
Abstract
Aim
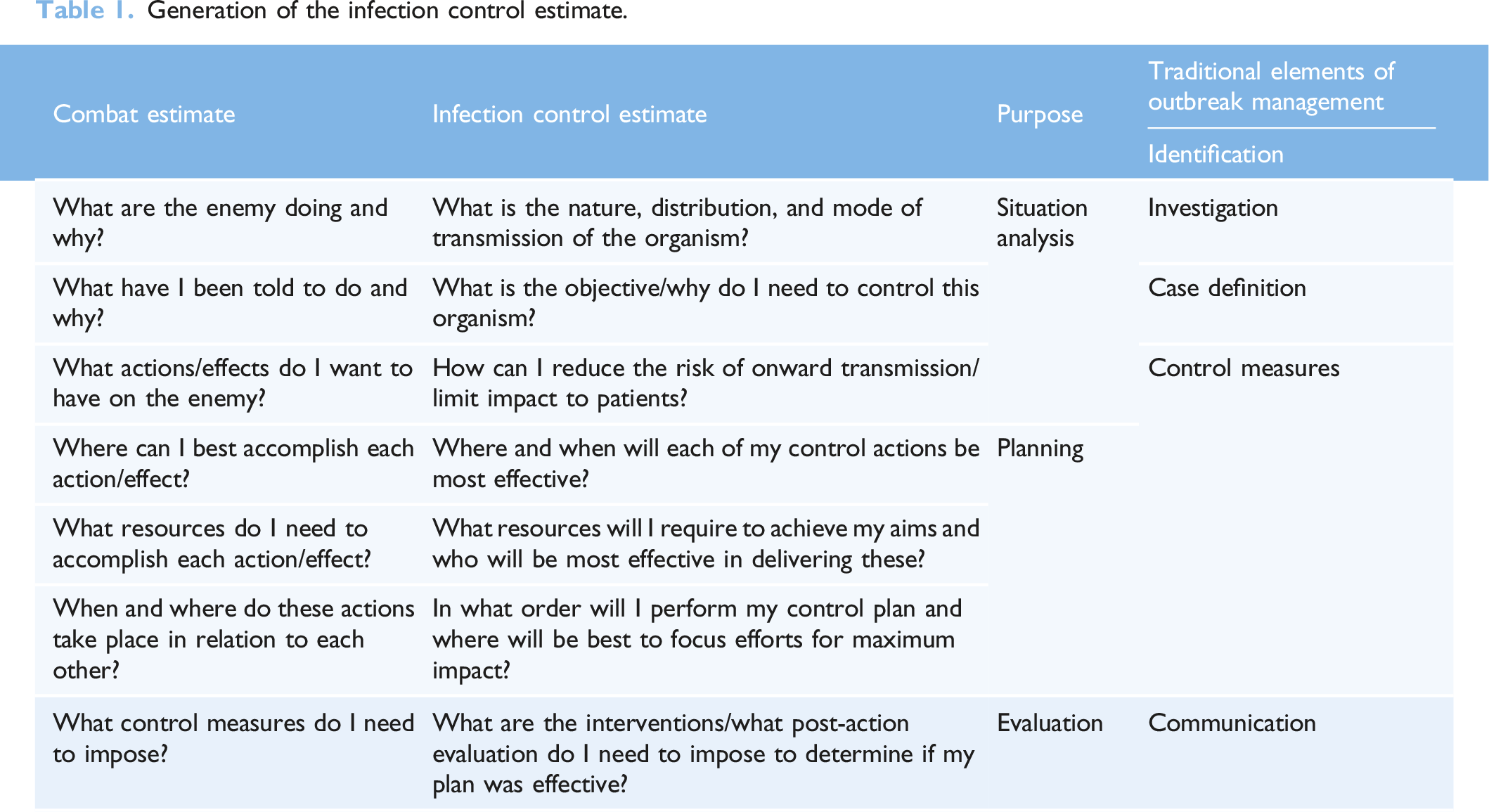
An Infection Control Estimate (ICE) Tool was developed based on a previously published concept of applying military planning techniques to Infection Prevention and Control (IPC) management strategies in the acute healthcare setting.
Methods
Initial testing of the outbreak management tool was undertaken in a large acute hospital in the North-West of England during a localised outbreak of COVID-19. The tool, developed using Microsoft Excel, was completed by trained IPC practitioners in real-time to log outbreak details, assign and manage meeting actions and to generate surveillance data.
Results
The ICE tool was utilised across five outbreak control meetings to identify and allocate tasks to members of the outbreak control team and to monitor progress. Within the meetings, the tool was used primarily by the trained IPC Specialist Nurses who were guided by and entered data into the relevant sections. Feedback indicated that the tool was easy to use and useful as the sole repository of outbreak information and data. Suggested improvements following the testing period were made and additional functionality was added.
Conclusion
Utilisation of the ICE tool has the potential to improve our understanding of the efficacy of currently employed outbreak management interventions and provides a cognitive support and targeted education for teams responsible for the management of outbreaks. It is hoped that by guiding teams through an outbreak with prompts and guidance, as well as facilitating collection and presentation of surveillance data, outbreaks will be resolved sooner and risks to patients will be reduced.
Introduction
The COVID-19 pandemic generated numerous challenges to healthcare services and has in many cases hastened a transition towards digital ways of working. These challenges highlighted several key issues related to the management of outbreaks of infectious diseases. Firstly, an appreciation of the importance of robust and timely datasets to support decision making has been realised during contact tracing and epidemiological modelling efforts (Budd et al., 2020). Secondly, the paramount importance of human factors and ergonomics, ensuring that workflows and processes are effective, engaging and barriers to outbreak interventions are recognised and addressed (Gurses et al., 2020).
Generation of the infection control estimate.
This article will discuss the first proactive application of this novel outbreak management tool during an outbreak of COVID-19 in a large acute hospital in the North-West of England.
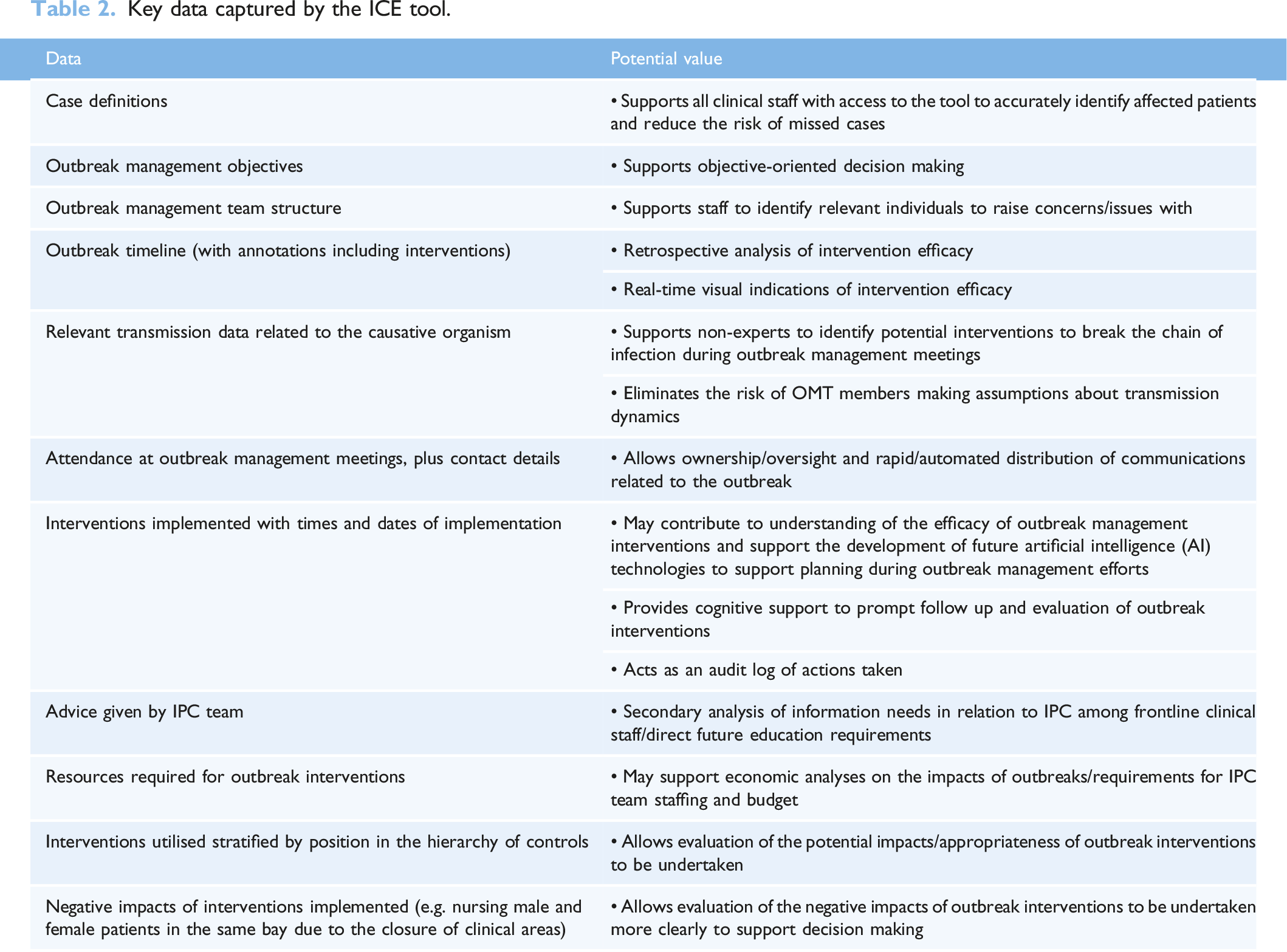
Key data captured by the ICE tool.
Background of outbreak
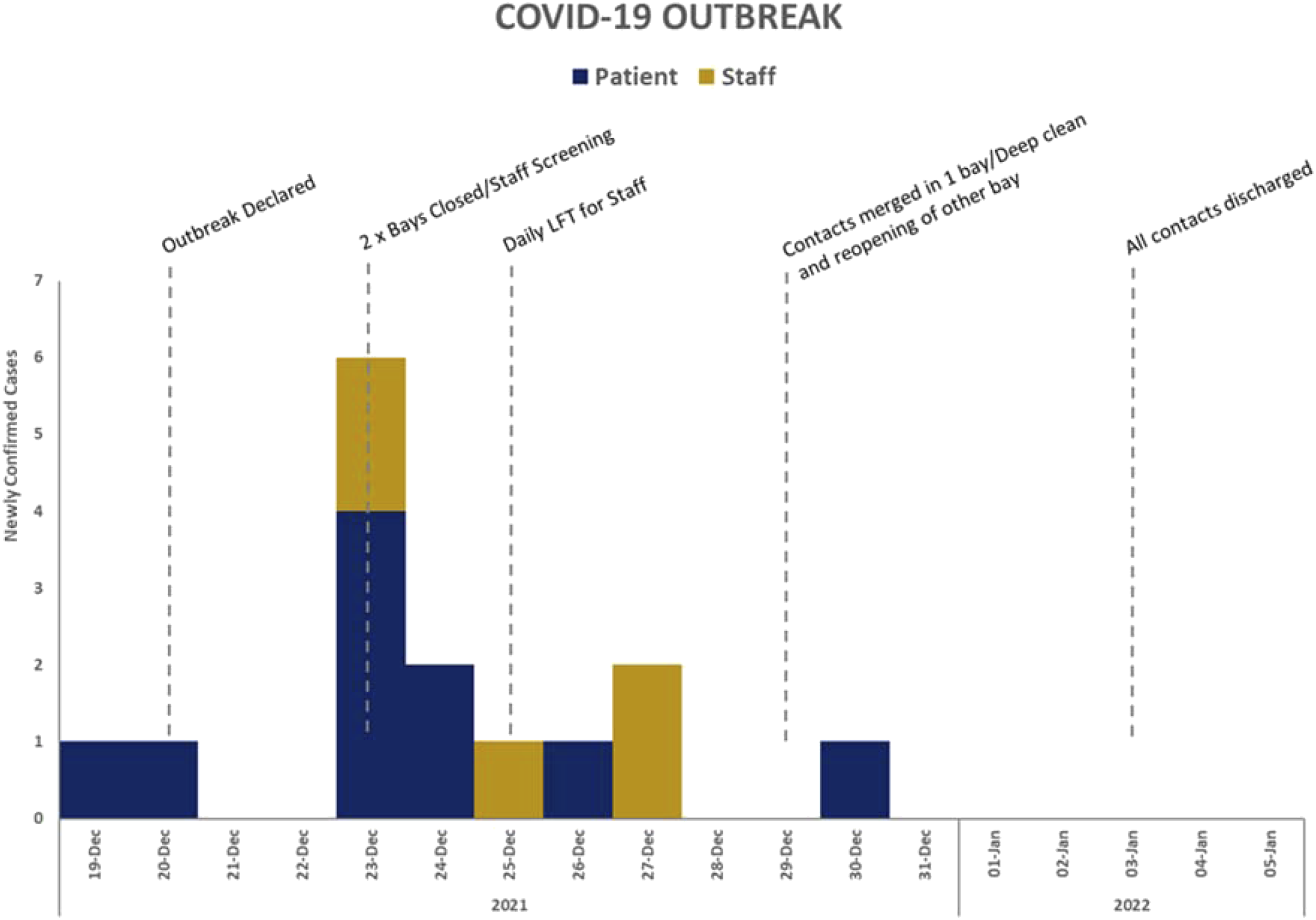
In 2021, the ICE protype tool was used for the first time during a live outbreak at a hospital in Northwest England. The outbreak concerned SARS-COV-2 and lasted 44 days, during which time 36 patients were infected. The outbreak was contained to a single ward.
The ICE prototype
The ICE tool prototype was used to document information related to the outbreak and answers the seven questions which constitute the estimate (Wynn et al., 2020). For example, the front sheet, as seen in Figure 1, contains data related to the causative organism, its modes of transmission, a case definition and an epidemic curve which addresses question one (What is the nature, distribution and mode of transmission of the organism?). In addition to providing a clear objective for outbreak management addressing question two (What is the objective/why do I need to control this organism?). Following the initial development of the prototype tool, it was tested using data from a historical outbreak to help identify gaps in the data collection or additional data entry fields which may support the management of outbreaks which could be included. Figures 2 and 3 show data visualisation capabilities of the ICE prototype. The ICE prototype front sheet/user interface. Hierarchy of control distribution for interventions used during the outbreak. Visualisation of the outbreak using epidemiological and intervention implementation data.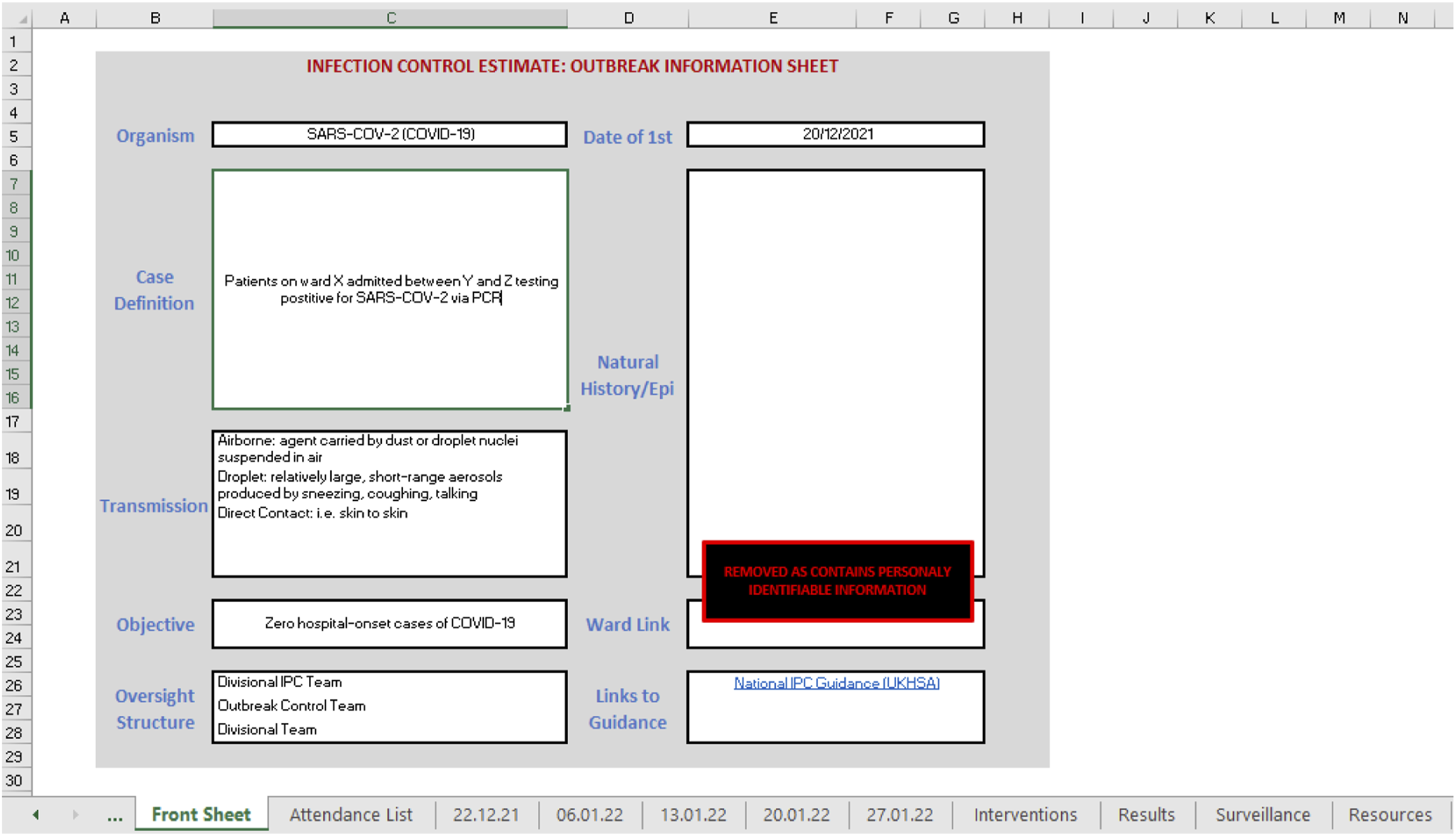
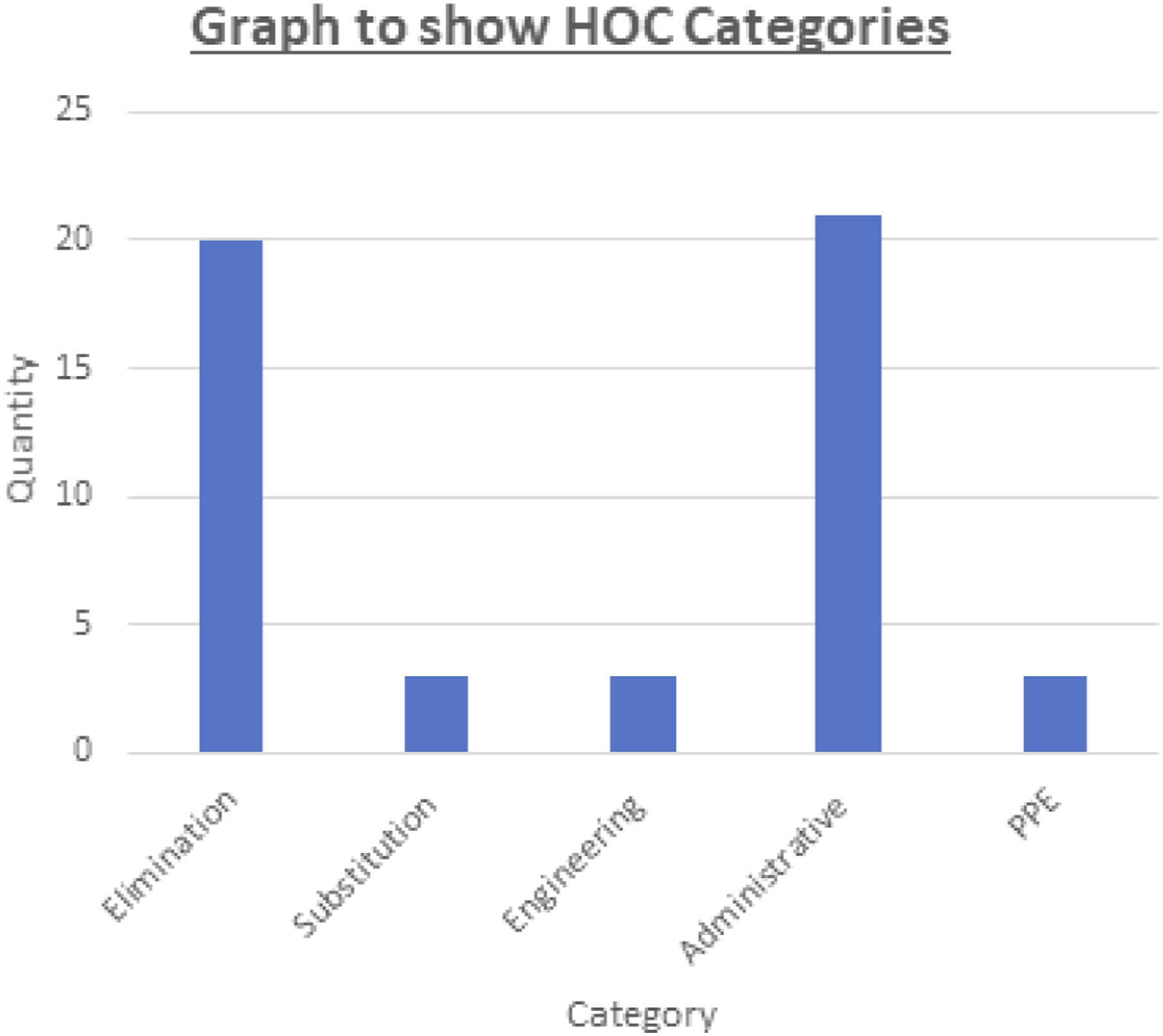
Throughout the outbreak, the ICE prototype tool was used to record key data related to the outbreak in addition to being used to help plan and evaluate control measures. A retrospective analysis of the ICE tool used during the outbreak identified 53 interventions employed. These were automatically analysed by the tool and categorised into the relevant hierarchy of control (HOC) categories (Centers for Disease Control 2015). This analysis highlighted that the majority (n = 41) of outbreak interventions were either elimination or administrative interventions with the minority of interventions (n = 12) representing substitution, engineering controls or personal protective equipment-based interventions.
The tool was utilised across five outbreak control meetings to identify and allocate tasks to members of the outbreak control team. The tool also indicates when these tasks were completed. Within the meetings the ICE tool was used primarily by the trained infection control specialist nurses who were guided by and entered data into the tool. It was reported that the tool was found to be easy to use and captured all necessary data, although new data collection fields were suggested during the outbreak including detailed recording of issues and negative impacts of management interventions.
Conclusion
The ICE prototype is the first digital tool which centralises key data related to the management of outbreaks in the context of inpatient hospital settings. The data captured within the ICE tool has the potential to improve our understanding of the efficacy of currently employed outbreak management interventions, the economic impacts of outbreaks and provides a cognitive support and targeted educational tool for teams responsible for the management of outbreaks. By ensuring that all aspects of the ICE seven questions are addressed within the tool, teams can be more confident that all key elements of the outbreak control process have been considered and all potential interventions have been implemented and evaluated. Future development of the tool will include the addition of greater communication functionality in addition to automated analysis of data captured within the tool to help better understand the efficacy of interventions and facilitate rapid and effective dissemination, and archiving, of the outbreak management plans to relevant clinical staff and leaders. Whilst this initial pilot testing of the tool during an outbreak has demonstrated the basic usability of the tool, wider robust testing is required to evaluate the value and potential impact of the ICE on outbreak management processes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.