
Abstract
In this paper, we explore the usage of decision aids, patient information leaflets (PILs), videos, social media and modern technology to empower patients and enable shared decision-making (SDM). It explores the role of enhanced consent processes in urology. A re-evaluation of the conventional consent process is required towards more patient-centred care and SDM, which prioritises patient education and understanding of their medical conditions and treatment pathways. The use of decision aids, such as multimedia resources and PILs, is crucial in enhancing patients’ understanding, level of satisfaction, quality of life and healthcare utilisation. New tools are opening exciting possibilities for patient education and information distribution, such as Chat Generative Pre-Trained Transformer (ChatGPT). The effectiveness of ChatGPT in comparison to well-established PILs is still up for debate, despite the fact that it makes information easily accessible. Improving patients’ involvement, understanding and engagement in SDM procedures relies heavily on decision aids, PILs and current technological integration. Patients and healthcare practitioners should work together in accordance with the principles of SDM, which include considering patients’ values, backgrounds, priorities and preferences when making treatment decisions. The emphasis on patient-centred care has prompted a re-evaluation of traditional consent processes in urology, with more emphasis on the shared decision-making process. Several informative aids are currently available as reported in the literature, ranging from 3D models, multimedia presentations and virtual reality (VR) devices. While the costs of these tools might be substantial, the advantages of adopting such informative resources are unmistakable. Social media and platforms such as patient–physician blogs are increasingly popular sources of medical information. Urologists should embrace these platforms to enhance patient engagement and the quality of information provided. Despite recent progress, there remains significant room for improvement in patient education and engagement which is achievable via concerted efforts of a wider medical community.
Keywords
Introduction
The emphasis on patient-centred care has prompted a re-evaluation of traditional consent processes in surgical specialities as well as in the whole healthcare community. The integration of decision aids, informative leaflets, videos and cutting-edge technologies is revolutionising the landscape of comprehensive consent. Indeed, patient compliance and adherence to treatment are crucially influenced by education and comprehension of the medical diagnosis and therapeutic options. 1 However, unfamiliar medical terminology and anatomical details often impact patient understanding, and consequently engagement in clinical discussions and consultations. 2 In urology, as in many other specialties, this challenge is exacerbated by the complexity of visualising the urinary tract system and associated pathological conditions. 3 To bridge the gap between medical terminology and patient understanding, urologists often utilise information leaflets, illustrations and radiological images to facilitate comprehension of anatomy and related treatments.
Several authors have already investigated the application of simulation models in urology, demonstrating significant effects on surgical planning and patient counselling. 4 The introduction of three-dimensional (3D) imaging marked an advancement in patient–surgeon communication by offering a clear and volumetric representation of patients’ organs, 5 a capability even further stressed by virtual reality (VR), through which a real-time interaction and modification of the model is allowed. Moreover, with the spread of multimedia tools and social media interest towards healthcare issues, patients can now seek medical information and advice through online platforms and social networks such as YouTube, Twitter and Instagram. While the availability and spread of information can have a positive impact on material and data sharing, limited information is available on the quality and impact this has on public understanding and health.
Recent investigations have focused on examining the efficacy of the various tools for patient counselling and consent, but the findings are currently underreported, leaving questions about the potential effects on patients’ comprehension of their disease and planned interventions. It also remains uncertain whether the potential increase in additional knowledge would result in relief from distress or heightened anxiety towards their disease or procedure.
In this review, we aim to explore how these multifaceted tools (i.e., decision aids, leaflets, videos and newer technologies) collectively empower patients, fostering informed choices and facilitating shared decision-making (SDM) (Figure 1). Currently, there is insufficient evidence on the role of enhanced consent via these tools in shaping patient expectations, and consequently its impact on medico-legal aspects of their treatment. Our goal was to explore the tools that have been implemented to enhance patient consent and shared decision-making process for urological interventions, providing an overview and future directions, and assessing their effect on patient understanding, anxiety, and satisfaction.
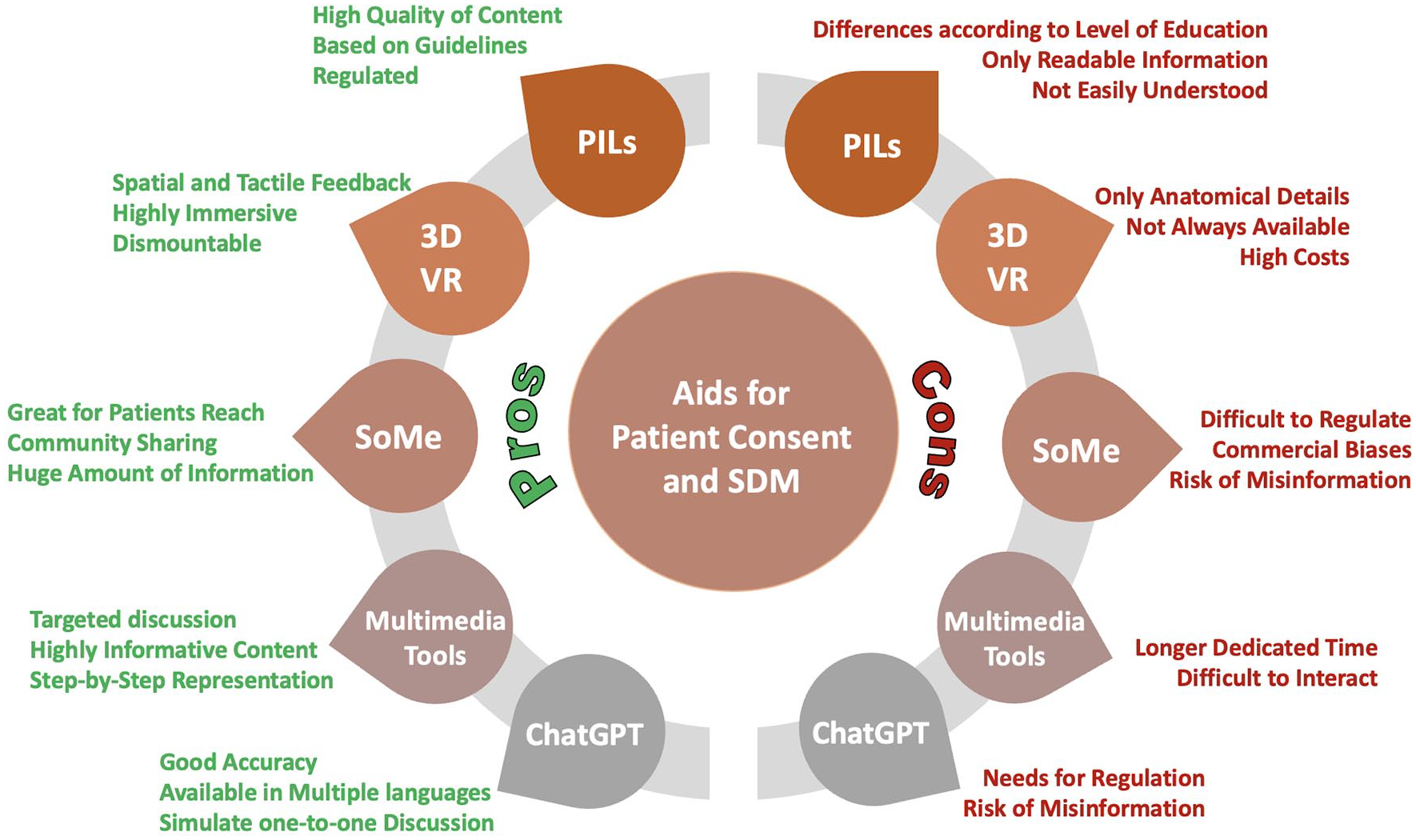
Pros and Cons of consent aids and SDM.
Materials and methods
A comprehensive search was carried out on PubMed, Embase and Google Scholar for eligible studies. The following terms and Boolean operators were used: (Decision Making OR Healthcare Communication OR Patient Education OR Patient Information OR Patient Consent OR Informed Consent OR Surgical Consent) AND (Virtual Reality OR Simulation OR Augmented Reality OR virtual simulation OR 3D models) AND (urological OR urology).
All retrieved studies were screened by two independent authors (CN and NN), and a third senior author (BKS) resolved discrepancies. We looked for original English-written studies reporting on the use of various informative devices for the patient’s information, informed consent and decision-making process. Preclinical studies, letters to the editor, case reports/case series and meeting abstracts were excluded. Full-text papers fulfilling the criteria were included in our review.
Given the significant variability in the protocols, outcomes and measures reported across the different studies, conducting a comprehensive statistical analysis or meta-analysis to compare results was deemed not feasible because of a lack of scientific significance. Therefore, we provided a narrative description of the reported outcomes, including an evaluation of the findings as presented by the respective authors. For a few selected studies, which utilised comparable outcome measures for similar devices and cohorts, an additional assessment of the statistical significance and magnitude of the effects was included.
Patient information leaflets
The primary aid to provide medical information to patients still remains via information leaflets. Patient information leaflets (PILs) are developed to improve knowledge and recall, symptom management, satisfaction, preferences, healthcare utilisation, and affective states. The positive effect of PILs on numerous patient‑related outcome measurements (PROMs) has been reported, with particular benefit in patients with a diagnosis of cancer. 6
PILs are available from the patient offices of urological associations such as European Association of Urology (EAU) https://patients.uroweb.org, American Urological Association (AUA) https://www.auanet.org/meetings-and-education/educational-programmes/patient-education and British Association of Urological Surgeons (BAUS) https://www.baus.org.uk/patients/information_leaflets/. The EAU has published evidence-based information for patients with urological conditions such as bladder cancer, prostate cancer, kidney cancer, kidney stones and many other urological conditions. 7 These PILs are primarily based on the clinical guidelines developed by EAU, and the content is converted to plain language to help patients better understand the information provided. 8 To this aim, EAU’s Patient Advocacy Group and language specialists are involved in the development of printable PILs.
The need for understandable PILs has been pointed out by Buyens et al. 9 In their study, they investigated cancer literacy within Europe which was found to be uneven across and within countries, with social groups systematically less informed and skilled regarding cancer care. Similarly, Graham and colleagues examined the comprehension of the leaflets provided by the BAUS, which are available for more than 150 urological procedures (www.baus.org.uk/patients/information_leaflets). They found that BAUS PILs require a relatively high level of education to be fully understood, which prevents their use as the only source of information for a substantial proportion of the population. Assessing readability with three different scores, Graham’s study revealed that the majority of PILs were written above the reading level of an 18-year-old, and at least 43% of the population would realistically have significant difficulty understanding them. While PILs can be used as an adjunct to clinical discussions, it is essential to ensure that all the information necessary to make an informed decision has been conveyed in a way that can be understood by the patient. Again, the importance of appropriate plain language for PILs is stressed, and this should be kept in mind by urologists while discussing medical issues with patients with different levels of education. 10
While the primary medium used for the provision of PILs remains a paper‑based format, with the emerging and cost‑competitive technologies, information can now be provided on an electronic tablet, with the added benefits of potential audio‑visual information, as illustrated in a study by Miha et al. 11 Using electronic PILs for information on prostate cancer, they reported positive feedback from patients, with the possibility of easily downloading and sharing content, while reducing the carbon footprint of paper PILs. 12 Both standard and electronic PILs demonstrated good feedback on patients’ information, with the material being comprehensive and easy to understand (positive responses > 90% in both groups); over 90% of the tested patients were satisfied with electronic PILs experience, while a small percentage reported a preference for paper PILs. In conclusion, they state that, even if printed material should still be available, the natural evolution of the provision of PILs should be through electronic devices.
3D models and VR
With the introduction of printable realistic 3D models, that can be patient-specific, dismountable and explanatory of the basic anatomical features, urologists have been increasingly interested in using these applications for medical teaching and patient education. 3D models can translate medical information into a visual language that is easy to understand. A discussion aided by the utilisation of a 3D printed model improves patient comprehension, thereby enhancing the quality of communication and therefore patient satisfaction.
In a study conducted by Wake et al. 13 on the impact of 3D printed models for renal and prostate cancer, 3D models were reported as having a positive impact on patient understanding of anatomy, with better outcomes compared to traditional imaging. With the ability to offer spatial comprehension and tactile feedback, 3D models improve patient comprehension of organs and tumour size, shape and location, easing the discussion on specific techniques or surgical procedures. 14
Nevertheless, 3D models have a financial impact on hospital costs, as the development costs differ in literature, ranging from $50 to over $500. 15 Moreover, even if they improve patient understanding of anatomy and surgical intent, 3D models are not able to show procedural steps fully and/or improve the understanding of operative risks.
To overcome this limitation, some authors have reported on the incorporation of 3D models in a VR setting, enabling the patient to fully immerse in a virtual anatomical space, where a simplified simulation of surgery can be witnessed. 16 In a discussion assisted by VR models, the urologist would be able to explain the procedure with visual aids, while being immersed in this, the patient receives this information and can interact with the VR simulation and/or urologists. This way, a hyper-realistic simulation would improve patient understanding of the surgical procedure and relative risks, possibly improving patient expectations and postoperative satisfaction. 17
Our search retrieved nine prospective controlled trials on the use of 3D models for patient information and shared decision-making (SDM).13–16,18–22 The summary of findings for these studies is reported in Table 1. A total of 8 out of 9 papers13,14,16,18–22 found a significantly positive impact on patient understanding due to the introduction of the model, and the remaining one stated a non-significant impact of the enhanced consent process (Figure 2). A total of six authors13,16,18–20,22 also investigated the role of enhanced consent on patients’ emotions, reporting a positive effect on anxiety reduction, distress relief and compliance intent. Only three of the retrieved studies included SDM among the outcomes.13,18,19 Three of them agreed on saying that the increased understanding of the disease, the planned procedure and the involved risks made the patients feel more involved in the process, increasing the quality of the patient–surgeon relationship and the willingness to comply with the treatment (Figure 2 and Table 1).
Studies reporting on the role of 3D models for patient information and consent.
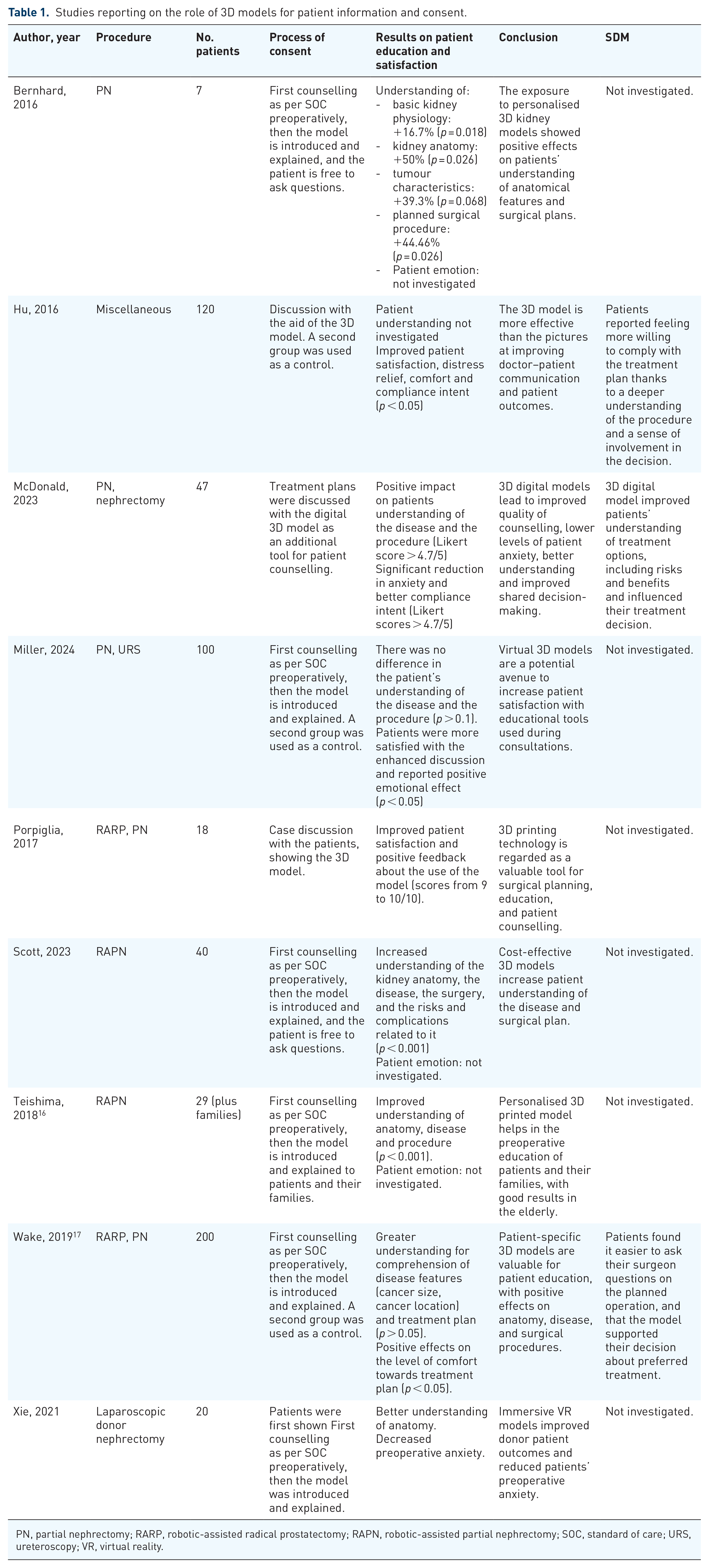
PN, partial nephrectomy; RARP, robotic-assisted radical prostatectomy; RAPN, robotic-assisted partial nephrectomy; SOC, standard of care; URS, ureteroscopy; VR, virtual reality.

Forest plot describing the reports on the usefulness of 3D models in patients’ consent. For each study, OR of patients’ reported usefulness of 3D models and corresponding errors are reported.
The impact of social media on patient education
Recently, the impact of social media (SoMe) in interpersonal communication has grown rapidly, and so has the use of SoMe for medical education. 18 The public is now using SoMe to obtain and share medical information in an understandable format, easy to share and always available. Different urological content is available among the SoMe platforms, ranging from cancer to benign diseases such as erectile dysfunction, 19 prostatic hyperplasia and urinary tract infections. 20 Several urological associations, such as AUA and EAU, now have Twitter accounts and hashtags for different diseases, through which patients and professionals can discuss and share information.
As investigated by Saade et al., 21 SoMe can improve patient engagement with treatment by expanding education and networking, but care must still be taken as the impact on patient care and satisfaction is still to be proven, and misinformation can lead to negative effects. As shown by Loeb et al. 22 there is a significant amount of misinformative and biased urological content on SoMe, sometimes even with commercial intent, that different organisations are making efforts to combat. They found that most of the articles shared about urologic oncology on Facebook, Twitter, Pinterest and Reddit are inaccurate, and most of the uro-oncological videos on YouTube are potentially biased and/or misinformative. Similarly, almost 20% of YouTube videos about kidney stones contain false or misleading information, and the same is reported for videos on sexual medicine and infertility. Moreover, Loeb reported on the high commercial content present in SoMe, with the highest rate (30–40%) found for incontinence on Facebook, Twitter and YouTube posts.
SoMe also provide online groups and platforms for patient interaction and discussion, where different topics can be found, from informative content and experience sharing to emotional support. 23 This way, communities of patients can gather and share access to certified medical information, from the FDA-approved blog on androgen deprivation therapy for prostate cancer (https://www.cancerabcs.org/advanced-prostate-cancer-blog) to other patient-centred social sites such as Smart Patients (www.smartpatients.com) and Patients Like Me (www.patientslikeme.com). Another useful exploit of SoMe is the possibility to reach and recruit patients for innovative treatments and clinical trials through these blogs, a powerful tool that indeed needs regulation to avoid misinformation. 24
The most investigated SoMe platform is by far YouTube, where an enormous number of healthcare- and urological-based videos can be found. Several authors have investigated the role played by YouTube in patient education and misinformation. Contrary to the reports previously described by Loeb, Siegel and colleagues positively reported on the quality of the most viewed videos on radical prostatectomy. 30 Even if overall medical content was not of high quality in the 179 analysed videos, they found good technical quality, reliability and overall content, especially for robotic radical prostatectomy videos. Moreover, the quality of videos was deemed significantly higher when performing a search sorting by relevance rather than views. On the other hand, Di Bello investigated the content of 121 testicular cancer videos on YouTube, 31 describing the unreliability of the information found on this platform. In this study, understandability was acceptable at 60%, actionability high at 100%, but misinformation was significant (Likert score 2.8/5). Videos on testicular cancer were in fact found to underestimate several aspects, such as testicular self-examination, risk factors and physiopathology of the tumour, and the effects on fertility due to treatment options. On the subject of immunotherapy for urological tumours, Di Bello had comparable findings with misinformation scores ranging from 2.3 to 4 over 5 according to the topic. 32 Similar results were reported by Warren and colleagues in 2016, in a study analysing YouTube content for hypogonadism: most of the studies were found to be unreliable, and the presence of a physician significantly impacted the quality of videos with improved reliability (p < 0.001). They concluded that there is a huge need for regulation and approval of the validity of the information given on the disease and the possible treatment options. 33
Multimedia tools
Multimedia presentations and platforms can be used as informative tools to enhance patient’s understanding and participation in the consent process. Through the explanation of images, animation and videos the urologists can better discuss the anatomical and procedural features, providing an explanation divided into steps, resembling a rapid lecture or presentation. Moreover, some authors reported on the use of interactive presentation, enabling the patient to interact with the informative content. Huber et al. 34 performed a prospective study on 203 patients undergoing radical prostatectomy and patients were randomised into a standard consent process or enhanced education via an interactive multimedia platform including illustrations, video sequences, pictures and textual content. Comparing the groups after discussion and counselling, they found increased satisfaction with the interaction for the multimedia platform cohort (p = 0.016), alongside the increased quality of questions from the patient (p = 0.018) and perceived knowledge (p = 0.037). The use of the multimedia tool did not affect the length of the discussion, and there was no significant impact on preoperative anxiety. The results show a positive impact on patient education and satisfaction, highlighting the feasibility of enhanced discussion in a clinical setting. Another comparative study by Gyombert et al. 35 reported on the use of a multimedia platform for radical prostatectomy, assessing patient’s knowledge with an objective test on critical aspects of the procedure and potential complications. They found significantly higher scores in knowledge (p < 0.001) in the enhanced-consent cohort, suggesting a better understanding of the implications of surgery.
Even if the quality and the content of the multimedia presentation result are more accurate and possibly more information compared to a standard discussion, it seems that the use of the multimedia tool does not impact the length of the conversation, thus avoiding prolongation of the consent process. 25 This is particularly significant in a hospital setting, unfortunately, characterised by the lack of additional time to dedicate to the patient discussion.
AI platforms like ChatGPT
Another recently emerged tool for patients’ education is the Chat Generative Pre-trained Transformer (ChatGPT, available at https://chat.openai.com/). This relatively new platform can generate educational material in plain language, being able to respond to specific healthcare and urological questions.
Through a virtual one-to-one discussion, ChatGPT can be used to discuss medical conditions and treatments, with even insight into urological procedures and relative risks and benefits. Several studies investigated the appropriateness and validity of the contents generated by ChatGPT, with overall promising results. 26 While being able to retrieve a good amount of information, ChatGPT’s ability to answer urological questions is however limited by the lack of clarity and accuracy, especially when compared to EAU’s PILs. 27 Nevertheless, the precision of ChatGPT responses seems to improve when dealing with urological surgical treatments compared to disease explanation. In a study by Gabriel and colleagues investigating ChatGPT performance, they reported excellent results, with high concordance and comparable information between ChatGPT and the BAUS PILs on robotic prostatectomy. 28 Moreover, being tested on urolithiasis ChatGPT was able to answer correctly to over 95% of questions on diagnosis and treatment by Cakir and colleagues. 29
Even if concerns remain about the lack of regulatory systems and privacy issues, ChatGPT could severely improve patient education and serve as a powerful tool for the decision-making process. With the expected progress that will expand ChatGPT accuracy and ability to provide precise information without endangering a patient’s health perspective, it could become a valuable instrument for patient education and enhanced care. 30 As a pre-clinical tool, in fact, ChatGPT could provide the patient with basic but correct urological education, improving the quality of discussion at the time of consultation and consent, and overall increasing the patient’s understanding and awareness.
Shared decision-making
SDM is a commonly used term in healthcare, also encouraged by international guidelines. SDM is based on patient preferences as a key component to ensure effective, patient-centred care, and requires intentional and cooperative communication between the patient and the urologist, aiming at delivering high-quality care. 31
For good SDM, the physician must combine medical knowledge and expertise with the patient’s values, life priorities and preferences. To achieve this, it is important to understand the reasoning behind patients’ decisions or choices and to also clarify its effect on long-term quality-of-life outcomes. 32 Other fundamental aspects playing a role in SDM and patient perspective are trust and respect, qualities that are not always easily delivered. 33 Indeed, SDM is a patient-centred approach but comprises other factors in the healthcare system.
The concept of SDM has also been investigated by the Agency for Healthcare Research and Quality, which defined it within the five steps of the S.H.A.R.E. approach. 34 Firstly, the importance of seeking patient participation is stressed, where new technologies and SoMe could help. Secondly, the patient must be educated on the treatment options and given tools to navigate among the possibilities. Again, educational aids such as multimedia content and the availability of a broad discussion could be of benefit. Thirdly, the S.H.A.R.E. approach asks the physician to assess the patient’s values and preferences, a fundamental step to reach the fourth stage, to decide with the patient. Once the final goal is achieved, the urologist would be required to objectively evaluate patients’ decisions and help them recognise possible biases, and if needed counsel them further.
A good example of implementing SDM is provided by the ‘patients friendly’ multi-disciplinary meetings (MDT), where the patients and even the family members receive a full overview of the possible treatment options, alongside the alternatives. In the MDT, the patient often perceives better quality of care, due to the presence of a structured team, that is felt to be more objective and therefore trustworthy. 35
Patient subgroups – differences in age and level of education
If multimedia tools and other simulation aids are showing promising results in improving patients’ understanding of the disease and compliance towards the proposed treatments, questions remain on whether the social background and level of education might influence their accessibility. Studies have generally found good patient acceptance and satisfaction in different subgroups, regardless of age and level of education. 36 Readability of difficult and specific information (i.e. for PILs) might negatively influence the transmission of information and therefore the effectiveness of the discussion. 9 On the other hand, multimedia tools and simulation devices seem to attract even more attention for low-education subgroups. 37 It appears in fact that the information provided by simplified figures, images and sounds might help in driving attention and transmitting the message more effectively than a plain discussion. If concern remains on the accessibility of some platforms and devices, the main advice is still to keep them as simple as possible, enabling the patients to immediately get comfortable with the technology and be able to easily navigate it to get the most from the informative aid. 38 Further studies will be however required to deeply investigate the possible difference of effectiveness among the available devices, according to age, educational and cultural subgroups.
Current limitations
The most obvious limitation of the SoMe and multimedia tools described in the present study is with regards to older patients, and/or patients less familiar with technological nuances. With large amounts of informative material available through the internet, this population might struggle with the virtual tools given by the urologist at the end of a discussion. For example, the addition of a QR code leading to an explanatory video to a PIL could sound easy and effective, but it might not be intuitive or easily accessible by those not using this technology.
Moreover, some materials might only be available in certain languages, and this could represent an obstacle to the education of immigrant patients. For those, the use of translated PILs or the addition of various language options to blogs, chatbots or other multimedia tools could improve the quality or spread of information delivered. In fact, too often, immigrants feel on average less involved in the SDM process, and it is the duty of the physician to try to overcome this gap. 39 Perhaps the use of Patient reported outcome measures (PROMS), nomograms and scoring systems can also help in patient counselling and measuring and comparing clinical patient-centred outcomes.40,41
Readability scores indicated that the readability of patient education materials (PEMs) or PILs may be too low, 42 potentially limiting patient understanding. Therefore, better efforts must be made to improve this and prevent patients from resorting to web searches that could lead them into the harmful trap of fake news. 43 Finally, the lack of additional time for discussion with patients and their families is a clear limitation to the quality of the decision-making process. The use of educational tools and decision aids possibly represent at least a partial solution to the problem, enabling patients to navigate options and learn about the disease and the possible treatment options, thus improving the quality and efficacy of the face-to-face discussion. However, it is of extreme importance that the urologist does not totally rely on the decision aids or on moving the discussion to a virtual setting entirely, thereby avoiding a direct interaction. However, these instruments and aids should be used to improve the SDM process and by empowering patient’s understanding.
Some limitations of the present report need to be addressed. There is still a lack of scientific evidence in current literature, that did not allow for a thorough report on the impact of the different modalities of patients’ education. This is particularly true for SoMe and AI platforms, whose reports are mainly narrative and subjective in nature. Further comparative studies analysing the role of online education will be needed to better assess the possible impact on healthcare. Due to the lack of scientific evidence, our report is a preliminary analysis of what could possibly evolve in the close future, deeply impacting the urological world. We recognise that the unavailability of comparative materials and the consequent impossibility of performing a systematic review and a metanalysis will require further evaluation on the matter.
Future developments
Despite recent efforts to improve patient education and SDM, significant gaps remain, and more work needs to be done. With advancements in technology and the varied sources of information accessible today, patients deserve access to high-quality information, education and counselling. Standardising informational materials and regulating them via protocols and guidelines could enhance the awareness and knowledge of patients. In this pursuit of improved SDM and patient satisfaction, perhaps urologists and other healthcare professionals need to work collaboratively to enhance current practices. The use of all available and future technological resources need to be used in conjunction with essential human connections.
Take home messages
The significance of patient-centred care has prompted a re-evaluation of traditional consent processes in urology, and more should be offered on the shared decision-making process.
Several information aids are currently available ranging from 3D models, multimedia presentations and VR devices. The costs of these tools must be balanced against the advantages of adopting them.
Social media and platforms such as patient–physician blogs are increasingly popular sources of information and urologists should embrace these platforms to enhance patient engagement and the quality of information provided.
SDM is a fundamental part of the patient–urologist relationship. It is not just a means to convey information but a mutual exchange of information that considers the patient’s background and preferences.
Despite recent progress, there remains significant room for improvement in patient education and engagement which can be achieved by working together and embracing the technological innovations to support it.