
Abstract
Background:
The ideal surgical approach for the management of varicocele in children and adolescents remains controversial. Several techniques are available including artery- or lymphatic-sparing with optical magnification (via open inguinal or sub-inguinal approach), laparoscopic, antegrade and retrograde embolization/sclerotherapy.
Objectives:
We aimed to appraise the clinical outcomes of these techniques in children and adolescents.
Data Sources and Methods:
A systematic review was conducted (1997–2023). Meta-analysis or proportional meta-analysis for non-comparative studies (Freeman-Tukey transformation) using the random effects model was conducted. Results are expressed as overall proportion % and 95% confidence interval (CI).
Results:
We identified 1910 studies; 632 duplicates were removed, 1278 were screened, 203 were reviewed and 56 were included, with 12 reporting on 2 different techniques (total of 68 data sets). Optical magnification via inguinal approach (498 cases): recurrence 2.5% (0.6–5.6), hydrocele 1.6% (0.47–3.4), testicular atrophy 1% (0.3–2.0), complications 1.1% (0.2–2.6); optical magnification via sub-inguinal approach (592 cases): recurrence 2.1% (0.7–4.4), hydrocele 1.26% (0.5–2.3), testicular atrophy 0.5% (0.1–1.3), complications 4% (1.0–8.8). Laparoscopic with mass-ligation/division (1943 cases): recurrence 2.9% (1.5–4.6), hydrocele 11.4% (8.3–14.9); complications 1.5% (0.6–2.9); laparoscopic with lymphatic-sparing (974 cases): recurrence 2.4% (1.5–3.5), hydrocele 1.2% (0.45–3.36), complications 1.2% (0.05–3.9); laparoscopic with artery-sparing (228 cases): recurrence 6.6% (2.3–12.9), hydrocele 6.5% (2.6–12.0). Antegrade embolization/sclerotherapy (403 cases): recurrence 7.6% (5.2–10.4), hydrocele 0.8% (0.17–1.9), technical failure 0.6% (0.1–1.6), complications 4.0% (2.3–6.1); retrograde embolization/sclerotherapy (509 cases): recurrence 6.9% (4.6–9.5), hydrocele 0.8% (0.05–2.5), technical failure 10.2% (4.6–17.6), and complications 4.8% (1.0–11.2).
Conclusion:
The recurrence rate varies between 2.1% and 7.6% and is higher with the embolization/sclerotherapy techniques. Post-operative hydrocele rate varies between 0.8% and 11.4% and is higher with the laparoscopic mass-ligation/division technique. Testicular atrophy has not been reported with the laparoscopic and embolization/sclerotherapy techniques. The retrograde embolization technique is associated with 10% technical failure (inability to complete the procedure). The laparoscopic lymphatic-sparing technique is characterized by the lowest recurrence rate, incidence of hydrocele and other complications, and no reports of testicular atrophy.
Keywords
Introduction
A varicocele is an abnormal dilation of the pampiniform plexus that occurs in 10–15% of the male population. 1 The clinical relevance of varicocele remains mostly unclear, with substantial individual differences in the clinical characteristics (e.g. grading), symptomatology (e.g. severity of pain) and impact on fertility. These variations are likely to account for the many inconsistencies surrounding the indications and optimal timing for intervention.
While infertility is generally considered an indication for intervention in the adult population, the indications for intervention in children and adolescents remain controversial. 2 Furthermore, the link with infertility is also questioned as, although varicocele is reported to be present in 30% of infertile couples, large population-based studies have documented that 85% of adults with varicocele are fertile. 3
In contrast, studies in the adult population have suggested that the effects of varicocele are progressive, resulting in testicular atrophy over time, proposing a role for intervention in the paediatric age. 4
It is therefore debatable if surgery performed at a young age could improve gonadal function, and increase fertility. However, utilization of semen specimens to identify and select patients ‘at risk’ for future infertility can be ethically and practically challenging, and often not feasible, in children and adolescents. Consequently, common indications for intervention in children and adolescents include significant testicular volume discrepancy (>15–20%), presence of pain or other symptoms (e.g. ‘dragging sensation’) and varicocele grade. 1
In addition to the uncertainty on the impact on future fertility, there are several controversies regarding the optimal surgical treatment in children and adolescents; these include the choice of the operative technique, the risk/benefit ratio of ligating the internal spermatic artery (leading to possible testicular atrophy) and the risk of post-operative hydrocele formation.
Although surgery for varicocele can be dated back as far as the first century A.D., it gained popularity with the introduction of the Ivanissevich (suprainguinal) and Palomo (retroperitoneal) varicocelectomy procedures, described, respectively, in 1918 and 1949.5–7 Since their original description, these techniques have undergone several modifications including the introduction of optical magnification and more recently laparoscopy.1,5 In addition, Lima et al. in 1978 introduced the injection of a sclerotizing substance through a cannula into a refluxing vein (antegrade embolization/sclerotherapy) which was subsequently popularized by Tauber et al. in 1988.8,9 Iaccarino in 1977 described a radiologically guided technique with the injection of a sclerosing agent in the spermatic vein via a retrograde approach after percutaneous catheterization of the femoral vein. 10
At present, several treatment options are available but ultimately, the choice of technique for varicocele surgery remains subjective, determined by the surgeon’s preference and prior experience. As discussed above, the long-term effects on fertility remain uncertain. In the short term, the ideal procedure should be characterized by a low rate of recurrence, hydrocele formation, testicular atrophy and other complications (e.g. wound infection) and lead to the resolution of symptoms such as pain. We conducted a systematic review and meta-analysis on the most widely utilized surgical approaches in children and adolescents including the inguinal and sub-inguinal artery- and lymphatic-sparing with optical magnification technique, the laparoscopic techniques and the antegrade and retrograde embolization/sclerotherapy techniques.
We focused on the incidence of persistent/recurrent varicocele, post-operative hydrocele formation, post-operative testicular atrophy, other complications and technical failure as endpoints of clinical significance.
Methods
Protocol and registration
We performed a systematic review and meta-analysis evaluating the outcome following surgical and radiological treatment of varicocele in patients up to 20 years of age. The study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2015. 11 We collected and analysed the following post-operative outcomes: recurrence, hydrocele formation, testicular atrophy, other complications (e.g. oedema, wound infection, hematoma formation, pain) and technical failure (defined as the need to abandon the procedure and/or the need for conversion to a different procedure). Collected data were recorded in a database spreadsheet (Microsoft® Excel for Mac version 15.41; Microsoft Corporation, Washington, USA; 2017).
Systematic review
An electronic database search was conducted to identify studies published between 1987 and 2023 evaluating outcomes following surgical or radiological management of primary varicoceles in children and adolescents (⩽20 years of age). The Ovid MEDLINE, PubMed, The Cochrane Library and ScienceDirect databases were searched independently by three investigators (ST, DB and MP) between January and February 2023. Search terms utilized were ‘varicocele’, ‘management’, ‘treatment’, ‘child’ and ‘adolescent’. Only articles in the English language were included. Randomized controlled trials (RCT), cohort studies, case–control studies and prospective and retrospective case series were considered for inclusion. Studies containing less than 20 patients in the therapeutic group, case reports, abstracts only, review articles, letters to the editor and comments were excluded. We also excluded studies with patients of ⩽20 years of age who had undergone previous inguinal surgery and/or patients with recurrent varicoceles. Evaluated treatment modalities included: microsurgical varicocelectomy using loupe or microscope magnification via inguinal and sub-inguinal incision, laparoscopic ligation/division (Palomo ‘en-bloc’ ligation/division, artery- and/or lymphatic-sparing), and radiologically guided antegrade and retrograde/sclerotherapy. When separate articles reporting on overlapping populations were identified, the most recent article with the largest study population was selected for review. A full-text copy of each article was obtained for detailed review. References within the included articles were also screened to identify additional relevant articles. The full text of the potentially eligible studies was obtained and independently assessed for eligibility by ST, DB and MP. Any disagreement over the eligibility of studies was resolved through discussion with the fourth author (RMN).
Meta-analysis
Statistical analysis was conducted with MedCalc® Statistical Software version 20.218 (MedCalc Software Ltd, Ostend, Belgium; https://www.medcalc.org; 2023). Meta-analysis was conducted for randomized controlled trials and comparative studies; to account for heterogeneity between studies, we used the random-effect model to produce relative risk (RR) for categorical variables along with 95% confidence intervals (CIs). Proportional meta-analysis with Freeman-Tukey transformation (arcsine square root transformation) and random effect was used to calculate an overall proportion (%) with (95% CI) from non-comparative studies. I2 value was used to assess heterogeneity; I2 > 50% was considered to be substantial heterogeneity. Studies having no events in both arms were excluded from the statistical analysis according to the Cochrane Handbook for Systematic Reviews of Interventions. 12 The Egger’s regression test was used to assess publication biases. p Values < 0.05 were considered significant.
Quality assessment
The Cochrane Collaboration’s tool for assessing the risk of bias in RCTs was used to assess the quality of all RCTs that met our inclusion criteria. 13 The Newcastle–Ottawa Scale for assessing the quality of non-randomized studies in meta-analyses was used to assess the quality of all case–control and case-series studies. 14 The Assessment of Multiple Systematic Reviews tool was used by the two senior authors (RMN and MP) to independently assess the methodological quality of this systematic review. 15
Results
We identified 1910 studies: 632 were duplicates and removed, 1278 were screened and 203 were reviewed in full text. A total of 56 studies were included in the final analysis with 12 studies reporting on 2 different techniques for a total of 68 data sets (Figure 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram. 16
The number of data sets for the different techniques included the following: inguinal microsurgical with artery- and lymphatic-sparing (n = 8)17–24; subinguinal microsurgical with artery- and lymphatic-sparing (n = 11)21,22,25–33; laparoscopic mass-ligation/division (n = 23)20,26,34–54; laparoscopic lymphatic-sparing (n = 8)32,35,39,50,55–58; laparoscopic artery-sparing (n = 5),38,53,59–61 antegrade embolization/sclerotherapy (n = 7)36,54,62–66; and retrograde embolization/sclerotherapy (n = 6).67–72
Inguinal and subinguinal artery- and lymphatic-sparing with optical magnification (microsurgical)
We identified a total of 19 data sets (17 studies) on the artery- and lymphatic-sparing techniques with optical magnification (Tables 1 and 2).17–33 Five studies reported on the inguinal approach alone17–19,23,24 and seven on the subinguinal approach alone.25,27–31,33 Two studies compared the two techniques.21,22 One study compared the laparoscopic mass-ligation/division technique to the inguinal artery- and lymphatic-sparing technique, 20 one study compared the laparoscopic lymphatic-sparing technique to the subinguinal artery- and lymphatic-sparing technique, 32 and one study compared the laparoscopic mass-ligation/division technique to the subinguinal artery- and lymphatic-sparing technique. 26 There were two RCTs,21,24 and two prospective studies.25,28 The remaining studies were retrospective. The results of the meta-analysis of proportions for non-comparative studies are summarized in Table 3. Meta-analysis was not feasible due to the lack of minimal data sets for randomized controlled trials and comparative studies.
Systematic review for inguinal artery- and lymphatic-sparing with optical magnification.

N/A, not available; ±SD, standard deviation.
Systematic review for subinguinal artery- and lymphatic-sparing with optical magnification.

N/A, not available; ±SD, standard deviation.
Meta-analysis of proportions of non-comparative studies for inguinal and subinguinal artery- and lymphatic-sparing with optical magnification.

Laparoscopic techniques
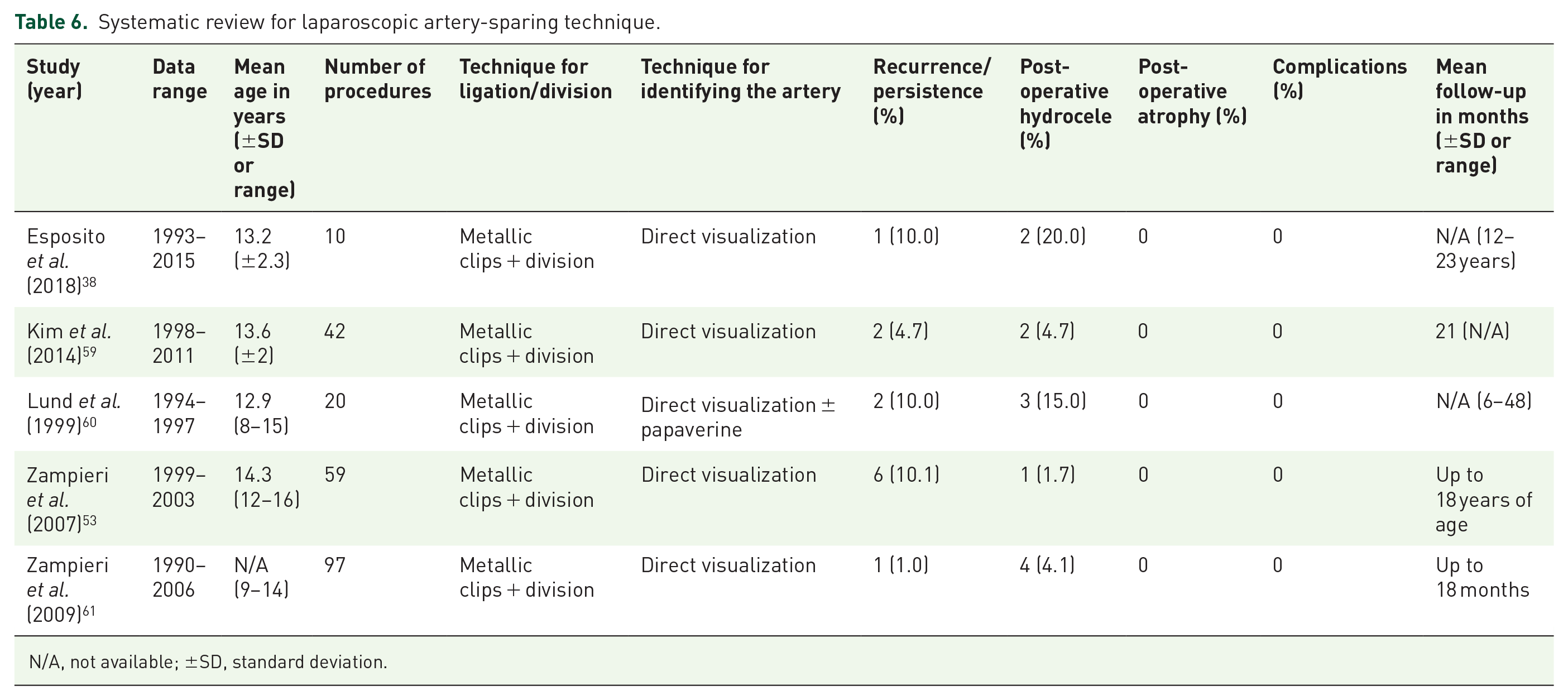
We identified a total of 36 data sets (31 studies) on 3 different types of laparoscopic techniques (Tables 4–6).20,26,32,34–61 A total of 14 studies reported on laparoscopic mass-ligation/division alone34,37,40–49,51,52; 4 studies reported on laparoscopic lymphatic-sparing alone55–58 and 3 studies reported on laparoscopic artery-sparing alone.59–61 Three studies compared laparoscopic mass-ligation/division to laparoscopic lymphatic-sparing techniques,35,39,50 two studies compared laparoscopic mass-ligation/division to laparoscopic artery-sparing techniques.38,53 Two study compared the laparoscopic mass-ligation/division technique to the antegrade embolization/sclerotherapy technique36,54; one study compared the laparoscopic mass-ligation/division technique to the inguinal artery- and lymphatic-sparing with optical magnification technique, 20 one study compared the laparoscopic mass-ligation/division technique to the subinguinal artery- and lymphatic-sparing with optical magnification technique, 26 and one study compared the laparoscopic lymphatic-sparing technique to the subinguinal artery- and lymphatic-sparing with optical magnification technique. 32 There were three RCTs,36,39,57 two prospective studies.51,53 The remaining studies were retrospective. The results of the meta-analysis of proportions for non-comparative studies are summarized in Table 7. We did not identify any reported case of testicular atrophy for any of the laparoscopic techniques.
Systematic review for laparoscopic mass-ligation technique.

N/A, not available; ±SD, standard deviation.
Systematic review for laparoscopic lymphatic-sparing technique.

N/A, not available; ±SD, standard deviation.
Systematic review for laparoscopic artery-sparing technique.
N/A, not available; ±SD, standard deviation.
Meta-analysis of proportions of non-comparative studies for laparoscopic techniques.

Meta-analysis of the three comparative studies for the laparoscopic mass-ligation/division and laparoscopic lymphatic-sparing techniques revealed similar recurrence rate [RR 1.4 (0.6–3.5), p = 0.43; I2 = 0.0% (0.0–0.0), p = 0.7] but significant lower incidence of post-operative hydrocele in the lymphatic-sparing group [RR 8.5 (1.3–55.2), p = 0.02; I2 = 53.2% (0.0–86.6), p = 0.1]; Egger’s test revealed significant publication bias for the recurrence rate (p < 0.0001) but not for the hydrocele (p = 0.3).
Meta-analysis of the two comparative studies for the laparoscopic mass-ligation/division and laparoscopic artery-sparing techniques revealed a high recurrence rate [RR 0.1 (0.02–0.5), p = 0.008; I2 = 0.0% (0.0–0.0), p = 0.7] for the artery-sparing technique and similar incidence of post-operative hydrocele [RR 1.4 (0.05–47.7), p = 0.8; I2 = 87.8% (53.0–96.8), p = 0.004]; Egger’s test revealed significant publication bias for both recurrence and hydrocele rate (p < 0.0001).
Antegrade and retrograde embolization/sclerotherapy
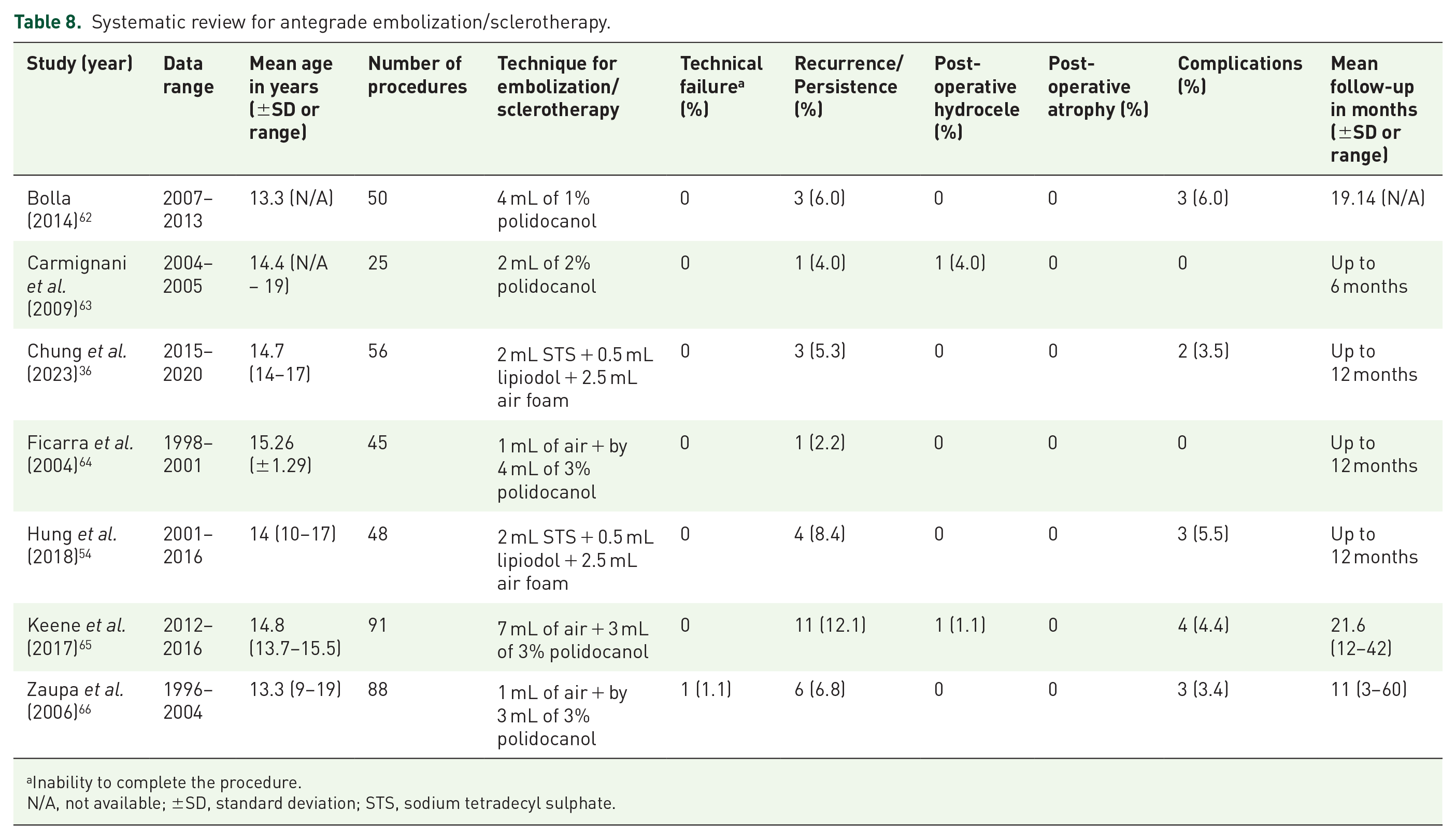
We identified a total of 13 data sets (13 studies) evaluating antegrade and retrograde embolization/sclerotherapy (Tables 8 and 9).36,54,62–72 There was one RCT, 36 and six prospective studies.62–66,72 The remaining studies were retrospective. The results of the meta-analysis of proportions for non-comparative studies are summarized in Table 10. Meta-analysis was not feasible due to the lack of minimal data sets for randomized controlled trials and comparative studies. We did not identify any cases of testicular atrophy for both techniques.
Systematic review for antegrade embolization/sclerotherapy.
Inability to complete the procedure.
N/A, not available; ±SD, standard deviation; STS, sodium tetradecyl sulphate.
Systematic review for retrograde embolization/sclerotherapy.

Inability to complete the procedure.
N/A, not available; ±SD, standard deviation; STS, sodium tetradecyl sulphate.
Meta-analysis of proportions of non-comparative studies for embolization/sclerotherapy techniques.

Discussion
Since the original description of the Ivanissevich and Palomo procedures, there have been several new techniques described for the management of varicocele, both in the adult and paediatric populations.5–7 Due to the controversies over the optimal technique for the treatment of varicocele, we conducted a systematic review and meta-analysis on the outcome following surgical and radiological management in children and adolescents. We investigated the peri-operative and short-term outcomes including the persistence/recurrence of the varicocele, hydrocele formation, testicular atrophy, overall complications and technical failure. We focused our attention on the most widely utilized surgical approaches in children and adolescents including the inguinal and subinguinal artery- and lymphatic-sparing with optical magnification technique, the laparoscopic techniques and the antegrade and retrograde embolization/sclerotherapy techniques.
Overall, we found a lack of high-quality evidence regarding the use of any of these techniques with the majority of studies being retrospective with only 5 RCTs out of the 56 studies analysed.21,24,36,39,57
In summary, we found that the overall recurrence rate for the various procedures varies between 2.1% and 7.6%; this is higher with the embolization/sclerotherapy techniques. Additionally, the retrograde embolization technique is associated with 10% technical failure.
Post-operative hydrocele rate varies between 0.8% and 11.4% and is higher with the laparoscopic mass-ligation/division technique. We will discuss the outcomes for the various techniques separately.
Inguinal and sub-inguinal artery- and lymphatic-sparing surgery with optical magnification (microsurgical)
We found a lack of high-quality evidence regarding the use of inguinal and sub-inguinal artery- and lymphatic-sparing surgery with optical magnification. Despite significant heterogeneity among the studies, the recurrence rate appears to be similar with the two techniques, as does the incidence of post-operative hydrocele. We identified only one RCT directly comparing the two techniques which did not report significant differences in the post-operative outcomes, although the inguinal approach appeared to have a shorter operative time (25.5 versus 33.3 min, respectively, p < 0.01). 21
Optical magnification, using loupes or the surgical microscope, allows careful ligation of all internal and external spermatic veins, while sparing the arterial and lymphatic vessels. This aims to reduce the incidence of testicular atrophy and hydrocele formation; indeed, we found a low rate of these two complications, similar to what has been reported in their adult literature. 21 Due to the limited number of publications that we identified during the 36-year period (i.e. 17 publications compared to 31 for the laparoscopic techniques), it would appear that these techniques have not gained wide popularity among paediatric surgeons and paediatric urologists compared to the adult counterpart; this is also confirmed by one survey reporting that only 30% of paediatric urologists opted to use a microscope, likely due to lack of familiarity with the instrument.73,74 Nonetheless, Hsieh et al. 75 argued that loupe magnification is sufficient for reliable identification of the testicular artery or lymphatic vessels and their smaller branches.
We identified a relatively low post-operative complication rate variable between 1.1% and 4% although Choi et al, 25 in their prospective study, reported an overall rate of 20%, which mostly included post-operative pain and oedema. Considering that the majority of the studies we identified are retrospective in nature, it is likely that the overall complication rate might be underreported.
Finally, it must be noted that one of the possible advantages of the subinguinal technique in adults is the possibility to perform it under local anaesthesia; however, this is seldom the case in children and adolescents.
In summary, although the inguinal and sub-inguinal artery- and lymphatic-sparing surgery with optical magnification might be technically challenging, they seem to be associated with a low recurrence rate (up to 2.5%), low rate of hydrocele formation (up to 1.6%), low rate if testicular atrophy (up 1%) and other complications (up to 4%.) There is a need for high-quality evidence research with large randomized controlled trials to draw definitive conclusions regarding the outcome of the inguinal and sub-inguinal artery- and lymphatic-sparing surgery with optical magnification.
Laparoscopic techniques
The laparoscopic transperitoneal varicocelectomy procedure was introduced in the late 1980s by Sánchez de Badajoz et al. and has since gained popularity due to being safe, quick and relatively of simple execution.39,40,76 However, the issues of preservation of the internal spermatic artery and lymphatic vessels are the subject of considerable controversy. We found a lack of high-quality evidence regarding the use of laparoscopy for the management of varicocele in children and adolescents with only three RCTs36,39,57 and two prospective studies.51,53 The remaining studies were retrospective. The majority of studies (73%−22/30) were focused on the mass-ligation/division either alone or compared to other techniques.
The proportional meta-analysis identified an overall recurrence rate similar to the inguinal and sub-inguinal artery- and lymphatic-sparing with optical magnification technique for the mass-ligation/division (2.9%) and the lymphatic-sparing technique (2.4%); however, for the artery-sparing technique, the recurrence rate is more than double (6.6%). The meta-analysis of the three comparative studies for the laparoscopic mass-ligation/division and laparoscopic lymphatic-sparing techniques also revealed a similar recurrence. The meta-analysis of the two comparative studies for the laparoscopic mass-ligation/division and laparoscopic artery-sparing techniques also revealed a high recurrence rate for the latter (p = 0.008). Therefore, the artery-sparing technique has the highest recurrence rate among the three techniques. The artery-sparing technique is based on the direct visualization with the telescope and it is possible that during the dissection of the artery from the internal spermatic vein some refluxing collaterals may inevitably be left behind. 34
The most common complication of the mass-ligation/division technique, both laparoscopic and open, is post-operative hydrocele, as a result of the interruption of the lymphatic vessels, with reports in the literature showing an incidence variable from 5% to 39%. 77
Our systematic review revealed an overall hydrocele incidence of 11.4% for the mass-ligation/division technique and, as expected, a very low incidence (1.1%) for the lymphatic-sparing technique; the incidence for the artery-sparing technique was between the other two techniques (6.5%).
The lymphatic-sparing technique is normally performed using a dye (Table 5) to identify the lymphatic vessels, allowing their careful dissection from the artery and internal spermatic vein and collaterals. 37 Hence, with the artery-sparing technique, it is possible that during the dissection of the artery, some lymphatic vessels will be damaged since no dye is used. To identify the lymphatics with a dye, there are three possible modalities of injection: subdartoic since the lymphatic vessels drain mostly to inguinal nodes, it requires the injection of dye well in advance of surgery and could also possibly lead to persistent blue discoloration of the scrotum; intravaginal, the injection is performed between the two layers of tunica vaginalis which might be particularly challenging to achieve; intraparenchymal, the injection is within the body of the testis which is fast and provides the best visualization of the lymphatic vessels. It must be noted that the use of intra-testicular dye for lymphography causes pathological changes in testicular histology in rats, although the long-term effects of these chances are not documented, and might not be relevant to the humans subjects. 78 Furthermore, the subdartoic injection of methylene blue can cause skin and fat necrosis and some authors advocate the use of patent blue dye V. 39
We did not document any cases of testicular atrophy, even with the mass-ligation/division technique. A possible explanation is that the vessels are ligated high in the retroperitoneum, allowing for distal blood supply. Consequently, some authors recommend to section the vessels 3–4 cm proximal to the internal inguinal ring to spare the collateral vascularization. 38
We found a <2% rate of other complications for the various laparoscopic techniques confirming that this approach is safe.
Finally, regarding the modality for ligation/division of the vessels, the majority of the authors report the use of clips followed by division with scissors (Tables 4–6). A few authors report the use of the LigaSure™ (Table 4) arguing that, although the device has a high cost, it is safe, easy and fast to use, leading to potential cost savings. 44 However, there are no studies comparing these different techniques in children and adolescents.
Antegrade and retrograde embolization/sclerotherapy
The injection of sclerosing agents in the spermatic vein to treat varicocele was initially introduced by Lima et al. in 1978 (antegrade approach) and popularized by Tauber et al. in 1988.8,9 Iaccarino in 1977 described a radiologically guided technique with injection of a sclerosing agent in the spermatic vein with a retrograde approach via the femoral vein. 10 Overall we only identified 13 studies which is a relatively small number compared to the other techniques; inguinal and sub-inguinal artery- and lymphatic-sparing with optical magnification techniques (17 studies), laparoscopic approach (31 studies). Therefore, we confirm previous observations that the utilization of embolization/sclerotherapy is not widespread among paediatric surgeons and paediatric urologists. 64 We found a lack of high-quality evidence regarding the of use these techniques with significant heterogeneity among the studies.
The aim of these techniques is to obtain a selective obliteration of the venous system while preserving the arterial and lymphatic vessels, to avoid post-operative hydrocele and testicular atrophy.
The proportion meta-analysis identified an overall recurrence rate of 7.6% for the antegrade technique and 6.9% for the retrograde technique. These recurrence rates are higher than the inguinal and sub-inguinal artery- and lymphatic-sparing surgery with optical magnification techniques (2.1% and 2.5%, respectively) and the laparoscopic mass-ligation/division and lymphatic-sparing techniques (2.4% and 2.9%, respectively). However, for the laparoscopic artery-sparing technique, the recurrence rate is similar (6.6%). From our systematic review, the reasons behind the higher recurrence rate with the embolization/sclerosing techniques are not entirely clear. Several devices and/or substances have been described for both techniques (Tables 8 and 9), but there are no studies that have compared the recurrence rates based on different methods.
Our meta-analysis documented a low incidence of hydrocele for both techniques, this is not surprising since the lymphatic vessels are spared with both procedures. Nonetheless, both techniques are predisposed to a relatively higher rate of other peri-operative complications (4.0% for the antegrade and 4.8% for the retrograde procedure) compared to other techniques that we analysed (Tables 3, 7 and 10). Common reported peri-operative complications for the antegrade approach include hematoma of the spermatic cord, wound infection and scrotal hematoma.36,54,62,65,66 Indeed, Hung et al. recommended that, for patients with anomalous drainage, the antegrade sclerotherapy should not proceed, as the incorrect cannulation of spermatic cord superficial veins could lead to significant complications because of occlusion of veins in other districts. 54 Complications for the retrograde approach include pampiniform plexus thrombophlebitis, groin hematoma and interval spermatic vein perforation with spillage of contrast.67,68,70,72
Technical failure (defined as the inability to complete the procedure and/or the need for conversion to a different procedure) is also an issue with embolization/sclerosing techniques, particularly with the retrograde approach. Pieri et al. reported that in a series of 1490 varicoceles the percutaneous retrograde sclerotherapy via the basilic vein was successful in only 79.2% of cases because in the remaining patients, there was a venous spasm during the introduction of the cannula, particularly in children. 79 We found an overall rate of technical failure of 10.2% with the retrograde technique, often due to difficult cannulation of the internal spermatic vein via the femoral vein in 10–20% of patients.67,68
Finally, it must be noted that both the antegrade and retrograde techniques expose patients to radiation (including the testicles). The latter technique especially can be characterized by a long operative time (up to 90 min for unilateral cases and 120 min for bilateral cases) and X-ray screening time of up to 3.5 min, subjecting children and adolescents to a significant radiation burden of nearly 14 times more than an abdominal radiography.66,70
Limitations
All of the included studies in our systematic review and meta-analysis grouped together populations of patients with a wide age range; from pre-pubertal 7-year-old children to post-pubertal 20-year-old young adults. However, it was not possible to break down the results based on age groups and techniques, which may account for some of the differences in outcomes that we identified.
For the meta-analysis, we used the random-effect model to mitigate differences in characteristics, such as age range and surgeon; nonetheless, we documented variable heterogeneity between studies and significant publication biases.
The cost–benefit is an important aspect to consider in choosing the technique; however, we did not find any study that directly compared the costs of different techniques and the costs related to the complications. In addition, most papers did not provide data regarding the modality of hospital admission (i.e. day surgery versus overnight stay). For these reasons, and considering the significant heterogeneity of techniques and healthcare settings, it is not possible to draw conclusions regarding the cost–benefit of each technique in children and adolescents.
Finally, we acknowledge that there are a number of novel techniques, such as single-port varicocelectomy, indocyanine-guided varicocelectomy or robotic-assisted laparoscopic varicocelectomy, that are more established in adults, but the scientific evidence for these techniques in children and adolescents is limited to small series.80–82
Conclusion
In conclusion, there is a lack of high-quality evidence regarding the outcome following surgery for varicocele in children and adolescents with any of the common techniques currently utilized.
The recurrence rate varies between 2.1% and 7.6% and is higher with the embolization/sclerotherapy techniques. Post-operative hydrocele rate varies between 0.8% and 11.4% and is higher with the laparoscopic mass-ligation/division technique. Testicular atrophy has not been reported with the laparoscopic and embolization/sclerotherapy techniques. The retrograde embolization technique is associated with 10% technical failure.
Based on the current evidence, the laparoscopic techniques appear to be of easy execution, with no cases of technical failure or testicular atrophy reported in the literature. The laparoscopic lymphatic-sparing technique offers the lowest recurrence rate and lowest incidence of hydrocele and other complications. Large prospective trials are needed to draw definitive conclusions regarding the best technique for the surgical management of varicocele in children and adolescents.