
Abstract
Background:
Aspergillosis localized to the kidneys and the urinary tract is uncommon. We conducted a comprehensive systematic review to evaluate risk factors and clinical outcomes of patients with isolated renal and genito-urinary tract aspergillosis.
Methods:
We systematically searched Medline, CINAHL, Embase, African Journal Online, Google Scholar, and the Cochrane Library, covering the period from inception to August 2023 using the key terms ‘renal’ OR ‘kidney*’ OR ‘prostate’ OR ‘urinary bladder’ OR ‘urinary tract*AND ‘aspergillosis’ OR ‘aspergillus’ OR ‘aspergilloma’ OR ‘mycetoma’. We included single case reports or case series. Review articles, guidelines, meta-analyses, animal studies, protocols, and cases of genitourinary and /or renal aspergillosis occurring as a part of disseminated disease were excluded.
Results:
We identified 91 renal and urinary aspergillosis cases extracted from 76 publications spanning 1925–2023. Among the participants, 79 (86.8%) were male, with a median age of 46 years. Predominantly, presentations consisted of isolated renal infections (74 instances, 81.3%), followed by prostate (5 cases, 5.5%), and bladder (7 cases, 7.7%) involvement. Aspergillus fumigatus (42.9%), Aspergillus flavus (9.9%), and Aspergillus niger/glaucus (1.1% each) were isolated. Underlying risk factors included diabetes mellitus (29.7%), HIV (12.1%), haematological malignancies (11%), and liver cirrhosis (8.8%), while common symptoms encompassed flank pain (36.3%), fever (33%), and lower urinary tract symptoms (20.9%). An autopsy was conducted in 8.8% of cases. Diagnostic work-up involved histopathology (70.5%), renal CT scans and urine microscopy and culture (52.6% each), and abdominal ultrasound (17.9%). Treatments included amphotericin B (34 cases, 37.4%) and azole-based regimens (29 cases, 31.9%). Nephrectomy was performed in 16 of 78 renal cases (20.5%). All-cause mortality was 24.4% (19 cases). No significant mortality rate difference was observed among antifungal regimens (p = 0.739) or nephrectomy status (p = 0.8).
Conclusion:
Renal and urinary aspergillosis is an important cause of morbidity and mortality, particularly in immunocompromised and people with diabetes mellitus. While varied treatment strategies were observed, mortality rates showed no significant differences based on treatments or nephrectomy status. Further research is needed to refine diagnostics, optimize treatments, and enhance awareness among clinicians for early detection and management.
PROSPERO registration number:
CRD42023430959.
Plain language summary
In this study, we investigated the rare occurrence of aspergillosis, a fungal infection caused by the mold Aspergillus, specifically affecting the kidneys and urinary tract (ureters, urinary bladder, prostate and urethra). This disease was first described in 1891 in Germany. To update our current understanding of this rare disease, we conducted a thorough review, examining risk factors and outcomes for individuals with Aspergillus infection of the kidney and/or urinary tract. We found 91 cases from 76 published articles spanning nearly a century, identifying common features such as predominantly male patients (almost every 9 in 10 cases) and isolated infection of one or both kidneys being the most common (8 in 10 cases). Diabetes mellitus, HIV infection, and certain cancers were noted as underlying risk factors, with symptoms ranging from flank pain, passing of blood in urine, passing of fungal particles (bezoars) in urine, pain while passing urine to fever. Diagnostic methods included histopathology and imaging techniques, while treatments varied, involving antifungal medications such as voriconazole and amphotericin B, drainage of abscesses, and, in some cases, surgical removal of the affected kidney (nephrectomy). Overall, about 1 in every 4 of the affected people died. Despite diverse treatment approaches, the study found no significant difference in mortality rates, emphasizing the need for further research to improve diagnostics, refine treatments, and raise awareness for early detection and management, especially among immunocompromised individuals such as those with diabetes mellitus and HIV infection.
Keywords
Introduction
Aspergillosis, caused by several species of the opportunistic fungal pathogen within the Aspergillus genus, primarily manifests as a pulmonary disease; however, instances of extra-pulmonary dissemination and localized diseases are well described.1–3 Findings from autopsy studies show that extra-pulmonary aspergillosis, involving the heart, kidney, central nervous system, gastrointestinal tract, spleen, liver, thyroid gland and pancreas, occurs in over 50% of cases of invasive aspergillosis.4,5
Renal and urinary tract aspergillosis is an infrequent yet potentially severe fungal infection that affects the genital urinary system, posing significant clinical challenges, particularly in individuals with notable immunosuppression. 6 While the kidneys are the organs most frequently affected, there have been occasional instances of involvement of the urinary bladder, prostate, ureters, and urethra.7–10 In autopsy series of HIV decedents, kidney involvement was documented in about 15% of fatal cases of invasive aspergillosis. 11 Infections in the urinary tract can arise from haematogenous spread originating from disseminated aspergillosis or contiguous spread from adjacent organs, such as an intra-abdominal source. 6 In experimental murine aspergillosis, infected intravenously, the kidneys carry the highest burden of infection.12,13 However, isolated cases of renal and urinary aspergillosis occuring in patients without evidence of systemic dissemination has been documented,14,15 and one case acquired peri-operatively. 16
Much as isolated renal aspergillosis can occur in apparently immunocontent individuals, 17 important risk factors for isolated renal aspergillosis include genito-urinary instrumentation, HIV/AIDS, solid organ transplantation, haematological malignancies and bone marrow transplantation, and other forms of immunosuppression.18–20 Diagnosis of genito-urinary aspergillosis is often challenging as symptoms such as flank pain, urinary tract obstruction, haematuria, and constitutional symptoms are non-specific in terms of the underlying aetiological agent. 21 Medical imaging, diagnostic autopsies, and histopathological examination of biopsy specimens are required for definitive diagnosis.5,18,22
A fundamental challenge in therapy is that none of the available antifungal agents with activity against Aspergillus spp. penetrate the urine, although they do get into renal, bladder and prostate tissue. 23 A combination of surgical and medical therapies, including nephrectomy and prostatectomy, with or without systemic antifungal treatment, has been employed to treat renal and genitourinary tract aspergillosis, resulting in varying outcomes.24–26 The objective of this systematic review was to comprehensively analyse documented cases of isolated renal and genitourinary tract aspergillosis, aiming to investigate the clinical presentation, risk factors, diagnosis, management, and clinical outcomes of patients affected by this relatively uncommon form of aspergillosis.
Methods
Protocol and registration
This systematic review was conducted following the preferred reporting items for systematic review and meta-analysis (PRISMA) guidelines 27 and the study protocol was prospectively registered with PROSPERO (Registration number: CRD42023430959).
Eligibility criteria
The inclusion criteria consisted of articles describing histologically proven or culture-confirmed cases of isolated renal and/or genitourinary tract aspergillosis involving adults or children following the PEO (
The population, exposure, and outcome criteria.

Database search
A qualified medical librarian (BM) systematically conducted searches across numerous databases, including Medline, CINAHL, EMBASE, African Journal Online, Google Scholar, and the Cochrane Library, covering the period from inception to August 2023. The Medical Subject Headings (MeSH) terms and keywords ‘renal’ OR ‘kidney*’ OR ‘prostate’ OR ‘bladder’ OR ‘urinary tract*’
AND ‘aspergillosis’ OR ‘aspergillus’ OR ‘aspergilloma’ OR ‘mycetoma’, and [Aspergillosis AND (renal OR kidney* OR urinary tract* OR bladder OR prostate)] were used. Furthermore, a manual examination of references from all citations meeting our study’s inclusion criteria was carried out. The search results were exported and processed through RefWorks to eliminate duplicate research articles.
Inclusion and exclusion criteria
We included single case reports or case series. Review articles, guidelines, meta-analyses, animal studies, environmental studies, protocols, and cases of genitourinary and/or renal aspergillosis occurring as a part of disseminated disease were excluded.
Data screening and extraction
Four authors (BM, BEE, MFM, WK) conducted independent assessments of search outcomes to establish eligibility by screening titles and abstracts. Retrieval of pertinent full-text articles was undertaken. Additionally, scrutiny of the bibliographies from the search findings was performed. We systematically eliminated duplicated and repetitive findings, non-English articles, as well as reports with inadequate patient information. English-language articles that encompassed essential patient particulars were selected through a meticulous process. Any disagreements regarding inclusion were resolved through a collaborative consensus. FB undertook a comprehensive review and provided ultimate endorsement for all the included papers.
Two sets of independent reviewers extracted data (BM and BEE, and MFM and WK), which was subsequently coded. We used a data extraction form prepared using Microsoft Excel 2016 to collect information from all eligible studies such as year of publication, first author’s name, number of cases, method of diagnosis, aspergillus species, autopsy, antifungal agents used and duration, and clinical outcomes (survived or died). FB independently reviewed the extracted data, and any disagreements were resolved by consensus.
Risk of bias assessment
All included studies were either single case reports or case series including less than 10 participants and hence were not eligible for risk of bias of assessment since these studies are considered anecdotal evidence and are often included in systematic reviews to provide insights, generate hypotheses, or to illustrate clinical observations rather than drawing definitive conclusions about treatment effects.
Statistical analysis and data synthesis
Patient demographic data, clinical manifestations, underlying comorbidities, diagnostic procedures, antifungal treatment modalities employed, treatment duration, and clinical outcomes were meticulously scrutinized and recorded within Microsoft Excel spreadsheets. Descriptive statistical analyses, encompassing measures of central tendency such as mean, median, and range, were employed to present the variables and resultant outcomes. A chi-square test was conducted to compare clinical outcomes across treatment regimens and nephrectomy status among patients with renal aspergillosis. No meta-analysis was conducted, given that data pooling was not warranted.
Ethics statement
No ethical approval was required for this study as the underlying data were retrieved from publicly available sources.
Results
Search results
From the literature search, 2112 articles were identified from different sources. Of the total articles, 801 duplicate articles were excluded using RefWorks and manual tracing. The remaining 1311 articles were screened by reading their titles and abstracts; 1126 articles were excluded. Of the 185 studies sought for retrieval, 10 articles were not accessible in full text, and 175 articles were screened for full-text assessment. Finally, 99 articles were excluded for various reasons and 76 articles were included in the synthesis and analysis, Figure 1.

Preferred reporting items for systematic review and meta-analysis flow diagram.
Patient demographics and comorbidities
In total, our study encompassed 76 publications spanning from 1925 to 2023, which collectively involved 91 patients, with 79 (86.8%) of them being males. The median age of all participants was 46 years, (range: <1 month to 79 years). Fifty-four (59.3%) of the cases were aged 40 years or older.
The data were sourced from 27 different countries, with most cases originating from India (n = 32, 35.2%), USA (n = 16 cases, 17.6%), Spain (n = 5, 5.5%), Turkey (n = 4, 4.4%), and three cases (3.3%) each from Brazil and France (Figure 2).
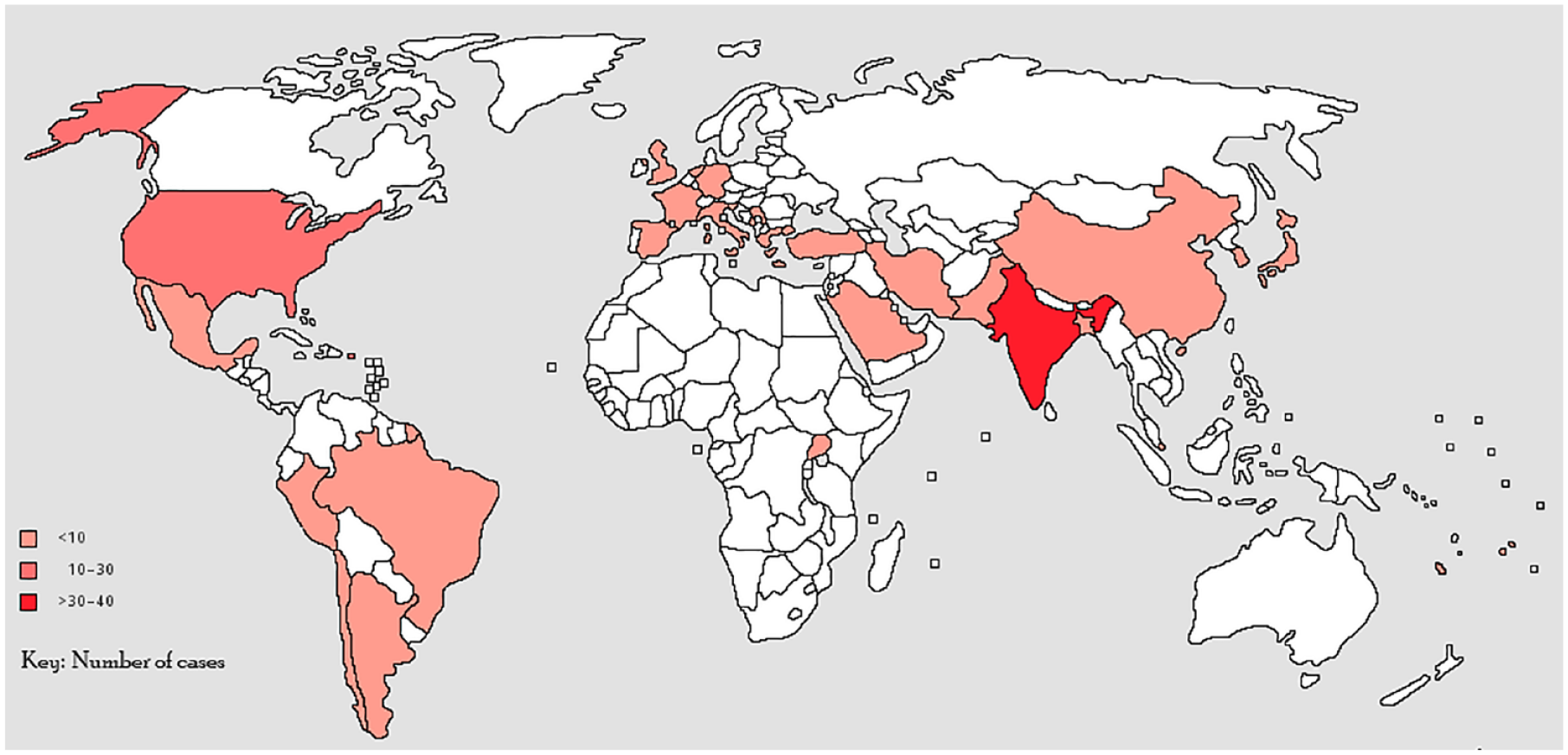
Distribution of isolated renal and genito-urinary tract aspergilloses cases reported across the globe.
Spectrum of renal and genito-urinary aspergillosis
Most cases involved isolated renal presentations, accounting for 74 instances (81.3%). Prostate involvement was observed in five cases (5.5%), and bladder involvement was noted in seven cases (7.7%). One case (1.1%) demonstrated a combination of renal and bladder involvement, and three cases (3.3%) presented with both renal and prostate involvement. Additionally, a single case (1.1%) was associated with only the ureter.
Among the 78 renal cases, 32 had specifications on involvement; bilateral involvement was observed in 20 cases (25.6%), left kidney involvement in 8 cases (10.3%), and right kidney involvement in 4 cases (5.1%), with specific pathologies including abscesses in 15 (19.2%) cases, aspergillomas in 10 (12.8%) cases, pyelonephritis in 1 (1.3%), and papillary necrosis in 1 (1.3%), Table 2.
Study characteristics, demographic, clinical characteristics, management, and outcomes of included classes.

Abd US, abdominal ultrasound; AIDS, acquired immunodeficiency syndrome; ALL, acute lymphoblastic leaukeamia; AMB, Amphotericin B; BDG, Beta-
Underlying risk factors
Nineteen cases (21%) had no reported underlying conditions whereas 27 cases (29.7%) had diabetes mellitus, 11 cases (12.1%) were associated with HIV, 10 cases (11%) were linked to haematological malignancies, 8 cases (8.8%) involved liver cirrhosis, and 5 cases (5.5%) each were related to renal transplant and injection drug use, Table 2.
Clinical presentation
The cases exhibited a range of symptoms, including 10 (11%) being asymptomatic, 33 (36.3%) experiencing flank pain, 30 (33%) presenting with fever, 19 (20.9%) showing lower urinary tract symptoms (LUTS), 14 (15.4%) having haematuria, 14 (15.4%) displaying particles in urine (fungal balls or bezoars), and 7 (7.7%) presenting with other systemic symptoms such as weight loss and fatigue.
Diagnosis
Among the 91 cases, 41 individuals (45.1%) exhibited histopathological evidence of Aspergillus infection, yet the specific species remained unidentified. Of the 50 cases where species identification was achieved, 39 (42.9%) were identified as Aspergillus fumigatus, 9 (9.9%) as Aspergillus flavus, and 1 (1.1%) each as Aspergillus niger and Aspergillus glaucus. Autopsy procedures were conducted on eight participants, representing 8.8% of the study population. Of the 78 cases of renal aspergillosis, diagnoses were mostly established through a combination of diagnostic methods. However, details of diagnostic workups were not provided for 5 cases. Histopathology of biopsy or autopsy samples was the primary diagnostic method for 55 cases (70.5%). This was followed by renal CT scans and urine microscopy and culture (MCS), both utilized in 41 cases (52.6%). Abdominal ultrasound was utilized in 14 cases (17.9%), while MRI or PET scans were used in 3 cases (3.8%). Galactomannan antigen tests were conducted in 4 cases (5.1%), Table 2.
Treatment
Sixty-three cases received antifungal therapy, with 34 (37.4%) individuals receiving amphotericin B-based treatment. This included cases where amphotericin B alone was administered (11 cases), in combination or followed by itraconazole (9 cases), and voriconazole (7 cases). In addition, flucytosine (5FC) was given in three cases, and 1 case each received amphotericin B with caspofungin and posaconazole, or isavuconazole and anidulafungin, or itraconazole and fluconazole.
Furthermore, 29 (31.9%) patients were treated with azole-based regimens, primarily voriconazole alone (n = 16) or in combination with caspofungin (n = 3). Other cases involved itraconazole alone (n = 6), in combination with voriconazole (n = 1), or 5FC (n = 1). Single instances of treatment with isavuconazole or caspofungin were also observed. The duration of treatment varied widely, ranging from as short as 1 week to 18 months. The treatment was not stated for 20 (22%) cases, and 7 (7.7%) cases received no antifungal treatment.
In terms of surgical procedures, a total of 19 patients underwent surgery. Among the cases of renal aspergillosis, 16 out of 78 (20.5%) underwent nephrectomy. Additionally, 2 of 8 (25%) cases involving the prostate underwent prostatectomy, while 1 of 8 (12.5%) cases concerning the bladder underwent radical cystectomy. A total of 13 (22.8%) of 57 patients with available surgical and antifungal therapy status were managed with both nephrectomy and antifungal therapy, Table 2.
Clinical outcomes
A total of 78 patients had documented clinical outcomes, including 19 (24.4%) fatalities, all linked to renal aspergillosis, Table 2. Thus, of the 67 isolated renal aspergillosis cases, mortality was 28.4% (19/67). Among the 19 fatal cases who died, 10 patients had received amphotericin B-based regimens, 2 received itraconazole, 1 was treated with a combination of voriconazole and caspofungin, 2 had no antifungal treatment, and 4 cases remained unspecified.
Among the 36 cases with both antifungal treatment and survival status available, the comparison of mortality rates across different antifungal treatment regimens revealed proportions of deaths as follows: 25% (4/16) for patients on amphotericin B, 40% (2/5) for patients with amphotericin B in combination with voriconazole, and 6.7% (1/15) for patients on voriconazole alone or in combination with itraconazole (p = 0.74).
In the group of 66 cases with both nephrectomy and survival status available, there was no significant difference in mortality rates between those who underwent nephrectomy (4/15, 26.7%) and those who did not (15/51, 29.4%) (p = 0.8).
For 57 cases of renal aspergillosis with antifungal, nephrectomy and mortality status stated, overall survival was 74%, and survival was relatively higher among cases treated with azole-based regimes with or without nephrectomy (85% and 100%), compared to those treated with amphotericin B – based regimens with or without nephrectomy (50% and 70%). However, the difference in mortality was not statistically significant (p = 0.49), and could reflect other advances in medicine, Figure 3.

Survival rates in renal aspergillosis stratified by antifungal therapy and nephrectomy status.
Discussion
Renal aspergillosis (nephromycosis aspergillina) was first described by Dr Ross in 1891. 88 Renal and genito-urinary aspergillosis are uncommon conditions, characterized by an unclear optimal treatment regimen and prognosis.29,41 This comprehensive systematic review offers valuable insights into various aspects of this relatively rare condition. Isolated renal cases constituted the majority (81.3%) of the cases included in this study, with diabetes mellitus, HIV, and hepatic cirrhosis emerging as the most significant underlying conditions. Most of these patients were immunocompromised and thus at high risk for invasive disease, mortality, and poor responsiveness to treatment. Therefore, clinicians should remain vigilant for early detection and consider tailored treatment approaches for individuals with these risk factors, given that clinical symptoms of renal and genitourinary aspergillosis, such as flank pain, fever, and lower urinary tract symptoms, are non-specific. Among patients with renal aspergillosis, mortality was unacceptably high at 28%. Further research is warranted to establish standardized treatment regimens and explore innovative therapeutic strategies to improve patient outcomes in this challenging clinical context.
We observed a distinct male predominance, with over 85% of the identified cases of renal aspergillosis being males. Whereas this association has not previously studied, we speculate that certain risk factors might be more prevalent among males, like occupational and behavioural exposures that make males more susceptible. As seen in this study, a higher proportion of men had diabetes mellitus, HIV/AIDS, and liver cirrhosis as the underlying comorbidities. Besides invasive candidiasis, this finding is consistent with previous studies of other invasive fungal infections, including pulmonary aspergillosis.26,89–91 Consequently, male sex has also been shown to be significantly associated with mortality, although this was not significant in our study. Besides underlying comorbidities and behavioural risk factors, there may exist the role of genetics and gender-specific immunological differences that may render males more susceptible, which necessitates further research studies into the mechanisms.
We found A. fumigatus as the most frequent Aspergillus species implicated in nearly 42.9% of all cases. Historically, A. fumigatus has been recognized as the primary pathogen in the Aspergillus genus, given its ability to thrive in a wide range of environmental conditions and its enhanced virulence factors. It is also the leading cause of invasive aspergillosis, including pulmonary aspergillosis. Its predominance in renal aspergillosis could be attributed to the mode of spread, which is believed to be primarily haematogenous. Renal and urinary tract aspergillosis is particularly concerning, as A. fumigatus infections often pose therapeutic challenges due to antifungal resistance and aggressive disease manifestation.92–94 While other species such as A. flavus and A. niger were also implicated in our study, the pronounced prevalence of A. fumigatus necessitates an increased focus on developing targeted diagnostic tools, therapeutic strategies, and public health measures for its effective management. Continued research into its pathogenicity, interactions with the human host, and resistance patterns will be pivotal for advancing our understanding and combating this pathogen.
Clinically apparent renal aspergillosis is a localized form of invasive aspergillosis, which particularly occurs in patients with systemic immunosuppression as seen in this review. If renal aspergillosis is a component of disseminated aspergillosis and is clinically silent, renal parenchymal disease can be treated effectively using modern antifungal therapy. However, if treatment of disseminated aspergillosis is successful, renal disease in this context does need to be addressed separately. Aspergillosis occurring in HIV/AIDS has recently been reviewed. 95 Histopathology, biomarkers, and medical imaging are key in the diagnosis of invasive aspergillosis. 96 In our review, we found that histopathology was the primary diagnostic method in over 70% of the cases.
Histopathology, biomarkers, and medical imaging are key in the diagnosis of invasive aspergillosis. 96 In our review, we found that histopathology was the primary diagnostic method in over 70% of the cases. The few reports of cases of renal aspergillosis in Africa, which has a high burden of risk factors for renal and invasive aspergillosis such as HIV, DM and increasing cancer burden is probably due to limited access and availability of diagnostics. In our recent diagnostic survey of access to World Health Organization-recommended essential diagnostics, we found that significant gaps exist in the accessibility of vital diagnostic tools for invasive fungal infections in Africa, specifically concerning Aspergillus antigen testing and contemporary medical imaging methods such as CT and MRI. 97 While concrete data on galactomannan (GM) in renal aspergillosis remains elusive, there is some insight when renal involvement is part of disseminated invasive aspergillosis. In such cases, a slightly elevated GM positivity rate compared to invasive pulmonary aspergillosis may be anticipated, contingent on factors like prophylaxis and neutropenia. 98 In isolated renal aspergillosis, the likelihood of serum positivity is expected to be minimal. However, there is potential for urinary GM to yield positive results. Notably, a novel urinary GM assay has shown promise, often yielding positive results due to vesicles present in the urine. 99
Managing renal and genitourinary aspergillosis presents significant challenges. Treating renal parenchymal disease necessitates systemic antifungal therapy, including options such as amphotericin B, systemic triazoles, or echinocandins, singly or in combination, although the effectiveness of these antifungal agents remains unproven. Co-administering flucytosine might be beneficial due to its substantial urinary excretion and synergistic effects with amphotericin B; 23 however, its activity is only demonstrable at acid pH, with uncertain implications for activity in the urine. 100
Expert opinion suggests a combination of medical and surgical approaches, involving topical and systemic antifungal agents, endourological procedures for cleansing and reducing mass, and potentially nephrectomy, depending on individual factors. Unfortunately, nephrectomy is often necessary, which is a less favourable option for patients with bilateral disease. We did not observe any difference in mortality rates for both patients on amphotericin B-based or triazole-based regimens, with or without nephrectomy. However, patients who received triazoles voriconazole, with nephrectomy had excellent survival. This is in line with current treatment guidelines that favour the use of voriconazole over amphotericin B for the management of invasive aspergillosis. All patients with prostatic aspergillosis in the review survived, and a combined medical and surgical strategy has been recommended.
The infectious diseases society of America guidelines for the treatment of aspergillosis propose a comprehensive approach, advocating both medical and urologic strategies for renal aspergillosis. 101 For ureteral obstruction, the recommendation is decompression if feasible, coupled with the local instillation of amphotericin B deoxycholate through a nephrostomy tube. For parenchymal disease, voriconazole is the preferred treatment. The guideline recommends medical management for smaller abscesses and surgical drainage for larger abscesses, with microwave ablation showing promise as a supplementary therapy in select cases where surgery is a less viable option. Nephrectomy is only recommended as a last resort when medical therapy has failed.
Strengths and limitations
The strength of our study lies in its comprehensive analysis of isolated renal and genito-urinary aspergillosis cases across diverse publications, contributing to a robust understanding of this rare condition. Moreover, to the best of our knowledge, this is the first systematic review to synthesize such comprehensive literature on genitourinary aspergillosis. However, the scarcity of available cases and the inherent limitations of case reports and case series may impact the generalizability of our findings. Furthermore, the potential for publication bias cannot be disregarded, as positive outcomes may be more likely to be reported. Due to the heterogeneity of the studies and the type of data available, no meta-analysis was performed. As a result, the study did not provide pooled effect sizes, which might limit the depth of the conclusions.
Implications
Our findings underscore the need for heightened clinical awareness among healthcare professionals, particularly in populations with established risk factors, such as diabetes mellitus, which could lead to earlier detection and intervention. The recognition of varying Aspergillus species emphasizes the importance of tailored treatment strategies based on local epidemiology. Additionally, our study highlights the need for further research to refine diagnostic protocols and optimize treatment approaches, especially considering the mortality rate and potential disparities in patient outcomes.
Conclusion
In summary, all-cause mortality in patients with renal aspergillosis was 28% and all patients with bladder, prostate or ureteric aspergillosis survived. DM, HIV, and other immunosuppressive conditions were common among these cases. While varied treatment strategies were observed, mortality rates showed no significant differences based on treatments or nephrectomy status. Further research is needed to refine diagnostics, optimize treatments, and enhance awareness among clinicians for early detection and management.