
Abstract
Background:
Ureteral fibroepithelial polyps (FEPs) are rare. The management of multiple polyps presents unique challenges, particularly when combined with other variants. These complex cases warrant individualized surgical planning.
Objective:
To characterize a distinct subset of complex ureteral FEPs defined by the triad of multiple annular stenosis, tortuous ureter, and multiple polyps—collectively termed “MASTUMP,” and to investigate its clinical, pathological, genetic features, and management considerations.
Design:
Single-center retrospective study.
Methods:
This study included nine patients treated for complex ureteral polyps between December 2019 and October 2024. Inclusion criteria required the presence of multiple FEPs (⩾3), ureteral tortuosity, and annular stenosis (⩾50% luminal narrowing). Clinical characteristics, imaging findings, surgical details, histopathology, and whole-exome sequencing (WES) were collected. Surgical outcomes and follow-up data were analyzed.
Results:
The cohort (77.7% male, mean age 35.1 ± 13.1 years) presented with bilateral (55.5%) or left-sided (44.4%) polyps, with a median lesion length of 4 (range 1–6) cm. All patients had a history of failed endoscopic or surgical management. According to the society of fetal urology grading system, hydronephrosis was classified as grade 1 in one case, grade 2 in three cases, grade 3 in four cases, and grade 4 in one case, with a mean anterior posterior diameter of 2.43 ± 0.88 cm. WES identified mutations in NRIP1 and TSC2 in two patients. Surgical management included segmental ureterectomy with reconstruction via ureteroureterostomy (two cases), pelvic flap (one case), lingual mucosal graft (one cases), and ileal ureter replacement (five cases). Over a median follow-up of 46.3 (range 11.5–75.4) months, no recurrences were observed.
Conclusion:
MASTUMP syndrome represents a clinical entity within complex ureteral polyps, potentially associated with congenital anomalies of the kidney and urinary tract. Endoscopic treatment carries a high risk of recurrence and should be approached with caution. Surgical resection with individualized reconstructive strategies offers durable outcomes. Further genetic studies and multicenter validation are essential to refine diagnostic criteria and treatment strategies.
Keywords
Introduction
Fibroepithelial polyps (FEPs) of the ureter, although the most common benign tumors of the ureter, remain rare. Unlike inflammatory polyps, FEPs are histologically characterized by normal-appearing urothelium overlying a fibrous stroma and do not regress after removal of chronic irritants such as stones or infections. 1 The etiology of ureteral polyps includes congenital anomalies, endocrine influences, and chronic mechanical or infectious irritation. 2 More than 80% of FEPs are solitary, with synchronous bilateral or multifocal presentations being exceptionally rare. 3 These polyps can cause significant ureteral obstruction, hematuria, and hydronephrosis, often mimicking urothelial carcinoma. 4
From a therapeutic perspective, the management of multiple polyps presents unique challenges in achieving complete excision while preserving ureteral function. 5 Ureteroscopic resection has emerged as the primary treatment modality due to its minimally invasive nature, particularly in cases where the disease is focal and the polyps are accessible. 2 However, more complex presentations involving diffuse polyposis, annular stenosis, or ureteral tortuosity complicate endoscopic treatment, increasing the risk of incomplete resection, recurrence, and subsequent renal dysfunction. 6 Current terminology inadequately distinguishes between patients with simple multifocal FEPs and those with a more severe triad of abnormalities. These complex cases warrant individualized surgical planning. 7
Our experience indicates that when multifocality, annular strictures, and ureteral tortuosity coexist, the disease behaves in a qualitatively different way—marked by recurrent obstruction, technically demanding surgery, and higher complication rates. Existing descriptors such as “multiple FEPs” do not fully capture this distinct clinical burden. To address this gap, we propose the descriptive term “MASTUMP,” representing Multiple Annular Stenosis, Tortuous Ureter, and Multiple Polyps. This nomenclature is not intended to redefine all multifocal FEPs but to provide a concise and clinically meaningful label for a reproducible constellation of abnormalities that is currently underrecognized.
In this study, we describe a series of rare and challenging MASTUMP cases, explore potential genetic underpinnings through whole-exome sequencing (WES), and evaluate optimal surgical strategies.
Methods
Patients
This retrospective, single-center case series included nine patients treated for complex ureteral polyps between December 2019 and October 2024. All cases met the following inclusion criteria: (1) presence of three features: (a) multiple annular stenoses (⩾2 segments) with ⩾50% luminal narrowing confirmed by retrograde or antegrade pyelography; (b) tortuous ureter with the presence of ⩾2 continuous angulations (>45°) observed on imaging or intraoperatively; (c) multiple polyps (⩾3 lesions) confirmed endoscopically or intraoperatively; and (2) histopathological confirmation of FEP. Exclusion criteria included inflammatory polyps, malignancy, concomitant urothelial carcinoma, inability to tolerate surgery, and incomplete follow-up. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental Material). 8
Data collection
Data were collected from Reconstruction of Urinary Tract: Technology, Epidemiology, and Results (RECUTTER) database. Clinical data included age, gender, BMI, comorbidities, symptoms, and previous treatment history. Laboratory assessments recorded serum creatinine and split renal function evaluated by renogram. Imaging evaluations utilized ultrasound, computed tomography urography (CTU), and magnetic resonance urography to quantify hydronephrosis severity, anteroposterior diameter (APD) of the hydronephrosis, renal parenchymal thickness, and polyp characteristics (number, size, location). The degree of hydronephrosis was assessed using the society of fetal urology (SFU) grading system. Surgical details documented the operative approach, reconstruction techniques, and intraoperative findings, such as polyp number, morphology, and distribution pattern; Pathological specimens underwent H&E staining.
Sequencing
DNA was isolated from peripheral blood samples obtained from the patients using Gentra Puregene Blood Kit (QIAGEN, Hilden, Germany). The SureSelect Human All Exon Kit (Agilent Technologies, Santa Clara, CA, USA) was used for whole exome capture. Target regions were sequenced on NovaSeq (Illumina, San Diego, CA, USA) and aligned to the GRCh37/hg19 human reference sequence. The mean coverage was >100X. Variants were annotated and filtered using TGex, with a particular focus on 54 established human congenital anomalies of the kidney and urinary tract (CAKUT)-associated genes and 131 genes implicated in monogenic multisystem syndromes that may present with facultative CAKUT manifestations. 9 The classification of variant pathogenicity is based on the American College of Medical Genetics (ACMG) guidelines.
Follow-up
Patients were followed every 3 months for the first year, then every 6 months thereafter. Symptoms, physical examination, serum creatinine, urine routine tests, and urinary ultrasound were performed at each visit. CTU and diuretic renograms were performed 3–6 months after the surgery. CTU. Recurrence was defined as the reappearance of polyps or stenosis on follow-up imaging or recurrence of clinical symptoms necessitating re-intervention.
Statistics
Statistical analyses were performed using SPSS 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were presented as mean ± standard deviation or median (interquartile range). Preoperative and postoperative comparisons were analyzed with paired t-tests. Statistical significance was defined as p < 0.05.
Results
A total of nine cases of complex ureteral polyps were included. Most were male (7/9, 77.7%). The mean age was 35.1 ± 13.1 years. Multiple polyps involved the left and bilateral sides in four and five cases, respectively. The polyps were numerous and mainly located in the proximal ureter, with a median size of 4 (range 1–6) cm long. All patients had failed previous treatments, including ureteroscopic electrotomy, thulium laser resection, polypectomy, or pyeloplasty. Hydronephrosis was graded according to the SFU system as follows: grade 1 in 1 case, grade 2 in 3 cases, grade 3 in 4 cases, and grade 4 in 1 case. The mean APD was 2.43 ± 0.88 cm, and mean renal parenchymal thickness was 1.41 ± 0.50 cm. Preoperative creatinine averaged 83.6 ± 14.2 µmol/L, with a mean affected-side renal function 44.2 ± 14.9 mL/min (Table 1).
Patients baseline characteristics.

Some patients have both flank pain and fever, or flank pain and hematuria.
Some patients have received several different treatments.
BMI, body mass index; PCN, percutaneous nephrostomy; SFU, society of fetal urology; URS, ureteroscopy.
Unlike simple polyps, all patients exhibited the triad of multiple annular stenosis, tortuous ureter, and multiple polyps (MASTUMP syndrome; Figure 1). Urography revealed a characteristic “lotus root” appearance of the ureter. WES identified NRIP1 and TSC2 mutations in two patients, who were more prone to full-length ureteral lesions.

The manifestation of the triad of multiple annular stenosis (a, b), tortuous ureter (c, d), and multiple polyps (e, f) observed by ureteroscopy and urography.
Surgical management included resection of the polyps, as well as the tortuous and annularly stenotic ureters in which the polyps had developed (Figure 2). Four patients underwent bilateral ileal ureter replacements due to long segment defects. One patient with bilateral disease underwent a left-sided lingual mucosal graft for a 2-cm lesion and robotic ileal ureter replacement on the right. For unilateral lesions, reconstructions included pelvic flap (5 cm), ureteroureterostomy (2 and 3 cm), and ileal ureter replacement (15 cm; Table 2). Pathological findings showed marked muscular hyperplasia with disordered arrangement and proliferation of intermuscular fibrous tissue.

Intraoperative and gross specimens’ appearance. (a, b) Annular stenosis of the ureter with multiple polyps; (c, d) ureteral strip and multifocal polyps; (e, f) thick ureteral wall with multiple strip-shaped polyps; (g, h) multiple annular stenosis of the ureter, from where multiple finger-shaped polyps grow out; red arrow = annular stenosis, yellow arrow = polyp.
Baseline data, polyps feature, surgical data, and follow-up of individual patient.
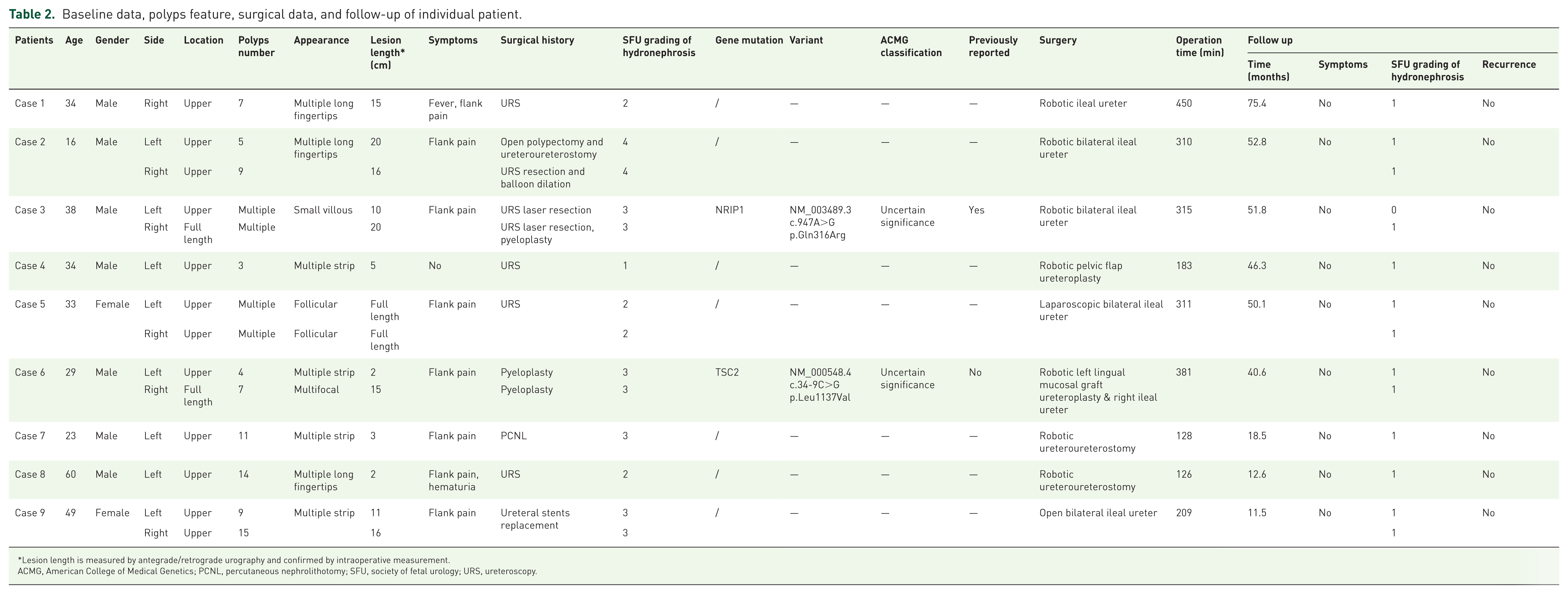
Lesion length is measured by antegrade/retrograde urography and confirmed by intraoperative measurement.
ACMG, American College of Medical Genetics; PCNL, percutaneous nephrolithotomy; SFU, society of fetal urology; URS, ureteroscopy.
One patient developed contralateral polyps and stones 2 years postsurgery. As he had already undergone contralateral ileal ureteral replacement, he was treated successfully with holmium laser lithotripsy and endoscopic polyp excision. At a median follow-up of 46.3 (range 11.5–75.4) months, no recurrences were observed. The mean APD improved to 1.43 ± 0.63 cm, and mean renal parenchymal thickness was 1.61 ± 0.42 cm. Postoperative creatinine was 84.0 ± 10.6 umol/L, and affected-side split renal function 48.7 ± 18.2 mL/min.
Discussion
Ureteral FEPs, although rare in adults, can cause significant clinical concern due to their ability to mimic malignancy and induce obstructive uropathy.4,10 With an incidence of 2% to 6%, most lesions are solitary and easily managed endoscopically.11,12 However, complex cases with multifocal or bilateral involvement present a therapeutic challenge. In adults, these complex lesions tend to be larger, more anatomically disruptive, and recurrent, differing from pediatric presentations. 13 These features complicate diagnostic accuracy and necessitate tailored therapeutic approaches to prevent life-threatening sequelae such as acute renal failure or malignant misdiagnosis. Endoscopic resection has been regarded as the gold standard for small lesions, whereas the optimal treatment for long lesions is still controversial. 14
This study introduces the descriptive concept of “MASTUMP syndrome,” defined by: (1) multiple annular stenosis with luminal narrowing ⩾50%, (2) tortuous ureter, and (3) multiple polyps. It should be noted that this criterion is primarily derived from clinical experience. Thresholds for ureteral tortuosity angle and annular stenosis were adapted from established cardiovascular criteria, 15 as these factors mainly influence endoscopic accessibility and procedural difficulty. While the cutoff of three polyps was selected to differentiate multifocal or diffuse ureteral involvement from focal lesions. We emphasize that MASTUMP is not intended to redefine all multifocal FEPs but to provide a concise framework for a specific subset in which this triad consistently coexists. This subset poses unique therapeutic challenges: while ureteroscopy is effective for simple lesions, tortuosity hampers endoscopic access, and annular strictures not only obstruct urine flow but also promote polyp recurrence.14,16 Notably, prior studies have associated annular stenosis with increased malignancy risk in upper tract urothelial carcinoma, further reinforcing the need for comprehensive resection. 17 Although polyps are benign tumors, we believe that annular stenosis should not be underestimated or misclassified.
Recognizing the MASTUMP pattern has important clinical implications for surgical decision-making. On preoperative imaging, diffuse defect with multifocal annular stenosis and marked ureteral tortuosity—particularly when producing a “lotus-root–like” appearance on retrograde or antegrade urography—should alert clinicians to the likelihood of MASTUMP rather than simple multifocal FEPs. In such patients, endoscopic interventions are often unsuccessful due to poor endoscopic access and high risk of recurrence. Therefore, when this triad is identified, early referral for definitive reconstructive surgery should be considered instead of repeated endoscopic attempts, as timely reconstruction may reduce iatrogenic injury, prevent treatment delays, and optimize functional outcomes.
Our surgical approach emphasized complete resection of polyps and diseased ureteral segments followed by reconstructive surgery. 18 The choice of reconstruction depended on defect length: short defects (<2 cm) benefited from direct anastomosis and flap repairs, while longer segments required intestinal substitution. Postoperative outcomes demonstrated good recovery without recurrence.
The etiology of FEPs remains unclear and is still debated. Various hypotheses have been proposed, including chronic irritation, infection, obstruction, trauma, and hormonal and developmental disturbances. 19 Our histological findings of smooth muscle hyperplasia and intermuscular fibrosis suggest a congenital or developmental basis rather than reactive changes. Moreover, WES identified NRIP1 and TSC2 variants in two patients. NRIP1 has been implicated in retinoic acid signaling and familial CAKUT,20–22 while TSC2 mutations, classically associated with tuberous sclerosis, could contribute to regulation of cell growth and proliferation via mTOR pathway. 23 These preliminary observations suggest that MASTUMP may represent a CAKUT-related phenotype, although causality cannot be established from such a limited dataset. Importantly, we caution against overinterpreting these findings: with only two mutation-positive patients among nine, genetic evidence remains suggestive rather than definitive. Larger studies comparing MASTUMP with solitary FEPs and other CAKUT phenotypes are required to clarify these associations.
Despite its novel insights, our study has limitations. First, the single-center retrospective design and small sample size limit generalizability. In particular, the identification of NRIP1 and TSC2 mutations in only two patients cannot establish a causal relationship, and the evidence for a genetic etiology should be interpreted with caution. This paucity of data may obscure the true prevalence of hereditary contributions, particularly given the known heterogeneity of CAKUT-related genes. 9 Second, the possibility of iatrogenic stenosis due to prior interventions cannot be completely excluded, and it is necessary to evaluate clinical conditions in untreated patients before fully establishing a new clinical entity in the future. Third, our diagnostic criteria for MASTUMP syndrome, although clinically intuitive, lack prospective validation and may be subject to interobserver variability. Future studies including cases with varying degrees of annular stenosis, ureteral tortuosity, and numbers of polyps are warranted to validate whether these criteria correspond to meaningful clinical or prognostic differences. These limitations underscore the need for prospective multicenter studies incorporating standardized criteria and genomic profiling to validate our findings.
In conclusion, MASTUMP syndrome is a newly proposed clinical entity characterized by multiple annular stenosis, tortuous ureters, and multiple polyps. A potential etiology may be genetic, as one form of CAKUT. Endoscopic treatment carries a high risk of recurrence and should be approached with caution. Instead, surgical resection with individualized reconstructive strategies offers durable outcomes. Further studies are warranted to validate diagnostic criteria and explore molecular underpinnings.
Supplemental Material
sj-pdf-1-tau-10.1177_17562872261422952 – Supplemental material for A clinical entity of multiple ureteral fibroepithelial polyps with annular stenosis and tortuosity: clinical features and management considerations
Supplemental material, sj-pdf-1-tau-10.1177_17562872261422952 for A clinical entity of multiple ureteral fibroepithelial polyps with annular stenosis and tortuosity: clinical features and management considerations by Xinfei Li, Xiaoteng Yu, Liqing Xu, Fangzhou Zhao, Honggang Ying, Zihao Tao, Xiang Wang, Lianghao Zhang, Zhihua Li, Kunlin Yang, Liqun Zhou, Gang Wang and Xuesong Li in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.