
Abstract
Background:
Traditionally performed as an inpatient procedure, day-case or ambulatory percutaneous nephrolithotomy (PCNL) has emerged in recent years as a promising alternative offering the potential to reduce hospital admissions and healthcare costs, without compromising patient outcomes.
Objectives:
Conduct a systematic review and meta-analysis to critically evaluate the efficacy, safety and overall outcomes of day-case PCNL
Design:
The systematic review was conducted in line with PRISMA guidelines (Preferred Reporting Items for Systematic reviews and Meta-Analyses).
Data sources and methods:
We conducted a comprehensive search of MEDLINE, Embase, Scopus, Web of Science, CENTRAL and Cochrane Databases from inception until January 2025 (CRD42024584357). The PICO statement for this systematic review is as follows: in patients with renal stones, what are the outcomes of day-case PCNL (intervention) compared with inpatient PCNL (comparator)? The authors included studies with more than 50 adult patients evaluating day-case PCNL (postoperative hospital stay ⩽ 24 h) written in the English language.
Results:
From an initial literature search of 2122 articles, 16 studies were identified, from which 3133 patients were included. A variety of standard, mini and ultra-mini techniques were used, with the majority opting for tubeless (61%) or totally tubeless PCNL (16%). The mean stone size was 21.5 ± 13.5 mm, with five studies including patients with renal structural abnormalities (3.6%). The pooled mean stone-free rate (SFR) was 90% (95% CI: 0.859–0.931), with a readmission rate of 3.2% (95% CI: 0.018–0.046). The overall complication rate was 10.7% (95% CI: 0.078–0.137), with most complications classified as minor with Clavien–Dindo Grade I–II (9.1%) and III–IV (1.6%). The quality assessment of the included literature revealed that all studies were of moderate to high quality.
Conclusion:
Day-case PCNL represents a safe and viable approach that has seen a growing adoption over recent years, driven in part by post-pandemic healthcare trends. Our review underscores its efficacy, marked by favourable outcomes and a low incidence of complications and readmissions. Moreover, detailed planning is paramount in order to establish clear criteria for potential surgical candidates and indications for inpatient admission, as well as a thorough follow-up plan.
Plain language summary
1. Aims and Purpose of the Research This study explored whether people who have a specific kidney stone surgery—called percutaneous nephrolithotomy (PCNL)—can safely go home the same day, rather than staying overnight in the hospital. This same-day approach is known as “day-case PCNL.” Before starting the research, we expected that with the right patient selection, same-day discharge could be safe and effective. Our aim was to combine data from existing studies to see how often the surgery was successful, how many patients needed to return to the hospital, and what kinds of side effects occurred. 2. Background of the Research This research matters because kidney stones are common, and PCNL is often used to treat large or complicated cases. Traditionally, patients are admitted to hospital after surgery, but hospitals are looking for ways to reduce inpatient stays and improve efficiency. If day-case PCNL is proven to be safe, it could benefit many patients by freeing up hospital beds, lowering healthcare costs, and allowing people to recover more comfortably at home. 3. Methods and Research Design We carried out a systematic review and meta-analysis, meaning we collected and analyzed data from multiple high-quality studies. We searched six medical databases and reviewed over 2,000 articles, ultimately including 16 studies with more than 3,100 adult patients who had day-case PCNL. We looked at how effective the procedure was, how often complications happened, and how many patients needed to return to the hospital after going home. 4. Results and Importance Our findings showed that about 90 percent of patients were successfully treated, just over 3 percent needed to return to the hospital, and around 10 percent experienced complications—most of which were mild and manageable. No deaths were reported. These results suggest that day-case PCNL is generally safe and effective for many patients, even some with more complex conditions.
Introduction
Since the pioneering work of Fernstorm and Jöhansson in 1976, 1 percutaneous nephrolithotomy (PCNL) has established itself as the gold standard for managing complex and large renal calculi, particularly those exceeding 2 cm in size.2–4
Traditionally performed as an inpatient procedure, day-case or ambulatory PCNL has emerged in recent years as a promising alternative offering the potential to reduce hospital admissions, lower healthcare costs, and enhance patient satisfaction. 5 This evolution has been driven in part by broader healthcare trends prioritizing shorter hospital stays, minimizing costs and improving convenience for patients. However, the paradigm shift towards performing PCNL as an outpatient procedure has also been facilitated by the advent of miniaturized instrumentation, improvements in lasers and nephrostomy-free surgical techniques.6–8
Individual studies have demonstrated the safety and efficacy of day-case PCNL, however, there remains a paucity of large-scale pooled data regarding its broader implementation and to delineate optimal patient selection criteria. 5 While recent meta-analyses by Calvillo-Ramirez et al. (day-case PCNL patients, n = 994) and Du et al. (day-case PCNL patients, n = 1956) have provided important insights into this approach, our study sought to evaluate a larger and more focused day-case cohort to better characterize outcomes in real-world practice.9,10
In addition, the heterogeneity in patient selection, surgical techniques and post-operative management across institutions further complicates the generalizability of existing data.
Thus, this systematic review and single-arm meta-analysis seeks to critically evaluate the efficacy, safety and overall outcomes of day-case PCNL. By synthesizing the available evidence, this review aims to elucidate the role of day-case PCNL within contemporary renal stone management and to identify potential areas for further investigation and clinical standardization.
Methods
Study design
This systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. 11 The review was registered prospectively with PROSPERO (CRD42024584357).
Search strategy
A comprehensive search of MEDLINE (via PubMed), Embase (via Ovid), Scopus, Web of Science, Cochrane Database of Systematic Reviews (CDSR) and Cochrane Central Register of Controlled Trials (CENTRAL) was conducted from the inception of each database until 15th January 2025. We also hand-searched the references of all review articles identified by our search strategy and screened unpublished ‘grey’ literature including conference abstracts.
Our search terms included (not limited to) ‘percutaneous nephrolithotomy’, ‘PCNL’, ‘day case’, ‘ambulatory’ and ‘outpatient’ and medical subject headings (MeSH) terms included ‘nephrolithotomy, percutaneous’ and ‘ambulatory surgical procedures’. The specific search strategy that we used is available in Supplemental Item 1.
Eligibility criteria
Inclusion criteria:
Studies where patients underwent day-case PCNL, defined as same-day discharge or within 24 h post-operatively.
Adult patients
Sample size of at least ⩾50 patients
Randomized controlled studies, cohort studies and case-control studies
English language
Exclusion criteria:
Studies where patients underwent inpatient PCNL that is, greater than 24 h admission post-operatively
Paediatric patients
Case reports, reviews and conference abstracts
Active urinary tract infection
Prior renal surgery
Retrograde intrarenal surgery (RIRS) and/or studies where patients underwent either PCNL or RIRS alone, and data pertaining to PCNL could not be individually identified
Abstracts were screened by two authors (SS and SL), with disagreements resolved by mutual agreement and discussion with senior author (BKS). Full-text screening was performed by the same authors, with conflicts handled using the same method. Title, abstract and full-text screening were conducted using Covidence systematic review software. In addition, the risk of bias for each included study was independently assessed by two authors (SS and SL) using the RoB-2 or the ROBINS-I tools, with results of this assessment included in Supplemental Item 2.12–14
Data extraction and outcome measures
For baseline characteristics, we extracted the following: patient demographics, incidence of comorbidities (hypertension and diabetes), incidence of pre-existing renal/urological conditions and pre-operative ASA classification. We also extracted operative characteristics detailing the technical aspects of the PCNL procedures undertaken in each study. Finally, several post-operative outcomes were extracted including stone-free rate (SFR), ED visit rate, readmission rate and complication rates. Data were initially extracted by one reviewer (SS) and subsequently independently validated by a second reviewer (SL). Any discrepancies identified during this validation process were resolved through discussion, with input from a third author (BKS) if consensus could not be reached.
Statistical analysis
Pooled means and proportions of our data were analysed using a random-effects, generic inverse variation method of DerSimonian and Laird, which assigns the weight of each study based on its variance. 15 The heterogeneity of effect size estimates across the studies was quantified using the Q statistic and I2 (p < 0.10 was considered significant) with a value of I2 of 0%–25% indicating insignificant statistical heterogeneity, 26%–50% low heterogeneity, and 51%–100% high heterogeneity. 16 When conducting this analysis, if the mean and standard deviation (SD) were unavailable, the median was converted to a mean using the recommended formulas illustrated in the Cochrane Handbook for Systematic Reviews of Interventions. 17 A leave-one-out sensitivity analysis was conducted by excluding studies in which means and standard deviations were estimated from medians and interquartile ranges, to test the robustness of the pooled effect estimates. Finally, data analysis was performed using Open Meta Analyst software (CEBM, Brown University, Providence, Rhode Island, USA).
Results
Study selection and patient characteristics
The initial literature search yielded 2122 potentially relevant articles. Following the removal of duplicates, abstract and full-text screening, sixteen unique studies involving 3471 patients were included in this systematic review and meta-analysis.6,18–32 PRISMA flowchart of the study selection process is depicted in Supplemental Item 3. From the studies selected, there were three randomized controlled trials (RCTs),6,19,26 three prospective cohort studies18,25,29 and ten retrospective cohort studies.20–25,27,28,30–32 It should be noted that of the 3471 patients, we have included only 3133 in our subsequent analysis; 338 patients across five studies3,6,19,26,28 did not meet our strict definition of day-case PCNL (i.e. planned/underwent same day discharge or discharge within 24 h post-operatively). Specifically, patients were excluded from Basiri et al. (planned 3-day admission cohort), and from Bechis et al., Kumar et al., Agrawal et al., and Roberts et al., where inpatient and outpatient data were reported separately but only day-case data met the inclusion criteria. This exclusion was necessary to preserve the integrity of pooled estimates for day-case procedures, although it may limit the generalizability of the findings to the broader PCNL populations. The baseline characteristics for all included studies are detailed in Table 1.
Basic characteristics of included studies.
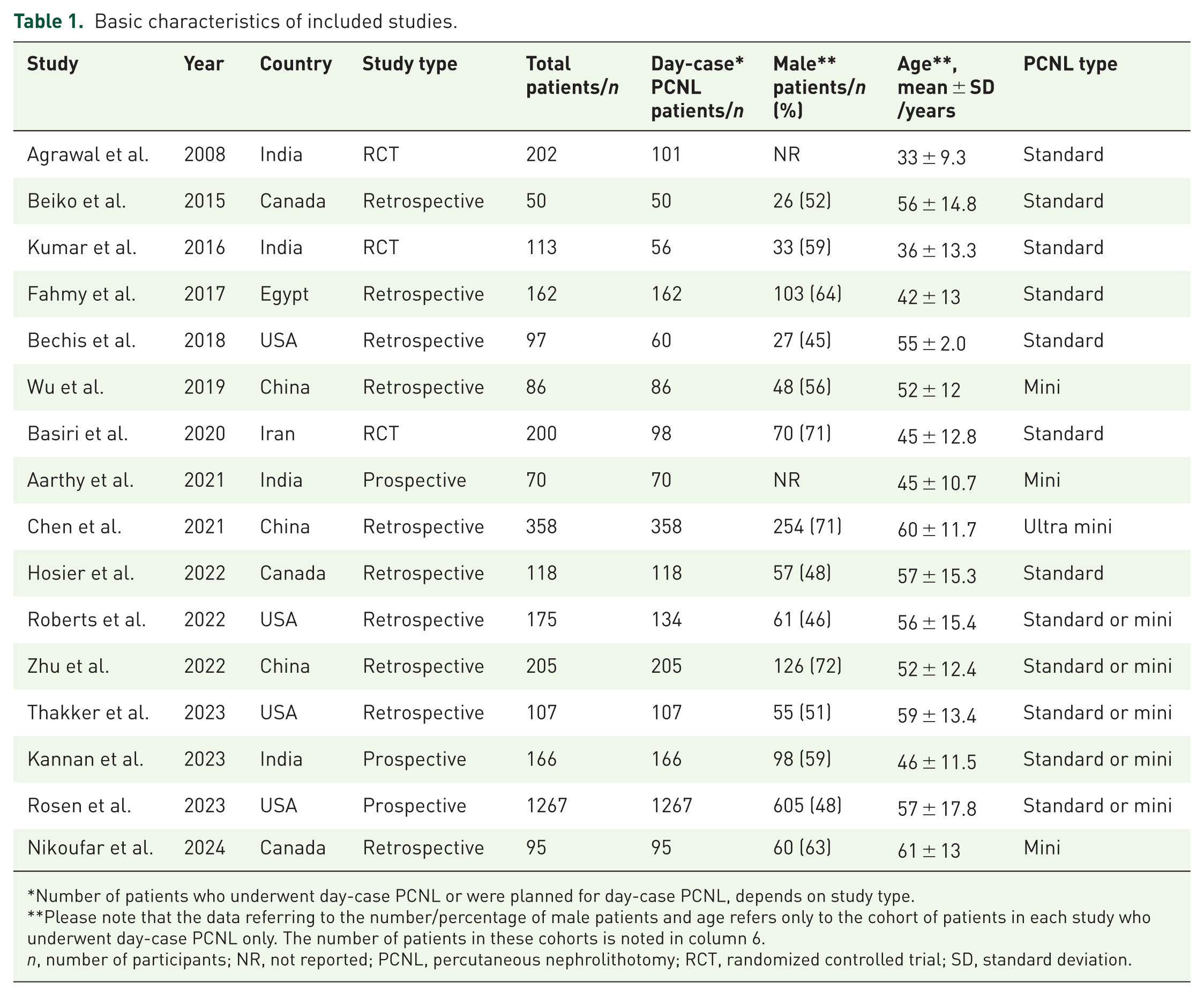
Number of patients who underwent day-case PCNL or were planned for day-case PCNL, depends on study type.
Please note that the data referring to the number/percentage of male patients and age refers only to the cohort of patients in each study who underwent day-case PCNL only. The number of patients in these cohorts is noted in column 6.
n, number of participants; NR, not reported; PCNL, percutaneous nephrolithotomy; RCT, randomized controlled trial; SD, standard deviation.
Assessment of risk of bias
The results of the quality assessment for all included studies are shown in Supplemental Item 2. Overall, all observational studies assessed using the ROBINS-I tool were assessed to be at moderate risk, with each study scoring as low or moderate risk across the various domains. Similarly, all randomized controlled trials assessed using the RoB-2 tool were determined to be of some concern, with most domains rated as low risk or some concern. Notably, Kumar et al. was considered high risk for bias arising from the randomization process, as the study mentioned randomization but lacked details on sequence generation and treatment allocation.
Clinical characteristics
The included studies recorded a range of baseline clinical characteristics as reported as pooled values in Table 2. Seven studies18,20,26–29,31 reported on rates of hypertension (48.0%) and diabetes (23.4%). In addition, five studies20,21,24,28,29 permitted patients with more significant comorbidities to undergo day-case PCNL, with 20.3% of patients in these studies classed ASA 3 or 4. From these five, three studies20,21,24 recorded a 3.6% incidence of renal structural abnormalities including horseshoe kidneys. Finally, nine studies18,20–24,29,31,32 included patients with partial or complete staghorn calculi to undergo day-case PCNL, accounting for 9.7% of their cumulative patient cohort.
Pooled clinical characteristics of included studies.

Notably, all data in this table refer only to patients who were planned for or underwent day-case PCNL in the selected studies. Total patients across all studies; n = 3471, only relevant day-case PCNL patients; n = 3133.
ASA, American Society of Anesthesiologists; N, total number of day-case PCNL participants across all studies; PCNL, percutaneous nephrolithotomy; SD, standard deviation.
Operative characteristics
Seven studies6,19–21,23,24,26 performed only standard or maxi-PCNL (sheath size 22–30Fr), three studies18,27,31 conducted only mini-PCNL (sheath size 14–20Fr) and Chen et al. performed ultra-mini-PCNL (sheath size 13Fr). The remaining five studies25,28–30,32 implemented a mixture of both standard and mini-PCNL procedures. Tubeless PCNL (ureteric stent insertion without concomitant nephrostomy insertion) was undertaken in the majority of studies, with three studies22,26,27 performing almost all cases with ‘totally tubeless’ technique (no stent or nephrostomy inserted). In addition, two papers utilized ECIRS (endoscopic combined intrarenal surgery), where ECIRS was the preferred modality.25,29 Finally, the mean stone size was 21.5 ± 13.5 mm with stones as large as 80 mm reported. 24 Other procedural details, including positioning, multi-tract PCNL incidence and mean operating room (OR) time, are noted in Table 3.
Operative characteristics of included studies.

Notably, all data in this table refer only to patients who were planned for or underwent day-case PCNL in the selected studies. Total patients across all studies; n = 3471, only relevant day-case PCNL patients; n = 3133.
These measurements refer to stone burden and are in mm2, rather than stone size in mm as reported by the other studies.
N, total number of day-case PCNL patients; NR, not reported; OR, operating room; PCN, percutaneous nephrostomy; PCNL, percutaneous nephrolithotomy; SD, standard deviation.
Post-operative outcomes
As illustrated in Table 4, studies implemented different protocols regarding same-day and overnight stay, resulting in varying discharge rates. Five studies19,21,24,27,28 successfully discharged all patients on the same day as the procedure, while the remaining studies discharged ⩾85% patients within 24 h post-procedure.
Post-operative outcomes of included studies.

Papers had varying definitions for stone-free rates with the majority of studies defining it as patients with residual stones <3 mm in size. See Supplemental Table 5 for further details.
CSC, complete stone clearance that is no residual fragments; ED, emergency department; NR, not reported.
As a measure of procedural success, the pooled SFR across fifteen studies was 90% (95% CI: 0.858–0.931, I2 = 93%, n = 2967) (Figure 1(a)) and for the seven studies6,18,20,25,27,28,31 that measured CSC (complete stone clearance that is no residual stones), the pooled CSC SFR was 83% (95% CI: 0.725–0.924), I2 = 97%, n = 657) (Figure 1(b)). Despite consistent reporting of SFR as a primary outcome, there was significant variation in SFR assessment methodology across studies, as shown in Supplemental Item 4. This variation observed in SFR modality and timing precluded further meaningful subgroup analysis.

(a) Pooled stone-free rate. (b) Pooled complete stone clearance rate.
Furthermore across fourteen studies, the pooled readmission rate was 3.2% (95% CI: 0.018–0.046, I² = 73%, n = 1700) (Figure 2(a)). The authors conducted further subgroup analysis assessing the impact of different PCNL types (standard/mini/ultra-mini). Studies conducting standard PCNL resulted in a pooled readmission rate of 3.9% (95% CI: 0.015–0.063, I2 = 70%, n = 645), mini-/ultra-mini-PCNL had a rate of 2.0% (95% CI: 0–0.042, I2 = 60%, n = 609) and studies employing both standard and mini-PCNL described a readmission rate of 5.1% (95% CI: 0–0.102, I2 = 87%, n = 446) as noted in Figure 2(b). Emergency department (ED) visit rates were also reported in seven studies, with an overall pooled rate of 12% (95% CI: 0.061–0.178, I2 = 88%, n = 726).

(a) Pooled readmission rate. (b) Subgroup analyses of standard, mini/ultra-mini and mixed cohorts for readmission rate.
Complications
The pooled overall complication rate across all studies was 10.7% (95% CI: 0.078–0.137, I2 = 88%, n = 3133) (Figure 3(a)). Further subgroup analysis was conducted to delineate differences in complication rates between PCNL types, as noted in Figure 3(b) with no significant difference identified. Fourteen studies further classified complications (n = 218) using the Clavien–Dindo classification with the majority being minor Grade I–II (85%) managed with conservative or medical treatment. The breakdown of complications by Clavien–Dindo grade is as follows: grade I 55%, grade II 30%, grade III 13% and grade IV 2%. The most common complication included post-operative fever and infection, accounting for 27% (n = 58), with twelve cases progressing to sepsis and requiring intravenous antibiotics. This was closely followed by mild to severe haematuria at 23% (n = 50), with six patients receiving blood transfusions and a further six requiring renal angioembolization for arterial pseudoaneurysm. Across all sixteen studies, there were a total of four grade IV complications. Hosier et al. reported one NSTEMI initially managed with medical management and subsequent coronary artery bypass grafting. Rosen et al. reported three unspecified grade IV complications without further details of these complications. No deaths were reported in any of the selected studies. Further detail regarding complications and management is summarized in Table 5. Finally, sensitivity analysis excluding studies with estimated means and SDs showed no substantial change in the pooled effect estimates or heterogeneity across SFR, readmission and complication rates.
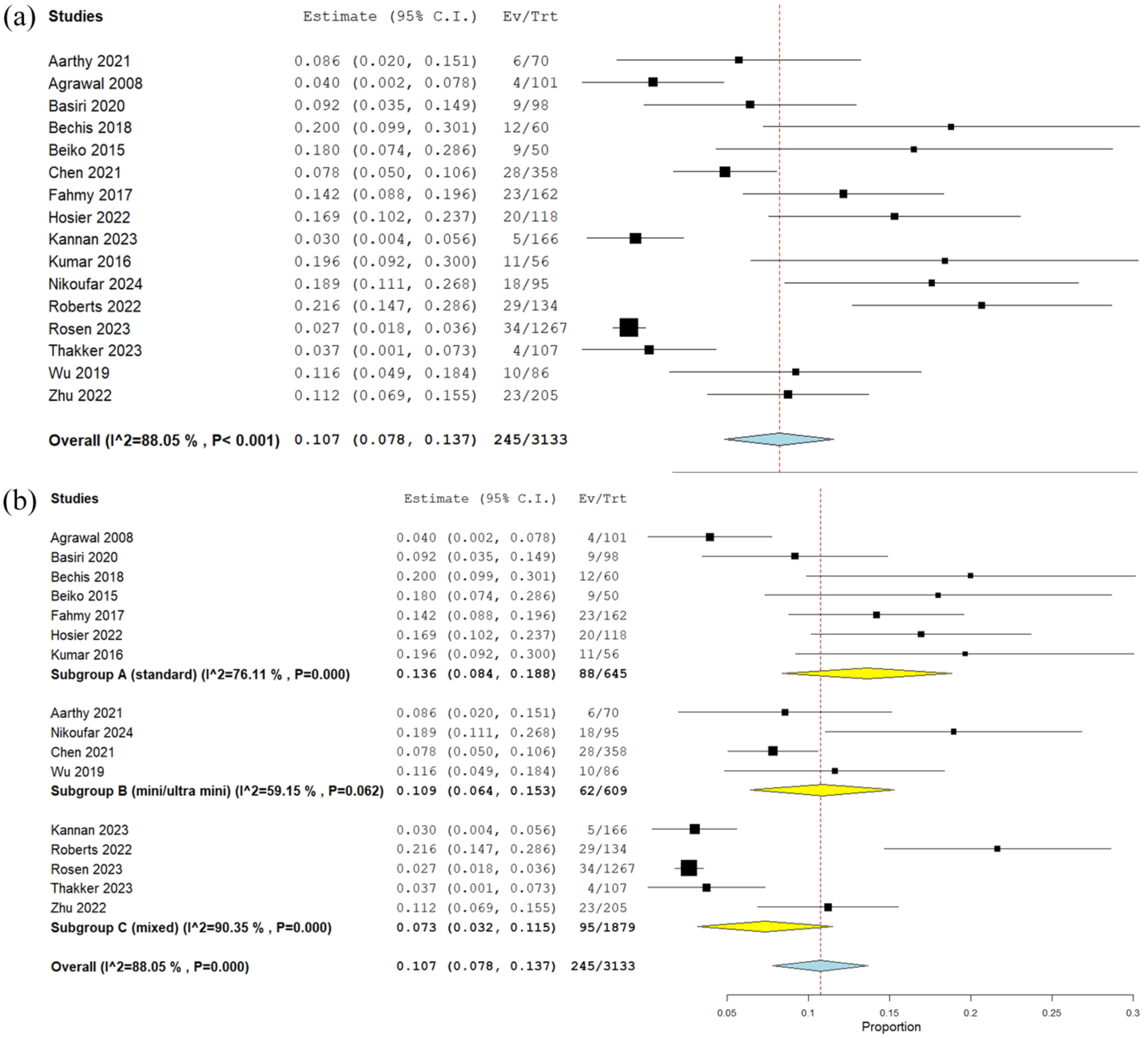
(a) Pooled complication rate. (b) Subgroup analyses of standard, mini/ultra-mini and mixed cohorts for complication rate.
Summary of all post-operative complications.

DVT, deep vein thrombosis; N, total number of day-case PCNL patients; NSTEM, non-ST-elevated myocardial infarction; PCNL, percutaneous nephrolithotomy; UTI, urinary tract infection.
Discussion
In the aftermath of the Covid-19 pandemic, the traditional inpatient model for PCNL has been increasingly challenged by the ascendency of ambulatory PCNL as institutions seek to maximize efficiency without compromising patient outcomes. To our knowledge, this study reports the largest pooled cohort of day-case PCNL patients (n = 3133), and successfully demonstrates that, with appropriate selection criteria, day-case PCNL is a safe and feasible strategy, yielding favourable outcomes and reduced healthcare burdens.
In line with recent studies, our analysis affirms the efficacy of day-case PCNL, evidenced by a pooled SFR of 90%. This aligns with rates reported in contemporary literature, such as Meng Gao et al., who reported similarly high success rates for day-case PCNL. 33 The consistency in these findings suggests that day-case PCNL achieves equivalent outcomes to traditional inpatient procedures, provided that patient selection and surgical techniques are carefully tailored.
The pooled readmission rate of 3.2% and complication rate of 10.7% also underscore the safety of day-case PCNL. Comparatively, Gassman et al. reported slightly higher readmission rates, likely attributable to differing patient populations and procedural characteristics. 34 Calvillo-Ramirez et al. also noted low complication rates in their analysis, further validating the safety of day-case PCNL in reducing post-operative morbidity. 9
Several studies18,22,29,32 documented reasons for failed day-case discharge. The most common causes were minor Clavien–Dindo grade I–II complications, such as pain, haematuria, fever, electrolyte disturbances, and hypotension. However, non-clinical barriers also emerged as significant factors. Zhu et al. reported that 23.3% of patients declined discharge despite meeting clinical criteria, primarily due to anxiety about potential post-operative complications. Moreover, Bechis et al. found that among the seventeen patients who were not discharged as planned, six remained for social reasons, such as inability to arrange transport or inadequate home support. These findings highlight the need for day-case units to screen for non-clinical barriers to discharge, including assessments of social support and discharge logistics – particularly when expanding pathways to more complex or vulnerable patient populations.
Patient selection remains a critical determinant of day-case PCNL success. Prior reviews, such as the study by Jones et al., have noted the importance of excluding patients with congenital anomalies, staghorn calculi, larger stone sizes and multiple morbidities. In addition, EAU 2024 guidelines emphasize selecting low-risk patients with ASA scores ⩽2, favourable stone and anatomical characteristics.2,5 The majority of included studies applied similar restrictions in order to achieve optimal outcomes with day-case PCNL. However, evidence from our review and external studies suggests that day-case PCNL can safely be performed in more complex patients.
Our post hoc analysis of nine studies18,20–24,29,31,32 that included staghorn stones (9.7% of the cohort) supports this, showing comparable SFRs and complication rates to those of less complex cases. Patients with staghorn calculi achieved a pooled SFR of 90% (95% CI: 0.879–0.934, I2 = 75%, n = 2376), which aligns closely with the overall pooled stone-free rate reported in this review. In addition, this value compares favourably with the 84.8% SFR reported by Zhu et al. 35 in their study of multi-tract day-case PCNL for the treatment of complex renal stones. Of the included studies, Rosen et al. included the highest number of patients with staghorn calculi (n = 79) and routinely pre-treated these patients up to a week prior with oral antibiotics before ambulatory surgery. In addition, they noted that staghorn calculi were more likely to require transfer to the hospital and require a second-look post-operatively. In addition, Bechis et al. and Beiko et al. successfully demonstrated the feasibility of day-case PCNL in multiple patients (n = 23) with renal structural abnormalities including horseshoe kidneys.20,21 These findings cautiously suggest that with experienced surgical teams, careful preoperative planning and standardized protocols, day-case PCNL could be safely extended to more complex patient populations, challenging the traditional boundaries of its use.
There was notable heterogeneity in the surgical techniques employed across the sixteen studies. Miniaturized techniques – particularly mini- and ultra-mini-PCNL – have been reported in the literature to be associated with reduced renal trauma, lower postoperative pain and shorter hospital stays due to smaller tract dilation. 36 However, this review observed no differences in readmission or complication rates between studies utilizing miniaturized and standard techniques. This is consistent with findings from Calvillo-Ramirez et al., who reported no significant differences in complication or transfusion rates between standard and mini-PCNL cohorts. In terms of drainage technique, most patients (n = 1971) underwent tubeless PCNL, and three studies employed totally tubeless approaches. Kumer et al. noted the benefits of tubeless PCNL, including reduced analgesic requirement, blood loss and faster return to normal activity. However, broader conclusions regarding the drainage technique or tract size remain limited by substantial heterogeneity in stone burden, patient comorbidities, perioperative protocols and inconsistent stratification of these variables across studies. Finally, Kannan et al. compared supine and prone positioning directly with no clear superiority identified, although prone positioning appears to be preferential in patients with complex anatomy or larger stone burden.
The economic advantages of day-case PCNL are significant. Thakker et al. highlighted the comparative cost-effectiveness of day-case PCNL, reporting lower overall expenditures when compared with inpatient procedures. In particular, they noted that day-case PCNL translated to advantageous operating margins through decreased bed occupancy and shorter post-operative monitoring periods. 30 These findings are consistent with the contemporary literature – as Kroczak et al. report, outpatient PCNL substantially reduces healthcare costs by minimizing inpatient bed occupancy and shortening post-operative monitoring. 37 However, it is important to acknowledge that not all institutions have the infrastructure, staffing or perioperative pathways required to safely support ambulatory surgery. Furthermore, while day-case PCNL is assumed to offer improved patient convenience and satisfaction due to earlier discharge and home recovery, these assumptions remain largely unverified – none of the studies in this review assessed patient-reported outcomes, such as quality of life or patient satisfaction. Echoed by a recent meta-analysis by Du et al., this lack of data on quality-of-life outcomes and patient satisfaction represents a significant gap in the literature. Future research should prioritize evaluating the impact of day-case PCNL on patient-reported outcomes to ensure a more comprehensive understanding of its benefits.
Despite this review representing the largest pooled cohort of day-case PCNL patients, several limitations must be acknowledged. First, the heterogeneity in surgical techniques (e.g., standard, mini-, and ultra-mini-PCNL), drainage techniques and patient positioning across studies introduces variability that complicates direct comparison of outcomes. To make more robust conclusions regarding surgical technique, further studies that directly compare these approaches in the day-case setting are needed.
Second, inconsistent definitions of outcomes, particularly SFR, limit the generalizability of our conclusions. The authors observed significant heterogeneity in the assessment and definition of SFR as recorded in Supplemental Item 4. Two studies assessed SFR endoscopically intra-operatively, with the remainder using post-operative X-ray, CT or ultrasound days, weeks or months following the procedure. In addition, definitions for SFR varied significantly, with papers defining SFR as the absence of residual fragments < 2, <3, <4 and < 5mm, respectively, as well as six studies that reported CSC. This heterogeneity undermines comparability and underscores the need for standardized outcome definitions across institutions. Similarly, ED visit rates were inconsistently reported across the studies, with only seven studies commenting on this outcome – further underscoring the need for uniform outcome reporting following PCNL.
Additionally, the predominance of retrospective cohort studies in our analysis also raises the potential for selection and reporting bias. Only three randomized controlled trials were included, highlighting the need for more prospective, high-quality evidence. Moreover, few studies addressed long-term outcomes, such as stone recurrence rates or functional renal recovery, limiting the ability to assess the durability of day-case PCNL outcomes.
Finally, from a methodological standpoint, although study screening was conducted independently by two reviewers with consensus and senior author adjudication for disagreements, a limitation is that inter-rater reliability was not formally quantified.
Finally, future research should address key gaps in the literature, particularly focusing on complex patient populations and underexplored outcomes. While this review demonstrates the feasibility of day-case PCNL in selected patients with staghorn calculi, further multi-centre, randomized controlled trials are necessary to standardize protocols and identify optimal patient selection criteria for these groups. In addition, future studies should evaluate long-term outcomes, such as recurrence rates and renal function preservation, to ensure that the safety and efficacy observed in the immediate post-operative period in complex stone patients are sustained over time. Moreover, studies such as Thakker et al. have emphasized the cost-saving potential of day-case PCNL – however, further granular financial analyses are needed to quantify savings across diverse healthcare systems, including comparisons of direct and indirect costs. Finally, none of the studies in this review explicitly evaluated patient-reported outcomes or quality of life. Given the increasing emphasis on patient-centred care, future research should prioritize these measures to better understand the broader benefits of day-case PCNL. Assessing post-operative pain, functional recovery and patient satisfaction will be critical to fully establishing day-case PCNL as a standard of care.
Conclusion
Day-case PCNL represents a safe and increasingly viable approach, with growing adoption in recent years, driven in part due to broader post-pandemic healthcare trends. Our comprehensive review underscores its efficacy, favourable outcomes and a low incidence of complications and readmissions. Rigorous pre-operative planning remains essential in establishing criteria for suitable surgical candidates; however, increasing evidence indicates the opportunity for extended patient criteria, including patients with renal abnormalities and complex stone burdens. Future research should standardize protocols and explore long-term quality-of-life analyses.
Supplemental Material
sj-docx-1-tau-10.1177_17562872251389084 – Supplemental material for Insights and outcomes of day-case percutaneous nephrolithotomy: results of a systematic review and single-arm meta-analysis
Supplemental material, sj-docx-1-tau-10.1177_17562872251389084 for Insights and outcomes of day-case percutaneous nephrolithotomy: results of a systematic review and single-arm meta-analysis by Shreehari Suresh, Sylvia Ling, Dilip K. Vankayalapati, Sherwin M. Ganegoda and Bhaskar Somani in Therapeutic Advances in Urology
Supplemental Material
sj-docx-2-tau-10.1177_17562872251389084 – Supplemental material for Insights and outcomes of day-case percutaneous nephrolithotomy: results of a systematic review and single-arm meta-analysis
Supplemental material, sj-docx-2-tau-10.1177_17562872251389084 for Insights and outcomes of day-case percutaneous nephrolithotomy: results of a systematic review and single-arm meta-analysis by Shreehari Suresh, Sylvia Ling, Dilip K. Vankayalapati, Sherwin M. Ganegoda and Bhaskar Somani in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.