
Abstract
Background:
Next-generation imaging (NGI) technologies such as multiparametric magnetic resonance imaging (mpMRI) and total-body NGI (tbNGI) methodologies including choline, fluciclovine or PSMA positron emission tomography/computed tomography (PET/CT), whole-body MRI (wbMRI), and PET/MRI are becoming increasingly available, but their use in different prostate cancer (PCa) settings is under debate. The Gruppo Uro-Oncologico del Nord-Est (GUONE) designed a survey to explore the current clinical practice of NGI utilization in a specific macro-region in North-Eastern Italy.
Methods:
A cross-sectional survey was conducted by administering an anonymous online multiple-choice questionnaire to uro-oncologists practicing in North-Eastern Italy, using the Google Forms® platform. The use of NGI was investigated in the following settings: primary staging of PCa; management of biochemical (BCR) and local recurrence (LR); re-staging in metastatic hormone-sensitive PCa (mHSPC), metastatic castration-resistant PCa (mCRPC), non-metastatic CRPC (nmCRPC), and oligometastatic PCa (OMPC).
Results:
In all, 100 uro-oncologists accessed and completed the survey. In primary N/M staging, the use of tbNGI increases in accordance with NCCN risk groups. Re-staging with choline and PSMA PET/CT is the prevalent choice in the case of BCR after radical prostatectomy. Moreover, when the PSA value rises, there is a parallel increased use of tbNGI. When an LR is suspected, PSMA PET/CT plus mpMRI is the most selected option. Re-staging with tbNGI (PSMA PET/CT) is preferred in mHSPC, mCRPC, and nmCRPC patients in case of progression of disease. Overall, there is a limited use of wbMRI and PET/MRI in all the settings investigated.
Conclusion:
Our survey describes the expanding role of NGI modalities in the management of PCa patients, from primary staging and re-staging to management of advanced PCa and assessment of treatment response. Several controversial issues have emerged, which need to be addressed in prospective studies to develop a standardized and cost-effective NGI utilization.
Background
Nowadays, prostate cancer (PCa) therapy is increasingly related to its clinical sub-settings, especially oligometastatic disease. Thus, it is crucial to accurately define the extent of metastatic burden, to correctly address effective therapeutic strategies, including chemotherapy, new androgen receptor pathway inhibitors (ARPis), radiometabolic approaches (177Lu-Prostate Specific Membrane Antigen [PSMA] and Radium–223) as well as metastasis-directed therapy (MDT).1,2
The phrase “next-generation imaging” (NGI) is generally employed in the PCa setting to refer to technologies such as multiparametric magnetic resonance imaging (mpMRI) as well as total body diagnostic methodologies (which go under the term total-body NGI, tbNGI) such as positron emission tomography/computed tomography (PET/CT) with PCa dedicated radiotracers (including [18F]/[11C]-choline, [18F]-fluciclovine and [68Ga]/[18F-] PSMA-ligands), whole-body MRI (wbMRI) and hybrid imaging techniques such as PET/MRI.
In the last few years, the diffusion of NGI technologies has brought a revolution in the diagnostic and therapeutic management of PCa and has provided clinicians with several diagnostic options.
Due to the lack of guidelines or clear recommendations derived from clinical data comparing NGI technologies with conventional imaging modalities (CIM), to date, their use in the different PCa settings remains widely debated. 3
Therefore, there is currently a significant level of heterogeneity in their use. Furthermore, the under- or over-utilization of such techniques may jeopardize oncological outcomes and impact waiting lists as well as healthcare costs.
The present survey was conducted by the Gruppo Uro-Oncologico del Nord-Est (GUONE) to collect the opinion of uro-oncologists and to describe the current clinical practice in a specific macro-region in North-Eastern Italy.
Methods
On May 1st, 2023, a cross-sectional survey was conducted using the cloud-based platform Google Forms® by administering an anonymous online questionnaire consisting of thirty multiple-choice questions to uro-oncologists (radiation oncologists, medical oncologists, and urologists) practicing in North-Eastern Italy and members of the genito-urinary tumor board at their respective Institution.
Topics of interest included radiologic investigations conducted in the primary staging of PCa, management of biochemical (BCR) and local recurrence (LR), re-staging in metastatic hormone-sensitive PCa (mHSPC), metastatic castration-resistant PCa (mCRPC), non-metastatic CRPC (nmCRPC), and oligometastatic PCa (OMPC).
All participants were invited to complete anonymously the electronic form within 60 days of the invitation. A reminder was sent after 30 days.
This survey did not require the approval of a referring Ethical Committee as there was no direct patient involvement.
The survey was anonymous and participation was voluntary. No one, including the researcher, could connect a respondent to his/her answer. Participants could choose not to participate in the survey, stop responding at any time, or skip questions. Therefore, in accordance with the European Union General Data Protection Regulation (GDPR) 2016/679, no informed consent or Ethical Committee approval was required.
Answers were reported as absolute numbers and percentages with a 95% confidence interval (CI) according to the Clopper–Pearson method. Differences across in answer distribution according to strata were evaluated through Fisher’s exact test.
Results
Overall, 100 uro-oncologists accessed the survey and completed all sections with a 100% response rate for each item (Table 1). A total of 41%, 32%, and 27% of responders were urologists, medical oncologists, and radiation oncologists, respectively. Sixty percent of responders have been specialists for more than 10 years (Table 1).
Sociodemographic characteristics of survey participants.

mp-MRI, multiparametric magnetic resonance imaging; NGI, next-generation imaging; PET/CT, positron emission tomography/computed tomography; PET/MRI, positron emission tomography/magnetic resonance imaging.
The majority of participants reported to practice in the Veneto region (49%) and community hospitals (49%) (Table 1). Sixty-six percent of participants declared to devote more than half of their working time to uro-oncology. NGI technologies are available at the Institutions of the survey participants in a range from 16% (PET/MRI) to 88% (mpMRI) (Table 1).
Figure 1 depicts the distribution of NGI technologies by the Local Health Unit in the macro-region addressed by the survey.

Distribution of NGI technologies by Local Health Unit in North-Eastern Italy.
Twenty-two percent, 29%, 22%, 11%, and 8% of participants have one up to five NGI technologies available at their Institutions, respectively; only 8% do not have any NGI method (Table 1).
The results of the survey are grouped by topic and they are summarized in the following sections.
Topic 1: Primary staging of PCa
The use of mpMRI for local staging (T-staging) is reported by half of the survey participants with no difference between risk groups: 52%, 57%, and 47% in the favorable-intermediate (FIR), unfavorable-intermediate (UIR), and high/very-high risk (HR/VHR) group, respectively (Supplemental Material Questionnaire, Q 2.1—2.0).
In the staging of regional and distant disease (N/M staging), the use of tbNGI technologies increases considerably in accordance with risk groups: 14% in the FIR, 42% in UIR, and 85% in the HR/VHR group (p < 0.01; Q 2.1–2.3, Table 2). Only in the HR/VHR group, the use of tbNGI is prevalent as compared to CIM (85% vs 14%, Table 2). In the FIR group, 29% of survey participants ordered no staging investigation for regional and distant disease, whereas in the UIR and HR/VHR groups, only 3% and 1%, respectively, did not order any investigation (Table 2).
Imaging technique utilization for staging purposes according to the patient’s NCCN risk group.
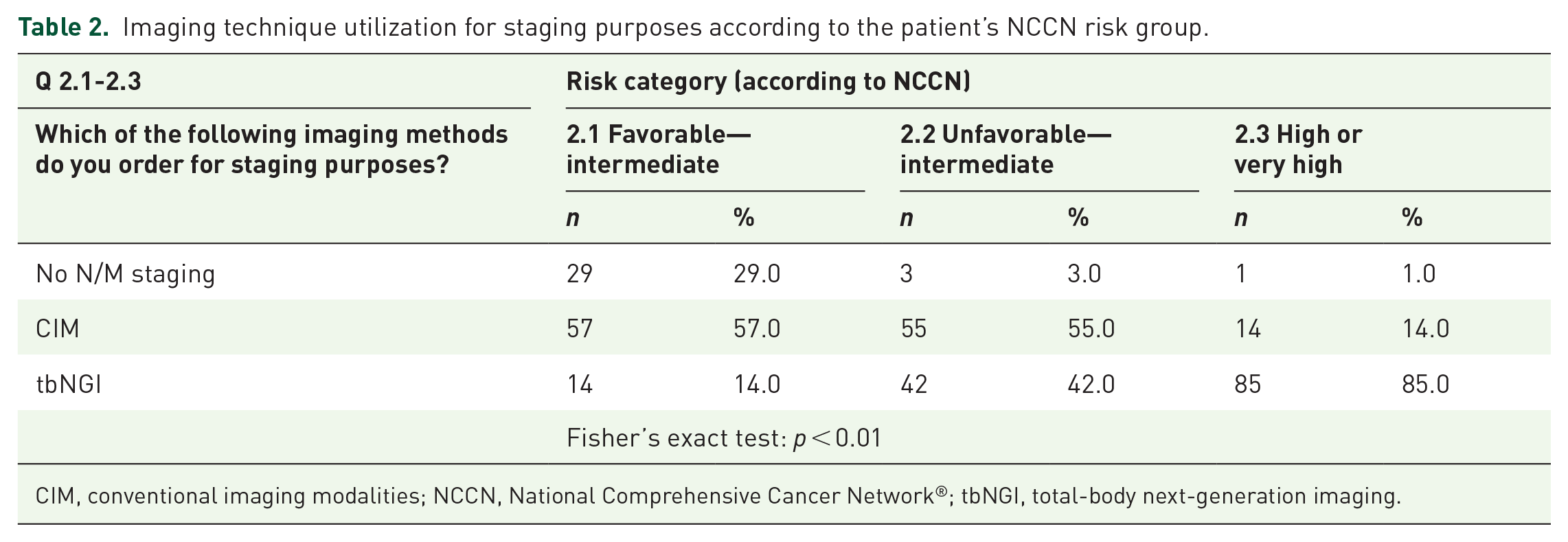
CIM, conventional imaging modalities; NCCN, National Comprehensive Cancer Network®; tbNGI, total-body next-generation imaging.
Among the tbNGI modalities, choline PET/CT (57%, 53%, and 52% in FIR, UIR, and HR/VHR groups, respectively) and PSMA PET (29%, 39%, and 40% in FIR, UIR, and HR/VHR group, respectively) are the prevalent choices between participants for N/M staging. The use of wbMRI or PET/MRI was inferior to 5% in all risk groups. No use of fluciclovine PET/CT was reported (Supplemental Material Questionnaire, Q 2.1–2.3).
Medical specialty and the number of years of professional practice of the responders did not significantly affect the choice between the two staging methods (CIM vs NGI) for each risk category.
More frequent reasons for ordering a tbNGI investigation at primary N/M staging are as follows: inconclusive CIM, HR/VHR group, and elevated PSA value at diagnosis (Q 2.4, Table 3).
Attitude to the use of tbNGI for staging and re-staging in different patterns of disease.

BPFS, biochemical progression-free survival; CIM, conventional imaging modalities; ISUP, International Society of Urological Pathology; mCRPC, metastatic castration-resistant prostate cancer; mHSPC, metastatic hormone-sensitive; PSA, prostate-specific antigen; PSAdt, prostate-specific antigen doubling time; RT, radiotherapy; tbNGI, total-body next-generation imaging.
Topic 2: Management of BCR and LR
For 80% of responders re-staging is not appropriate after primary therapy (surgery or radiotherapy) in the presence of biochemically controlled disease (Supplemental Material Questionnaire, Q 3.1). In the case of BCR following primary therapy and/or suspected LR, 47% of survey participants ordered a tbNGI investigation associated with local mpMRI, whereas 40% ordered a tbNGI only and 10% a mpMRI only (Supplemental Material Questionnaire, Q 3.2). In this setting, PSMA PET/CT (80%) and choline PET (41%) were the most largely ordered tbNGI investigations by the survey responders. Only 3% of responders requested a PET/MRI; none requested a wbMRI or fluciclovine PET/CT (Supplemental Material Questionnaire, Q 3.2).
In these scenarios, radiation oncologists, more frequently than medical oncologists and urologists, request tbNGI combined with mpMRI (p = 0.03).
In the case of NGI suspicious for LR, 62% of survey responders require a biopsy confirmation in selected cases only, 35% do not require any biopsy, and 3% ordered a biopsy confirmation in all cases, respectively (Supplemental Material Questionnaire, Q 3.3).
Re-staging with tbNGI is the prevalent choice in patients candidate to salvage radiotherapy for BCR after radical prostatectomy, for any PSA range considered (0.2–0.5, 0.5–1, 1–2, ⩾2 ng/ml). Moreover, as the PSA value rises, there is a concomitant increased use of re-staging tbNGI investigations (Q 3.4–3.7, Table 4; p < 0.01).
Re-staging investigations in patients candidate to salvage radiotherapy for BCR after radical prostatectomy according to PSA level.
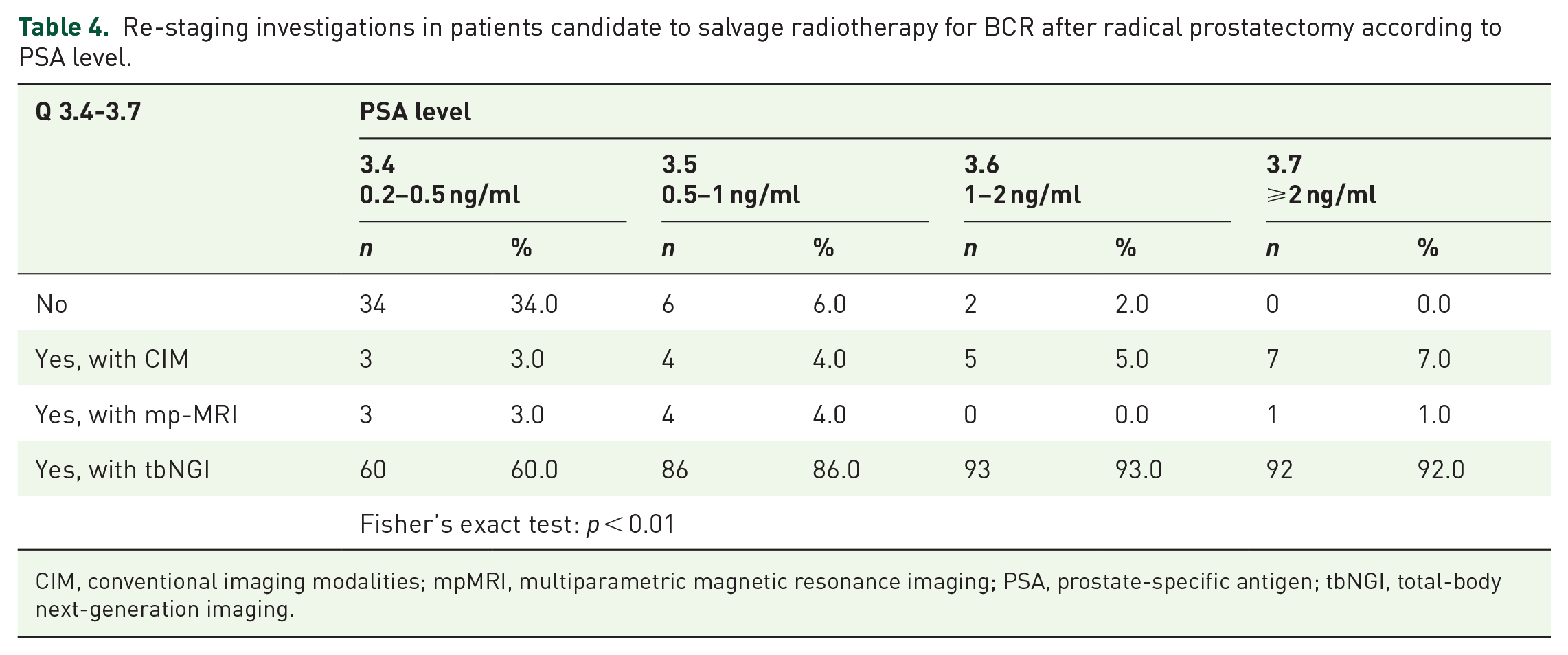
CIM, conventional imaging modalities; mpMRI, multiparametric magnetic resonance imaging; PSA, prostate-specific antigen; tbNGI, total-body next-generation imaging.
When PSA ranges between 0.2 and 0.5 ng/ml, 34% of survey participants do not re-stage patients (Table 4).
Among the tbNGI modalities, choline PET/CT and PSMA PET/CT are the most selected choices for each PSA range considered. In particular, PSMA PET/CT is the prevalent option for PSA range 0.2–0.5 ng/ml (87%), 0.5–1 ng/ml (84%), and 1–2 ng/ml (66%). Only for the PSA range ⩾2 ng/ml, the greatest percentage of participants opted for choline PET/CT (67%) (Supplemental Material Questionnaire, Q3.4–3.7). For each PSA range, the use of wbMRI or PET/MRI was <5%. None of the responders employed fluciclovine PET/CT (Supplemental Material Questionnaire, Q 3.4–3.7). In the case of BCR following radical prostatectomy in patients candidate to salvage RT, the most relevant factors associated with the request of tbNGI before RT are evidence of pN+ disease at histological examination (78%) and PSA doubling time (PSA DT) <6 months (64%) (Q 3.8, Table 3).
Topic 3. Re-staging in mHSPC
In the mHSPC setting, more than half of the interviewees (54%) would demand a tbNGI re-staging in case of biochemical progression only when systemic therapy is ongoing, as well as in patients with both biochemical and clinical progression (56%) (Q 4.1, Q 4.3, Table 5). In both scenarios, smaller percentages of participants chose CIM or the modality used previously.
Attitude to investigation utilization for re-staging purposes according to clinical setting.

CIM, conventional imaging modalities; mCRPC, metastatic castration-resistant prostate cancer; mHSPC, metastatic hormone-sensitive; nmCRPC, non-metastatic castration-resistant prostate cancer; tbNGI, total-body next-generation imaging.
In patients with only biochemical or with both clinical and biochemical progression, PSMA PET/CT was the most largely used investigation, whereas the use of wbMRI or PET/MRI was ⩽3%; fluciclovine PET/CT was not employed in this setting (Supplemental Material Questionnaire, Q 4.1, Q 4.3).
The presence of clinical progression in addition to biochemical progression does not significantly impact the re-staging modality (p = 0.42; Q 4.1, Q 4.3, Table 5). When asked about the criteria used to prompt for tbNGI assessment in case of biochemical progression, 56% identified PSA DT < 6 months as the most prominent one (Q 4.2, Table 3).
Topic 4. Re-staging in mCRPC
Similarly, to mHSPC, in the mCRPC setting, most participants (50%) choose a tbNGI investigation in case of biochemical progression during treatment. tbNGI remains the preferred choice even when biochemical progression is associated with clinical progression (45%) (Q 5.1, Q 5.3, Table 5).
Both in patients with only biochemical and patients with clinical and biochemical progression, PSMA PET/CT was the most largely used investigation (Supplemental Material Questionnaire, Q 4.1, Q 4.3), whereas the use of wbMRI or PET/MRI was ⩽2%; fluciclovine PET/CT was not employed (Supplemental Material Questionnaire, Q 5.1, Q 5.3).
As in the mHSPC setting, the presence of a simultaneous clinical and biochemical progression does not significantly modify the attitude of the participants (p = 0.66; Q 5.1, Q 5.3, Table 5). Having previously performed a tbNGI investigation represents the main reason (60%) for requesting a new tbNGI in case of biochemical progression during treatment for mCRPC (Q 5.2, Table 3).
Topic 5. Re-staging in nmCRPC
In the case of diagnosis of nmCRPC obtained with CIM, 14% of the participants declare that they request a further investigation with tbNGI in all cases, 76% require a further investigation with tbNGI only in selected cases, while only 10% never require a further investigation with tbNGI (Supplemental Material Questionnaire, Q 6.1). The main reasons for requesting further investigation with tbNGI include the presence of a doubtful finding with CIM (54%) and a PSA-DT < 6 months (41%) (Supplemental Material Questionnaire, Q6.1).
PSMA PET/CT is the most requested diagnostic method in case of additional investigation with tbNGI of a CIM-based nmCRPC diagnosis (60%), whereas 30% of participants opt for a Choline PET/CT (Supplemental Material Questionnaire, Q6.2). The use of wbMRI or PET/MRI was ⩽2%; fluciclovine PET/CT was not employed (Supplemental Material Questionnaire, Q6.2).
In the nmCRPC setting, 60% of interviewees would request tbNGI re-staging in case of biochemical progression when systemic therapy is ongoing. Also for clinical and biochemical progression, the majority’s choice falls on NGI (45%) although a tendency to significance was registered to indicate a greater propensity toward CIM in these conditions (p = 0.07; Q 6.3, Q 6.4, Table 5).
Both in patients with biochemical only or with clinical and biochemical progression, PSMA PET/CT was the most largely requested examination (Supplemental Material Questionnaire, Q 6.3, Q 6.4). In both patient groups, the use of wbMRI or PET/MRI was ⩽2%; none of the responders requested a fluciclovine PET/CT (Supplemental Material Questionnaire, Q 6.3, Q 6.4).
Topic 6. Re-staging in OMPC
In patients candidate for MDT for OMPC diagnosed with CIM, only 8% of participants declare that they never considered further investigation with tbNGI, 45% require further investigation with tbNGI in selected cases only, while 47% require an additional tbNGI investigation in all cases (Supplemental Material Questionnaire, Q1.1). Among those who require tbNGI only in selected cases, the presence of a PSA-DT < 6 months (33%) and a doubtful finding on the CIM (28%) represent the main reasons (Supplemental Material Questionnaire, Q 7.1).
With the last question, the participants were inquired on whether an imaging assessment is appropriate following MDT for OMPC, once biochemical control is achieved. Sixty-seven percent of participants declare that they do not perform any imaging tests in these scenarios, while 15% declare that they request the same test used before MDT (Supplemental Material Questionnaire, Q 7.2).
Discussion
This survey involved a large, multidisciplinary panel of professionals from North-Eastern Italy, mostly devoted to uro-oncology care, offering a reliable picture of current clinical practices in PCa.
Several key findings emerged. First, NGI techniques are increasingly accessible in daily clinical practice across North-Eastern Italy. PSMA PET/CT is still less accessible than choline PET/CT, and only a few participants can rely on PET/MRI or wbMRI. Therefore, it is our opinion that the results of this survey are representative of the availability and use of advanced diagnostic imaging technologies in many developed countries worldwide.
Second, our survey confirms that, when available, NGI techniques are routinely employed for the primary staging of PCa. Specifically, the use of mpMRI for T-staging stands at around 50%. Although the TNM classification still relies on digital rectal examination for cT-staging, 4 mpMRI is now considered the gold standard both for detection and T-staging accuracy,5,6 leading to better risk stratification, which correlates with improved oncological outcomes, 7 particularly for higher-grade tumors (ISUP ⩾ 2). 8
Regarding N/M staging, the survey confirms that the use of tbNGI increases in patients with higher NCCN risk groups.3,7,9 PET/CT with PCa dedicated radiotracers provides high diagnostic accuracy for detecting occult metastases at CIM, guiding treatment decisions, and avoiding unnecessary local therapies.10,11 This approach is supported by literature showing that PSMA PET/CT can reduce the costs associated with inaccurate staging. 12 Moreover, promising evidence suggests that PSMA PET/CT or PET/MRI could become a one-stop imaging modality for PCa detection and primary staging, particularly in patients with negative mpMRI scans.13 –15
Third, in suspected LR, most participants indicated that they would perform tbNGI alone, or in association with mpMRI.7,16,17 Unsurprisingly, radiation oncologists were significantly more prone to select the association of both imaging methods, as the fusion of functional and anatomic images is useful for radiation therapy planning. 18 Interestingly, only 3% of respondents required biopsy confirmation for LR in any case. Although histological confirmation is recommended before local salvage treatment, 9 studies have demonstrated the reliability of PSMA PET/CT, especially when combined with mpMRI.19 –21
For patients with BCR after radical prostatectomy, the use of tbNGI increased with higher PSA values. While PSMA PET/CT is capable of detecting recurrence even at low PSA levels,19,22,23 some participants preferred to delay imaging until PSA exceeds 0.5 ng/ml. This preference likely reflects the limited availability of PSMA PET/CT and the lower sensitivity of choline PET/CT at these PSA levels. However, when PSA exceeds 2 ng/ml, choline PET/CT is commonly used, likely due to its broader availability. Despite its lower sensitivity, choline PET/CT remains a useful tool in BCR patients with PSA values above 2 ng/ml, particularly when PSMA PET/CT is less accessible. 24
In patients with advanced disease, including mHSPC and mCRPC, tbNGI is favored for re-staging in case of disease progression. However, the added value of tbNGI in comparison to CIM remains unclear in metastatic PCa patients, 25 with updated guidelines suggesting that tbNGI should not be used routinely for treatment monitoring due to the lack of solid evidence.9,26,27 Nevertheless, in patients with clinical progression, tbNGI could be useful for a better understanding of the patient’s metastatic lesions, to guide eventual MDT.
In nmCRPC, tbNGI is preferred for re-staging of these patients, as PSMA PET/CT can identify metastases missed by CIM. 28 However, the deriving stage migration is likely due to a more accurate diagnostic technology rather than to a true disease progression, configuring a “Will Rogers Phenomenon.” Consequently, the real impact of the PSMA-derived upstaging on patients’ outcomes is still undetermined. 29 In addition, PSMA expression can be reduced or absent in low differentiated lesions, limiting the utility of PSMA PET/CT in CRPC.30 –32 As such, combining PSMA PET/CT with other imaging modalities, such as choline PET/CT or [18F]-FDG PET/CT, should be considered for patients with discrepancies between imaging and clinical data. 29
In patients with OMPC, the majority of respondents considered tbNGI prior to MDT. PSMA PET/CT is the most accurate tool for the early detection of lymph nodes and distant metastases and could potentially enable accurate MDT in OMPC patients.33,34 However, it remains unclear whether early detection of metastases through tbNGI improves survival outcomes or simply results in “lead-time bias.”35,36 Despite these uncertainties, most interviewees do not refrain from tbNGI before MDT, and 14% even request tbNGI after MDT to evaluate treatment response.
While the survey highlights the good availability of NGI technologies in North-Eastern Italy, access is often hindered by long waiting lists. Notably, 14% of respondents indicated they would stage FIR PCa with tbNGI, in contrast to current guidelines, and 33% performed re-staging in OMPC patients after MDT, irrespective of PSA values. These findings suggest the need for better patient selection and more appropriate prescription practices to optimize access to NGI.
The survey’s strengths include a large, experienced cohort of uro-oncologists and high response rates to a large number of items. However, its geographic focus limits the generalizability of the findings. Despite this, the results offer valuable insights into the use of NGI in different PCa settings.
In conclusion, this survey underscores the expanding role of NGI in the management of PCa in North-Eastern Italy. Further studies are needed to address the controversies identified in this survey and to develop an evidence-based, standardized, and cost-effective use of NGI.
Supplemental Material
sj-docx-1-tau-10.1177_17562872251321971 – Supplemental material for The expanding role of next-generation imaging in prostate cancer management: a cross-sectional survey exploring the clinical practice of uro-oncologists in North-Eastern Italy; on behalf of GUONE (Gruppo Uro-Oncologico del Nord-Est)
Supplemental material, sj-docx-1-tau-10.1177_17562872251321971 for The expanding role of next-generation imaging in prostate cancer management: a cross-sectional survey exploring the clinical practice of uro-oncologists in North-Eastern Italy; on behalf of GUONE (Gruppo Uro-Oncologico del Nord-Est) by Fabio Matrone, Luca Urso, Rossano Girometti, Jerry Polesel, Matteo Sepulcri, Francesco Pierantoni, Paolo Artioli, Anna Caliò, Irene Campo, Alessia Cimadamore, Enrico Munari, Luca Ongaro, Valentina Orlando, Camilla Sachs, Alessandro Veccia, Alessandro Antonelli, Roberto Bortolus, Matteo Brunelli, Orazio Caffo, Laura Evangelista, Matteo Salgarello, Umberto Basso, Rocco De Vivo, Mario Gardi, Andrea Guttilla, Marco Andrea Signor, Fabio Zattoni, Filippo Alongi, Giampaolo Montesi and Gianluca Giannarini in Therapeutic Advances in Urology
Footnotes
Acknowledgements
The authors would like to thank Daniela Michilin for her assistance in the final preparation of the manuscript and Lara Matrone for image optimization.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.