
Abstract
Previous evidence suggested a significant variation in the testing algorithms used across the United Kingdom for the diagnosis of Clostridium difficile infection (CDI) and new national guidelines were issued in 2012. The main aim of this paper was to explore if such variation in testing and reporting is still present, to compare the management of CDI cases, and to investigate if there is any significant variation in the antibiotic policies among different hospitals. Using London hospitals as a sample, results show that there is still a wide variation of testing methods and reporting used, making comparisons difficult. It is likely that the overall variability in practices would be greater at a national and, even more, at international level. The relationship between broad-spectrum antibiotics and C. difficile incidence and alternative approaches in antibiotic guidelines may require further studies.
Keywords
Introduction
Clostridium difficile infection (CDI) is still associated with considerable morbidity and mortality, with symptoms ranging from mild diarrhoea to toxic megacolon. Since 2007, the Department of Health in England and Wales has introduced mandatory reporting of all C. difficile toxin positive samples and hospital targets (Department of Health (DH) website, 2014), with monetary sanctions for failing hospitals. This has been associated with a reduction in the incidence of hospital cases in England (Public Health England, 2014) and similar reporting systems have been introduced in the rest of the United Kingdom. However, previous evidence (Goldenberg and French, 2011) suggested a significant variation in the testing algorithms used across the country, which has prevented an accurate comparison among hospitals. Using the London hospitals as a sample, the main aim of this paper was to investigate if such variation in testing and reporting is still present after the introduction of new Department of Health guidelines (DH website, 2012) and relevant literature on the topic (Planche et al, 2012). A secondary aim was also to compare the management of CDI cases and to explore if there is any significant variation in the antibiotic policies among different hospitals.
Methods
A questionnaire was sent out to all 25 London hospitals (also called NHS trusts). This was a pilot project (with the aim of a future national survey) and it referred to the year 2013, including requests for information on the following: testing algorithm used (with all possible combinations), criteria used for mandatory reporting, management of CDI with reference to isolation ward and multidisciplinary team review, and antimicrobial guidelines. Information on antimicrobial guidelines was focused on the choice of antibiotic for community/hospital acquired pneumonia (CAP and HAP) and urinary sepsis, restricted antibiotics and availability of modern technologies in the form of electronic prescribing and an antimicrobial mobile phone application.
Results
Twenty-four hospitals out of 25 responded to the survey, including seven major university teaching hospitals and 17 acute general hospitals.
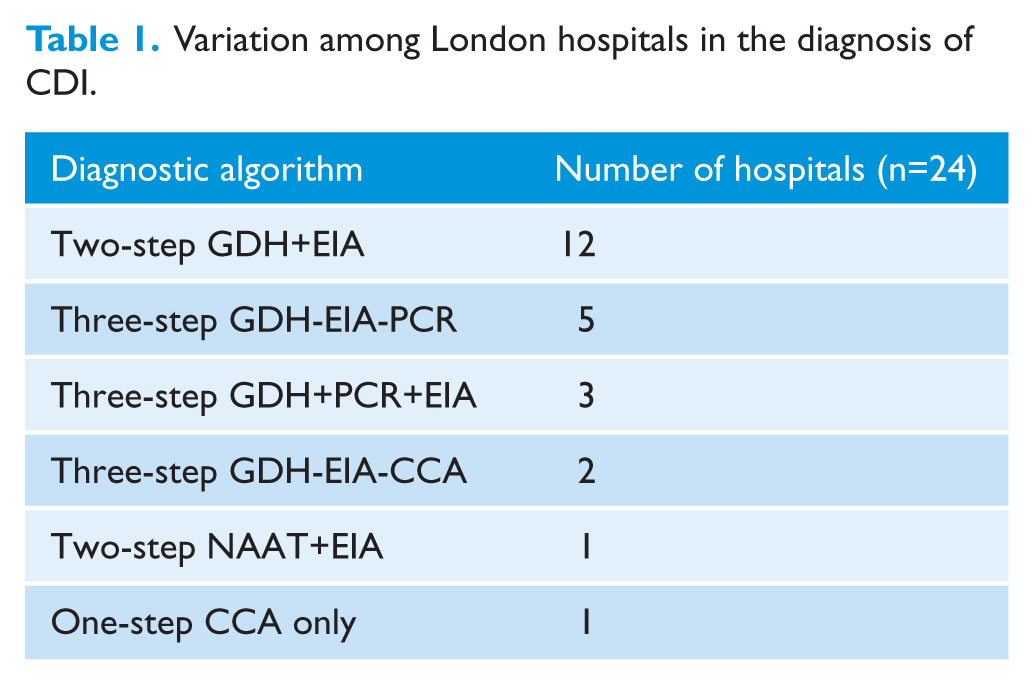
Testing algorithm: thirteen hospitals (52%) use a two-step algorithm for testing, 12 using Glutamate Dehydrogenase (GDH) followed by Enzyme Immunoassay (EIA) for C. difficile toxins A and B and one using Nucleic Acid Amplification Test (NAAT)-Polymerase Chain Reaction (PCR) for the toxin gene as a screening test, followed by EIA. Ten hospitals (40%) use a three-step algorithm: three using GDH-PCR-EIA, five using GDH-EIA-PCR and two using GDH-EIA-Cell cytotoxicity assay (CCA). One hospital reported using a one-stage procedure of only CCA without a screening test. Such variation is shown in Table 1.
Variation among London hospitals in the diagnosis of CDI.
Mandatory reporting: twenty one hospitals reported all positive toxin tests by EIA. Two hospitals reported positive toxin EIA results only where there was accompanying clinical evidence of CDI. The hospital using stand-alone CCA reported CCA positive results only when there was no alternative cause for the diarrhoea or the patient received treatment for presumed CDI. One hospital additionally reported all positive CCA results where the EIA was negative. There is no hospital reporting a positive PCR result in the absence of a corresponding EIA positive toxin result. No hospital is currently reporting the presence of pseudomembranous colitis on histopathology or colonoscopy.
CDI Management: two sites, both acute general hospital trusts, have a separate isolation ward for C. difficile patients. Sixteen hospitals have a weekly multidisciplinary team meeting (MDT) or ward round for patients with CDI of which five are teaching hospitals. Participants include a medical microbiologist and infection control nurse in all 16 hospitals, an antimicrobial pharmacist in 12 hospitals, a gastroenterologist in eight hospitals (one hospital has input only in severe cases) and the surgical team in one hospital for severe cases only. One hospital has a dietician input to the MDT and two hospitals have participation of ward managers/leaders.
Antimicrobial guidelines: nine of the 24 hospital trusts have their antimicrobial recommendations on the correct choice of antibiotics incorporated into a policy. Two university teaching hospitals have separate guidelines for elderly people over 75 years of age. In terms of restricted antibiotics, five hospitals (21%) restricted co-amoxiclav, 11 (46%) restricted piperacillin-tazobactam, 15 (62%) restricted clindamycin and fluoroquinolones, 19 (79%) restricted cephalosporins and 20 (83%) restricted carbapenems.
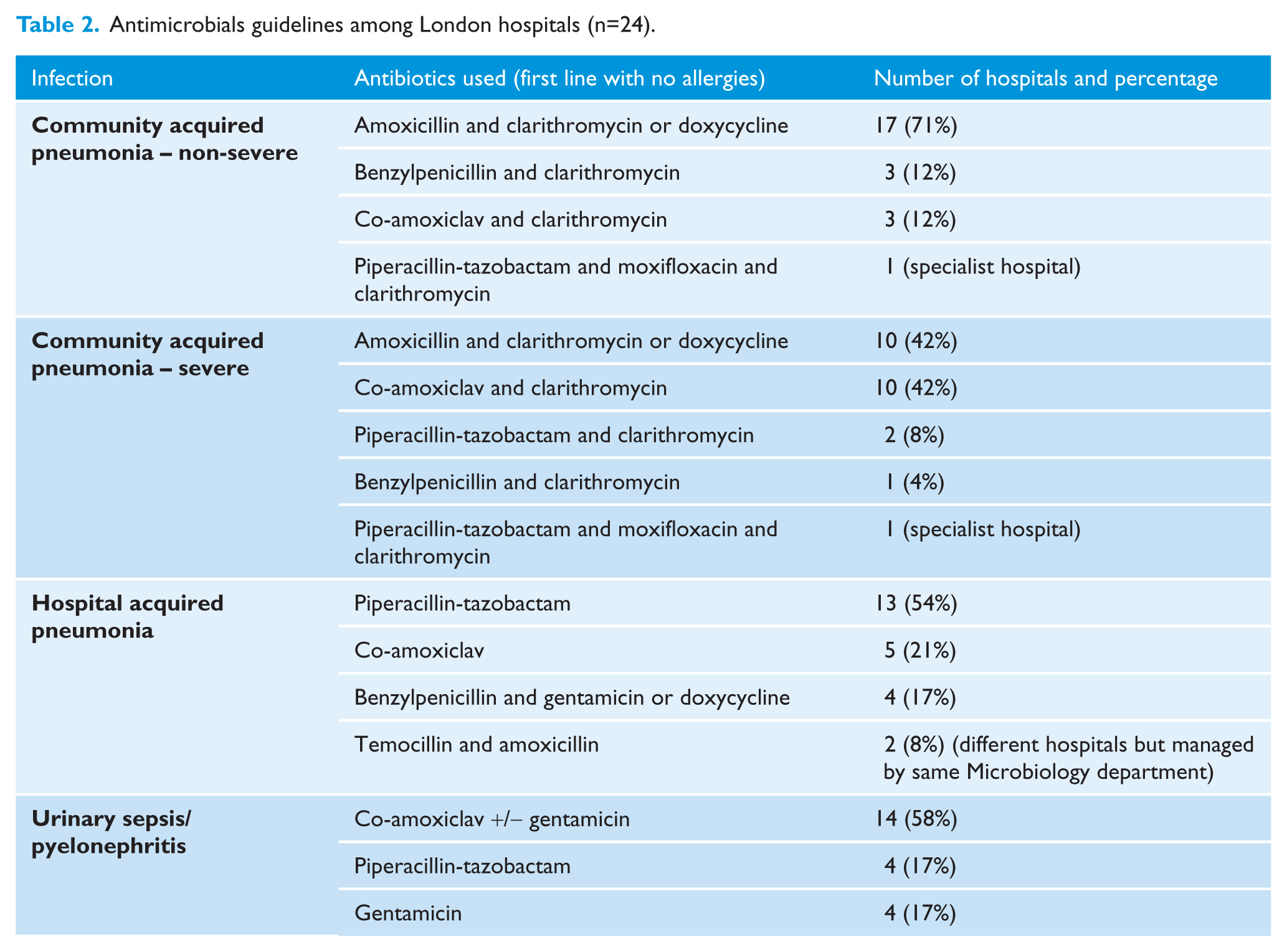
The variation in guidelines for CAP, HAP and urinary sepsis is shown in Table 2.
Antimicrobials guidelines among London hospitals (n=24).
Only six hospitals (25%) have an electronic prescribing system in place and eight hospitals (33%) have an antimicrobial guidelines application for mobile phones.
Discussion
A 2010 UK survey of 168 hospital trusts comprising 107 diagnostic laboratories showed that there were >25 different algorithms currently in use, preventing accurate comparison (Goldenberg and French, 2011). A recent validation study had calculated the sensitivity and specificity of all different tests and algorithms (Planche et al, 2012). Based on its findings, the Department of Health in March 2012 (DH website, 2012) issued updated guidance. This guidance recommended a two-stage testing algorithm for the diagnosis of CDI that consists of GDH (or a NAAT) followed by a sensitive toxin EIA (or a cytotoxin assay). It advises the mandatory reporting of all toxin positive samples as well as when there is the presence of pseudomembranous colitis on colonoscopy, histopathology or autopsy. However, as shown in our results, there is still some variability in testing and mandatory reporting of C. difficile two years on from this guidance. Hospitals using a CCA as a third step and reporting positive CCA results on negative EIA samples are possibly prone to report more cases of CDI. It is interesting that three hospital trusts are using a dual screening test (GDH and PCR together) and testing for EIA only on those samples that are positive by both tests. Although three hospitals used clinical criteria to decide which EIA positive samples to report last year, this is likely to be less of an issue from April 2014 with this way of reporting explicitly rejected in the 2014 update of DH guidelines (DH website, 2014). However, these new guidelines have allowed some flexibility in terms of unavoidable CDI cases as Clinical Commissioning Groups (CCGs – in England they hold 60% of the healthcare budget) can now opt to exclude these from any penalties, though this is at the discretion of individual CCGs. This may potentially introduce even more variability as different CCGs may accept or reject such option.
We did not find much variability in the management of the CDI cases. It is unclear how much a separate isolation ward contributes in addition to other infection control precautions, in reducing the incidence of CDI. The majority of hospitals within London do not have this facility. Current guidelines (Public Health England, 2014) suggest that CDI cases should be reviewed weekly, preferably by a multidisciplinary team, to ensure patients receive optimised care. Currently this happens in two thirds of hospitals within London. An infection control nurse, microbiologist and antimicrobial pharmacist appear to be the only disciplines that are consistent participants. Despite the importance of a gastroenterologist and dietician, their presence at MDT seems to be sporadical or incredibly rare, respectively.
Cephalosporins and clindamycin are the most frequently implicated antibiotics in CDI and the role of fluoroquinolones is less clear except for infections with 027 strains (Freeman et al, 2010). There is limited research into the relationship between amoxicillin-clavulanic acid or piperacillin-tazobactam and the incidence of CDI. Within NHS hospitals, there has been a significant increase in the use of these antibiotics and carbapenems: a 50% increase in co-amoxiclav usage, and a three-fold increase in piperacillin/tazobactam usage (Ashiru-Oredope et al, 2012). An interrupted time series restricting the use of co-amoxiclav and further restricting cephalosporin use showed a significant fall in CDI associated with the intervention; however this result cannot be attributed to restriction of co-amoxiclav alone (Fowler et al, 2007). From our results, mosthospitals within London have similar guidelines withsome difference probably due to the local epidemiology. The majority are restricting carbapenems, cephalosporins, fluoroquinolones and clindamycin, while there is little restriction of amoxicillin-clavulanic acid or piperacillin-tazobactam. Also, many hospitals have reached such a low rate of CDI cases that achieving a year on reduction in the number of cases is proving to be challenging as we may have finally touched the bottom line or steady state. We appreciate and support the importance of all infection control measures but we also raise the question whether we should re-think our antibiotic policies. It is interesting to note that two hospitals are using a combination of temocillin-amoxicillin for hospital-acquired pneumonia. One small study appeared to suggest that temocillin-amoxicillin is as effective as piperacillin-tazobactam while also inducing significantly fewer cases of CDI (Habayeb, ECCMID 2013, personal communication) in hospitals with a low incidence of Pseudomonas aeruginosa. However, further studies to corroborate these findings and to assess any adverse impact on patient morbidity and mortality would be useful. There is currently no data on the effectiveness of a separate antibiotic policy for elderly people to help reduce the incidence of CDI. Electronic prescribing was a great promise as a tool to reduce inappropriate antimicrobial consumption (Hitchen, 2007) but its cost and the time taken to implement it limit its availability in all hospitals. Finally, mobile phone applications may increase the compliance (Charani et al, 2013) of antimicrobial guidelines though they are expensive and not widely available.
New guidelines for the diagnosis and management of CDI are now in place but there is still a wide variation of testing methods and reporting used making comparisons difficult among London hospitals. With the limitations of this pilot survey, it is likely that the overall variability in practices would be greater at a national and, even more, at international level. The relationship between other broad-spectrum antibiotics and C. difficile incidence and alternative approaches in antibiotic guidelines may require further studies.
Footnotes
Acknowledgements
We thank all London hospitals for providing the data.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.