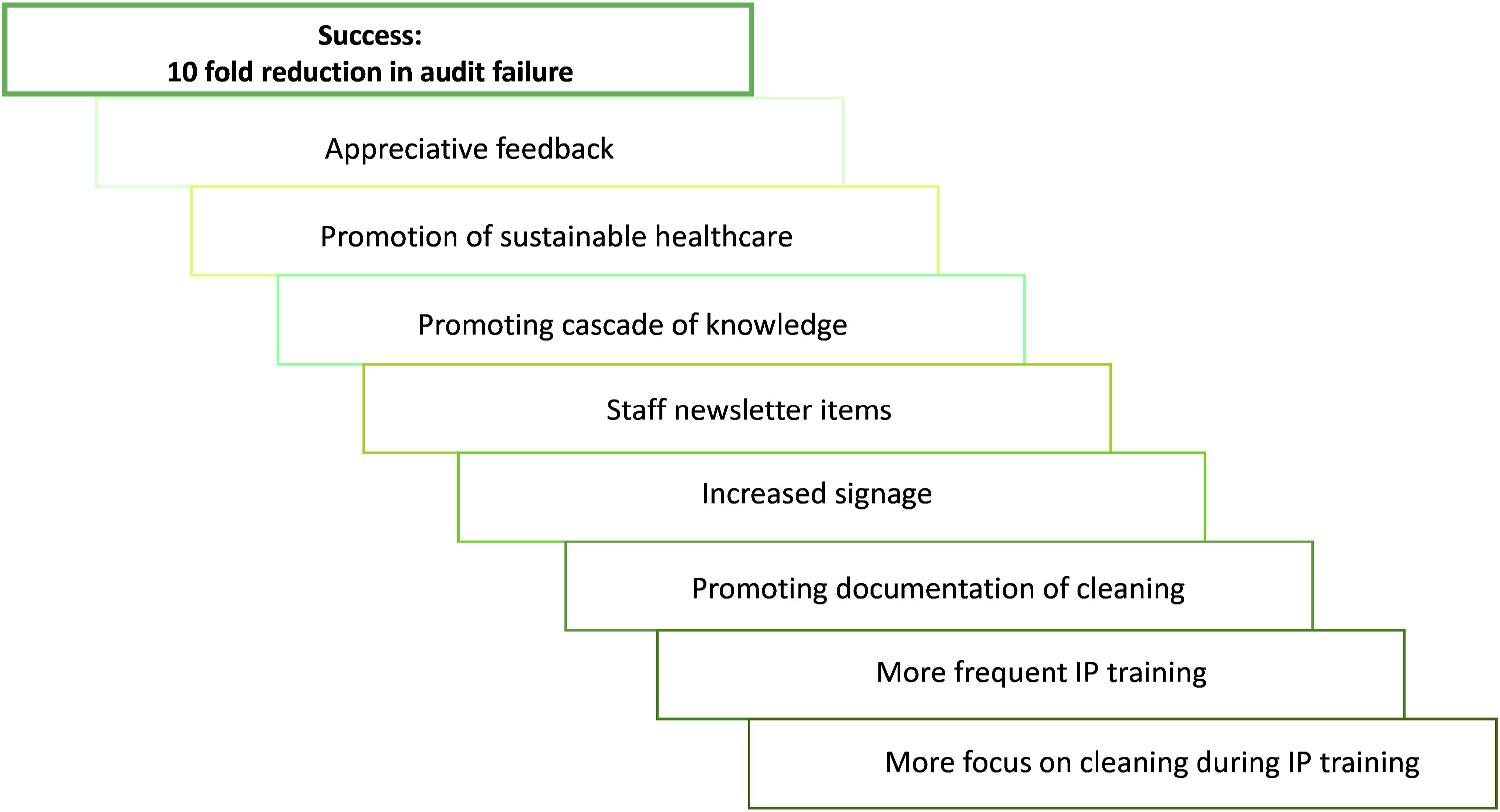
Signage about clinical cleaning responsibilities was developed and displayed in bedspaces, signage was refreshed around hotspots in the ward, and the role of cleaning in delivery of sustainable healthcare was promoted both locally and across the Trust. More experienced staff were encouraged to promote cleaning to new staff during their supervised introduction to the ward. Together, these multi-modal interventions gave a dramatic reduction in audit failures. Between February and July, the success rate of cleaning audits meeting the required standard was over 95%. Having re-established the training cascade, adapted the IP training to be better suited to the current needs of the team, and promoted clinical cleaning as a keystone of sustainable healthcare, the period of more intense support from the CAE was finished. The IP link nurses were empowered to enable their team to deliver ongoing excellence. The success of the CAE and PICU collaboration was regularly celebrated at the Trust weekly cleaning meetings, the monthly overview meeting, and at the IP Trust meeting, raising the profile of cleaning and the opportunity clinical areas had to work with a dedicated CAE.
Bed occupancy and cleaning audit performance
Over the study period, bed occupancy peaked in December but was consistently high from October to May (Figure 3). The relationship between emergency and elective admissions was inversely proportional as expected – when emergency admissions were high, the capacity for elective admissions was reduced and these dropped. Using Prasad et al. (2022), the carbon footprint of the unit was estimated to peak in December with the high bed occupancy. Bed occupancy, the number of elective admissions, and the number of emergency admissions on the PICU over the study period. The estimated carbon footprint is indicated using the Prasad et al. (2022) figure of 138 kg CO2e per bed day for ICU care, multiplied by the total number of bed days in the month. The black boxes indicate months when the average cleaning score was below the expected standard.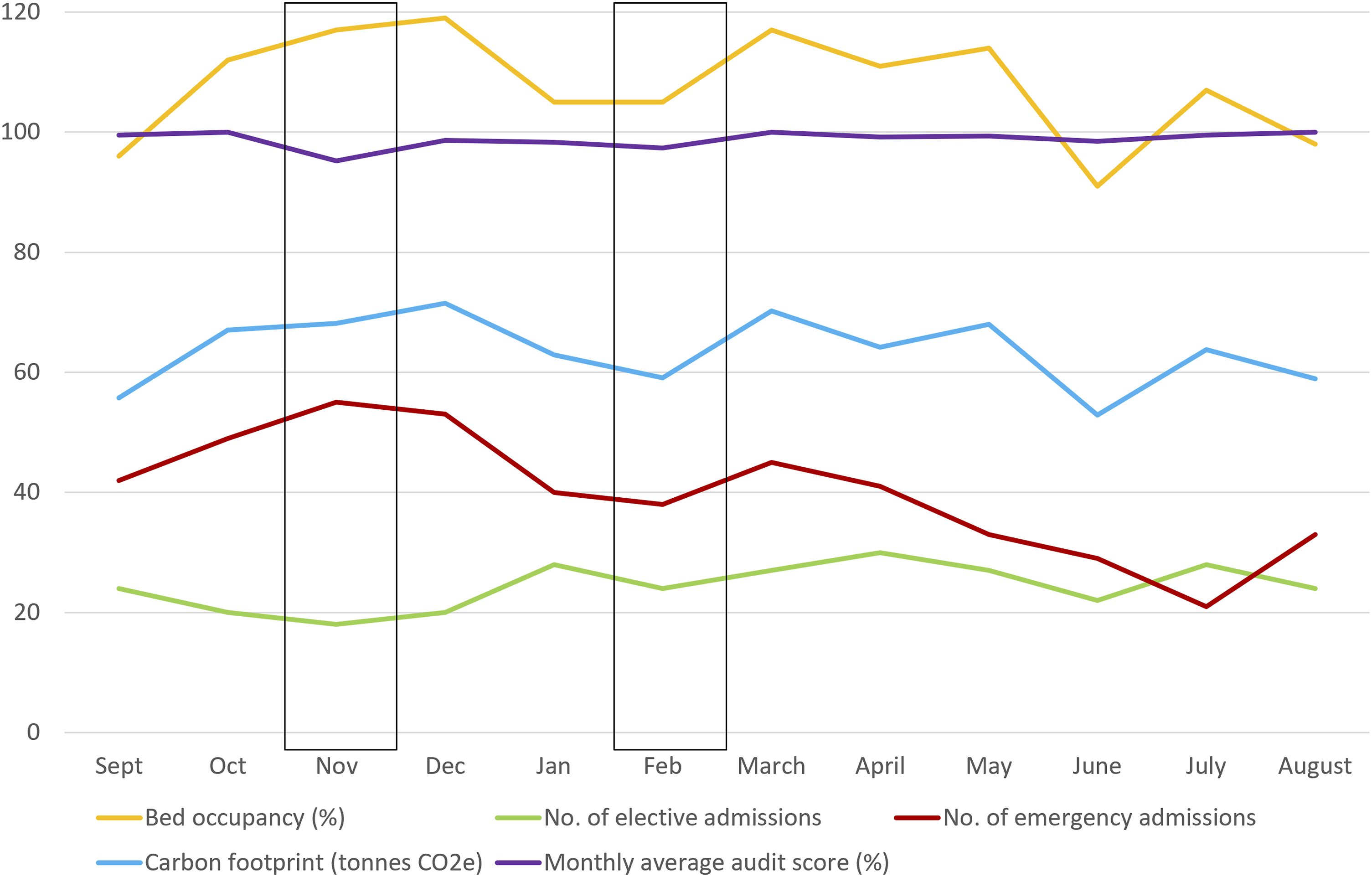
Historically, the environmental cleanliness of the unit had reached the FR1 (Functional Risk category 1) standards set out in the National Standards of Healthcare Cleanliness (2021). This changed in October 2023 with only 50% of audits meeting the expected standard over the next 4 months, as shown in Figure 3 (purple line) and in Figure 4. This period coincided with the high bed occupancy outlined above (yellow line), but while the bed occupancy remained high through April and May, the outcome of the cleaning audits improved from February onwards (Figure 4). This suggested that although staff workload and bed pressures may have been the trigger for poor cleaning performance, they are not inevitable cause and effect. The clinical cleaning audit results for PICU over a period of 12 months. The red shaded area indicates failure to meet the required standard, with the green shaded area showing the audits achieving the required standard, as audited against the National Standards of Healthcare Cleanliness (2021).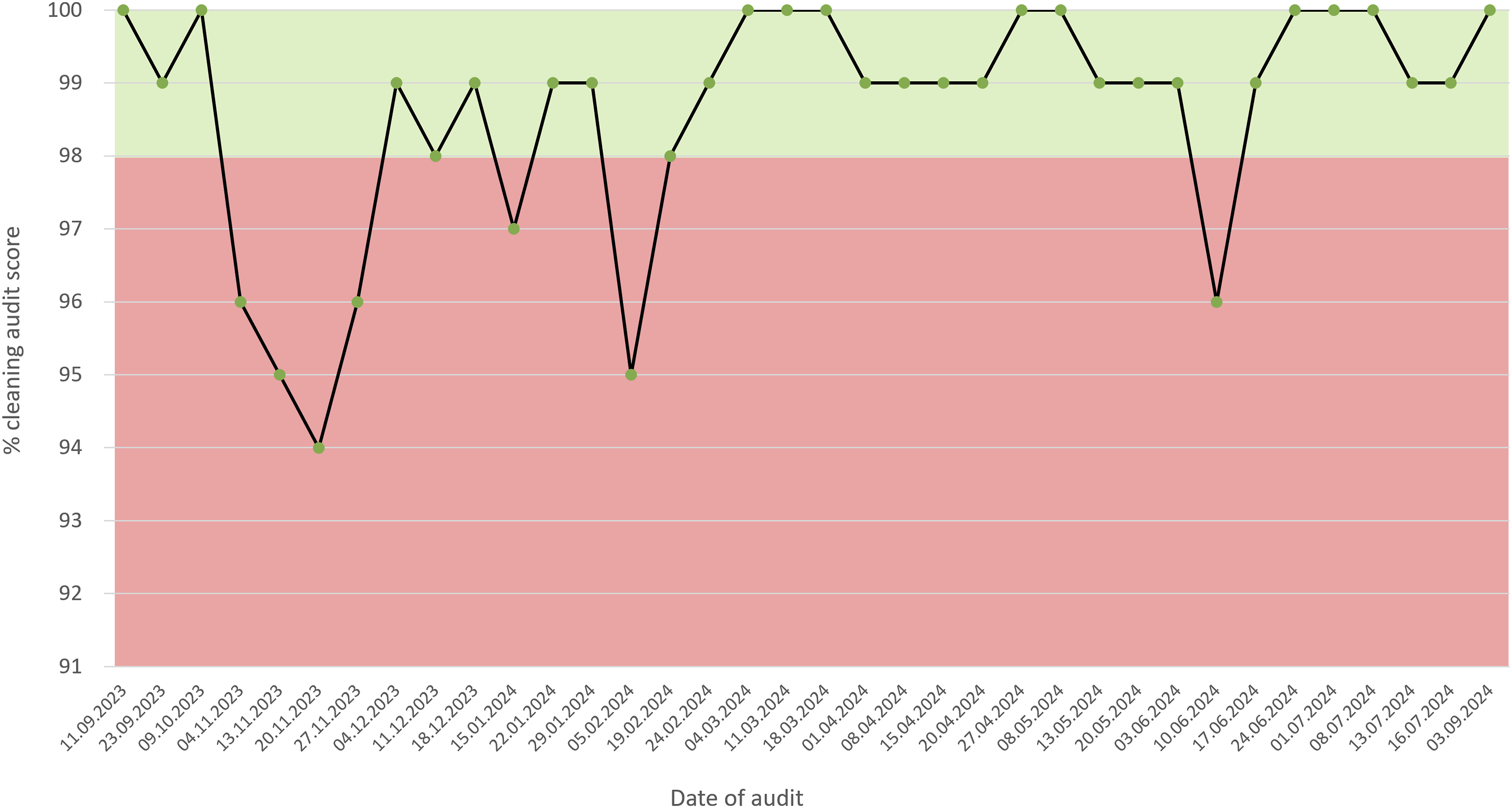
Hotspots for cleaning
There were clearly identifiable elements that failed on multiple occasions, suggesting that while most cleaning was effective and at suitable intervals (no audit scored less than 94%, Figure 4), there were hotspots within the unit that were being routinely missed. The key contaminants identified in the environment were blood and dust, and the items most likely to be marked were the sharps/ pharmaceutical bins, beds and cots, and the general purpose trolleys present in each bedspace to hold the basic nursing equipment (Figure 5). Key terms highlighted in PICU cleaning audits over 12 months. The percentage displayed is the number of times the term was reported divided by the total number of elements failed across all audits in the timeframe.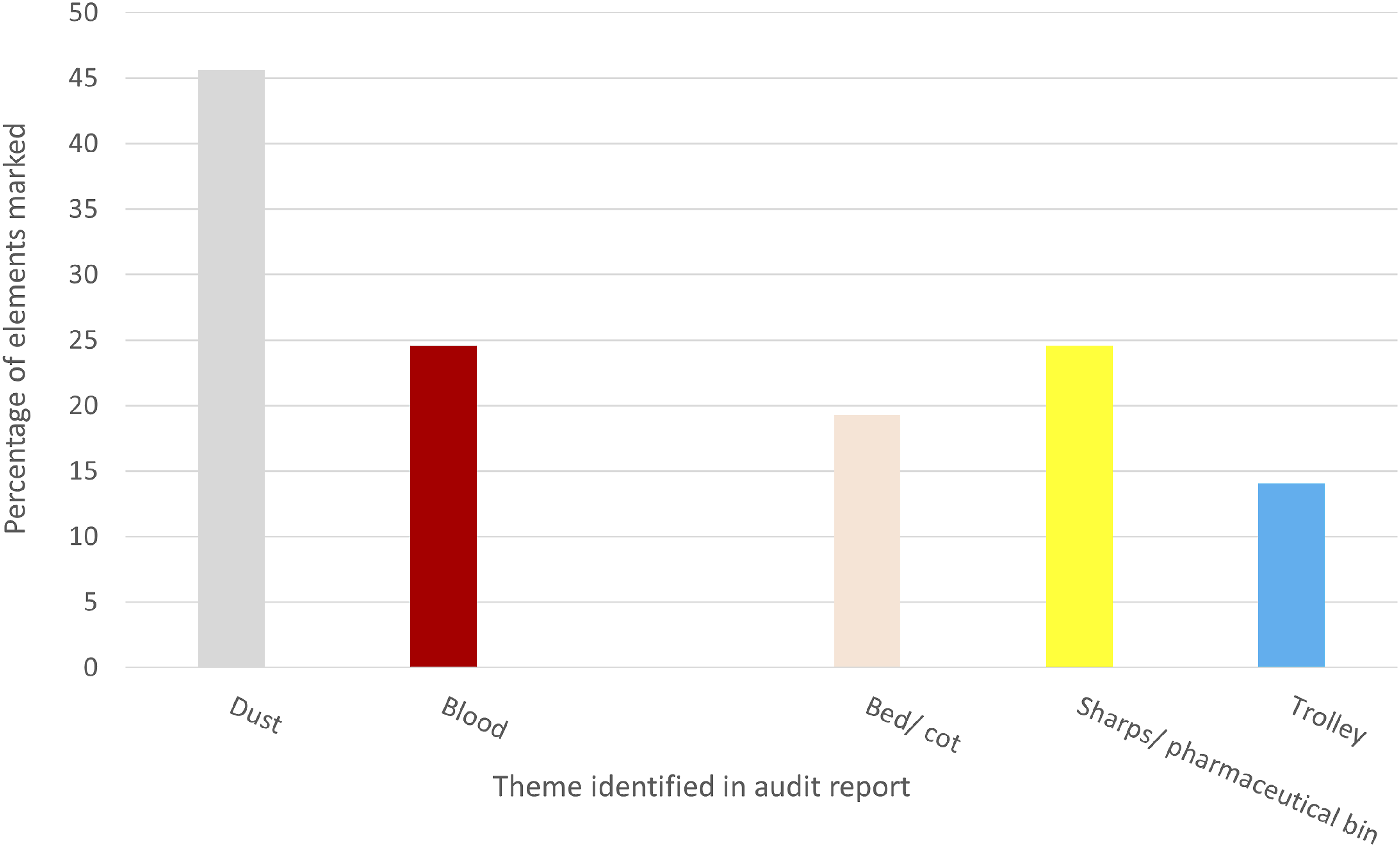
These findings, and the consistency of the cleaning ‘hotspots’, enabled an effective, targeted education programme to be delivered.
Discussion
Clinical cleaning is part of the nursing workload in any care setting but is particularly significant in the intensive care unit. In this study, bed occupancy remained high throughout the period but cleaning standards improved from early on suggesting that thorough cleaning is not dependent on staff workload and that the educational interventions were successful at raising standards. While the high occupancy and number of emergency admissions over the beginning of the winter period may have contributed to the poor cleaning performance, the relationship between effective cleaning and workload is clearly more complex than a simple correlation. The audits were conducted by the hospital cleaning audit team and they were aware of the improvement project. While this may have had an impact on the audit outcome, marking against a set standard reduces the likelihood of this. The CAE worked with many areas across the hospital and not all areas experienced improved audit outcomes, suggesting that this was a valid result.
The CLEEN study has recently shown the efficacy of cleaning in reducing the occurrence of HCAI (Browne et al., 2024), and as HCAIs are associated with increased length of stay (Manoukian et al., 2018), there are strong grounds for promoting cleaning as a key part of sustainable healthcare. The results from this study did not align well with the CLEEN study findings. The trial unit experienced few HCAIs over the study period, and these showed only a slight association with cleaning audit scores. HCAI rate did not map to bed occupancy, nor the number of emergency versus elective admissions. While the presence of dust on sharps bins and trolleys may be considered ‘low risk’ environmental contaminants for spreading the organisms responsible for HCAIs, the presence of blood splash in the environment and contaminated beds would have been thought to be ‘high risk’. It may be that the low number of HCAIs over the period provides insufficient data to see a trend or association. The CAE did not have access to alternative or additional methods to assess cleanliness, so the lack of correlation seen here between cleaning and HCAI may suggest that additional measures such as UV light reveal for body fluids may enhance the value of auditing.
The time spent cleaning and the person responsible for cleaning are both factors that have been highlighted in the nursing literature (Matterson et al., 2024; Mitchell et al., 2021). In this study, housekeepers and healthcare assistants (HCAs) played an important role in cleaning empty bed spaces and communal areas while nurses were responsible for the occupied bed spaces. Saito et al. (2015) cited in Scott et al. (2017) reported housekeepers as spending nearly twice as long cleaning during a shift as the registered nurses. In this study, the housekeepers played an active role in giving feedback of the challenges of cleaning in the high pressure environment of rapid turnaround times during high occupancy, and the need for more rapid dissemination of the audit results to enable greater learning and enhanced rectification. One of the actions arising from the PDSA cycle was to improve the cascade of audit results to the housekeepers and HCA more rapidly, to enable more timely remedial action. The roles and cleaning responsibilities of each member of the clinical team were well-understood and reiterated during the study. These factors were thought to contribute to the success of clinical cleaning on the unit.
Co-creation of the programme was key to success. Co-creation is typically referred to in the academic setting but transfers well to the clinical setting and increases the likely acceptance of interventions and successful implementation of changes (Laugaland et al., 2023). Rather than the CAE designing an intervention programme for the unit, all interventions were the result of co-creation with unit staff enabling the identification of shared goals, empowering unit staff to build processes that would support long-term behavioural change, and joint celebration of success (Ng, 2014; Den Boer et al., 2017). At the time of this project, the CAE was also working with three other high acuity areas within the Trust to co-create more effective cleaning strategies for their areas, and had already completed a similar project with one of the specialist theatres with similar outstanding results. This was a low-cost intervention which enabled a long term positive behavioural change in clinical cleaning. The impact on antimicrobial stewardship and reducing the environmental impact of high acuity care will be seen over the coming months and years.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.