
Abstract
Urosepsis is sepsis caused by urogenital tract infection and is one of the most common critical illnesses in urology. If urosepsis is not diagnosed early, it can rapidly progress and worsen, leading to increased mortality. In recent years, with the increase of urinary tract surgery, the incidence of urosepsis continues to rise, posing a serious threat to patients. Early diagnosis of urosepsis, timely and effective treatment can greatly reduce the mortality of patients. Biomarkers such as WBC, NLR, PCT, IL-6, CRP, lactate, and LncRNA all play specific roles in the early diagnosis or prognosis of urosepsis. In addition to the abnormal increase of WBC, we should be more alert to the rapid decline of WBC. NLR values were superior to WBC counts alone in predicting infection severity. Compared with several other biomarkers, PCT values can differentiate between bacterial and non-bacterial sepsis. IL-6 always has high sensitivity and specificity for the diagnosis of sepsis, and CRP also has high sensitivity and specificity for the diagnosis of urosepsis. Lactic acid is closely related to the prognosis of patients with urosepsis. LncRNAs may be potential biomarkers of urosepsis. This article summarizes the main biomarkers, hoping to provide a reference for the timely diagnosis and evaluation of urosepsis.
Introduction
Urosepsis is sepsis caused by infection of the urogenital tract. In the past, clinical symptoms of urinary tract infection and systemic inflammatory response syndrome (SIRS) were diagnosed as urosepsis. In 2016, the Society for Critical Care Medicine (SCCM) and the European Society for Critical Care Medicine (ESICM) revised the definition and diagnostic criteria for sepsis, defining sepsis as infection with life-threatening organ dysfunction due to impaired host response. The Sequential Organ Failure Assessment (SOFA) score was used to assess organ dysfunction (when SOFA score ⩾2, sepsis = infection + SOFA score, Table 1). 1
The Sequential Organ Failure Assessment (SOFA) score.
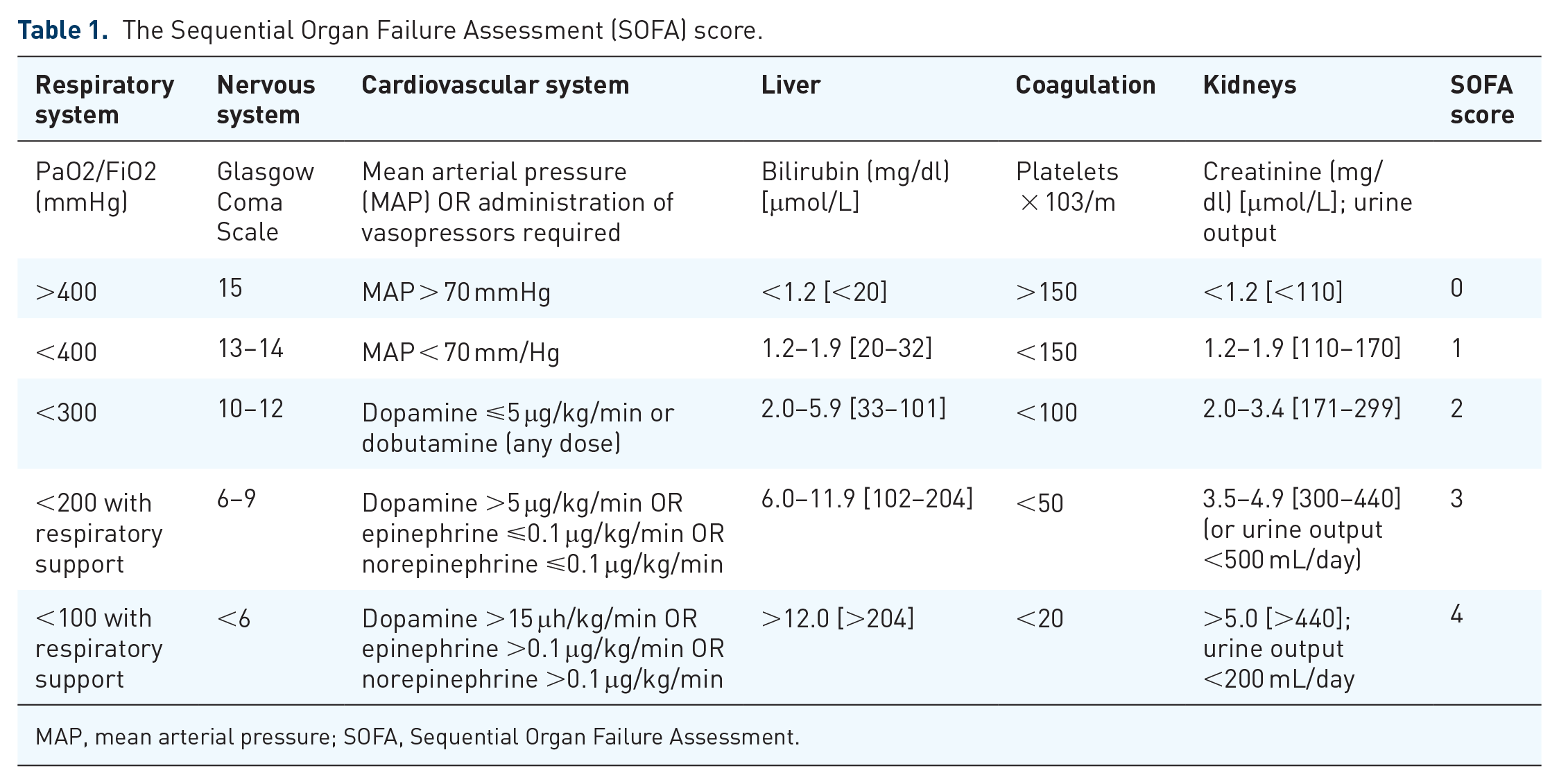
MAP, mean arterial pressure; SOFA, Sequential Organ Failure Assessment.
Therefore, the definition of urosepsis can be simultaneously updated to refer to life-threatening multiple organ dysfunction caused by a dysregulated body response to infections originating from the urinary system. According to the epidemiological survey in the United States, the incidence of sepsis is increasing year by year, with an annual growth rate of about 8.7%, of which urosepsis accounts for about 8.6–30.6%, and the mortality rate reaches 20–40%. 2 High mortality is not only related to disease severity but also to early diagnosis and effective treatment of the disease. Early detection of risk factors before surgery can help doctors to take measures to prevent the occurrence of urosepsis, and timely detection of sepsis after surgery can help doctors to quickly carry out appropriate treatment and reduce the morbidity and mortality of sepsis.
Urosepsis is often accompanied by abnormal levels of various infectious biomarkers, 3 providing strong evidence for the diagnosis of urosepsis, including white blood cells (WBCs), procalcitonin (PCT), C-reactive protein (CRP), interleukin (IL)-6, pathogen culture, and other biomarkers. Positive blood cultures are the gold standard for diagnosing sepsis, but pathogen culture and identification are time-consuming compared to rapid biomarker results. Sepsis-related scoring systems such as the SOFA score and the Acute Physiology and Chronic Health Evaluation II (APACHE II) score can determine the severity of urosepsis and predict patient mortality. 4 However, there are many evaluation indicators and the evaluation process is complicated, and its application in general wards is difficult to promote. Therefore, changes in relevant biomarkers that enable rapid results are playing an increasingly important role in diagnosing urosepsis (Table 2). This article summarizes the use of the following biomarkers in urosepsis.
Role of biomarkers in urosepsis.

CRP, C-reactive protein; NLR, neutrophil to lymphocyte ratio; PCT, predictive comparisons of procalcitonin; SOFA, Sequential Organ Failure Assessment; WBC, white blood cell. All samples can be obtained from serum.
WBC
WBC count is a commonly used clinical indicator of acute inflammation. In addition, the surgery itself causes a physiological increase in WBC. Goel et al. 32 found that the WBC count increased on the first postoperative day and gradually returned to normal from the fourth day. Other studies have found that symptoms of fever and leukocytosis are more common in infected patients, but only after the sixth postoperative day. 33 Bozkurt et al. 5 showed that postoperative WBC count (>14.05 × 109/L) or the absolute difference between postoperative and preoperative WBC count (>5.25 × 109/L) was significantly associated with the occurrence of sepsis after percutaneous nephrolithotomy (PCNL). This indicates that for patients with urinary tract infection, blood WBC count greater than 14 × 109/L can be used as an early warning factor for urosepsis. But in urosepsis, the WBC count is actually lower than normal. This is because severe sepsis consumes large amounts of WBC, platelets (PLTs), and fibrinogen when severe infection occurs, resulting in a decrease in WBC and PLT. 34
A study of urological lithotripsy found a sharp drop in blood WBC counts within the first 2 h of urosepsis shock. The threshold of WBC counts 2 h before urosepsis shock was 2.85 × 109/L, and the sensitivity and specificity for predicting urosepsis shock were 95.9% and 92.7%, respectively. This may be a good predictor of urosepsis shock in patients undergoing intracorporeal lithotripsy. WBC count should be measured within 2 h after intracorporeal lithotripsy for patients with high-risk factors of urosepsis, such as female, advanced age (age ⩾ 65 years), renal insufficiency (creatinine ⩾ 248 mmol/L), positive preoperative urine culture, and elevated CRP.6–9
The application of blood WBC count in the diagnosis of urosepsis should pay attention to the abnormal increase of blood WBC count and the absolute difference between postoperative and preoperative. In patients with urinary tract infections, the likelihood of urosepsis should be increased if the postoperative WBC count is abnormally elevated or sharply decreased compared to preoperative WBC levels.
Neutrophil to lymphocyte ratio
Neutrophils and lymphocytes are important components of the immune system and initially resist inflammatory invasion during the body’s inflammatory response. When sepsis occurs, peripheral blood neutrophil counts are markedly increased due to the adhesion between neutrophils and endothelial cells and the delay in normal neutrophil apoptosis.35,36 Apoptosis and reduction of lymphocytes are the result of sepsis-induced immunosuppression. 37 Neutrophil to lymphocyte ratio (NLR) is the ratio of neutrophils to lymphocytes in peripheral blood, and Zahorec 38 was the first to propose the use of NLR as an additional marker of infection in clinical practice. Compared with more expensive tests such as PCT, NLR is a simple and effective predictor of infection severity, outperforming traditional laboratory tests such as blood WBC count, neutrophil count, and CRP.39,40 Furthermore, NLR is a better predictor of sepsis than platelet-to-lymphocyte ratio (PLR). 41 Using preoperative NLR to predict the occurrence of sepsis after PCNL, Sen et al. 10 found that the incidence of postoperative urosepsis was significantly increased when the preoperative NLR was >2.5. NLR < 5 can be used as a cut-off value for the differential diagnosis of infection and sepsis. When NLR > 5, the accuracy of sepsis diagnosis is similar to that of PCT, and when the elevated NLR level in patients with sepsis returns to normal or lower than normal, it may mean that the sepsis disappears or the patient’s condition improves. 11 A retrospective study by Loonen showed that NLR has some value in predicting a positive blood culture. 42 Another retrospective study involving 664 patients showed NLR values of 10.8–38.2 and 6.2–14.5 in septic and non-septic patients, respectively. 43 These all indicate that NLR value can be used as an effective predictor or diagnostic indicator of urosepsis, which is better than pure blood WBC count and neutrophil count to a certain extent.
IL-6
Il-6 consists of 212 amino acids and is a pleiotropic cytokine synthesized by T lymphocytes, fibroblasts, endothelial cells, and monocytes. 12 It has a wide range of biological activities in immune regulation, hematopoiesis, inflammation, and tumorigenesis, and is an important cytokine in the acute phase of inflammatory and septic responses.44,45 IL-6, PCT, WBC, and neutrophils have different diagnostic abilities for postoperative urosepsis at different time points, and IL-6 can be used as a biomarker for prediction and early diagnosis of urosepsis at 2 h and 1 day after PCNL. 13 In PCNL patients, peak IL-6 levels may be 1000–10,000 times the preoperative level in the presence of urosepsis and 10–100 times the preoperative level in the absence of urosepsis. 13
The normal serum IL-6 concentration is <5 pg/mL, and the serum IL-6 level increases within 1 h after infection stimulation, and peaks rapidly within 2 h. 46 Previous studies have shown that IL-6 is the most effective inflammatory marker for diagnosing urosepsis 2 h after surgery. 13 From infection to sepsis, IL-6 is first produced, and as the disease progresses, IL-6 levels increase, usually >500 pg/mL.45,47,48 This suggests that levels of IL-6 increase in proportion to the severity of the infection. In addition, elevated IL-6 often precedes PCT,49,50 CRP, and fever. 51 IL-6 has high sensitivity and specificity in differentiating sepsis, regardless of age and gender. This means that IL-6 can be used as a diagnostic marker for sepsis 52 to differentiate sepsis from infection at an early stage. In the early stage of urosepsis, the diagnostic value of IL-6 and PCT is similar and better than that of CRP. 12 Compared with PCT, the advantage of IL-6 is that it can be used to identify early acute infection and provide early warning of possible sepsis. In addition, compared with PCT, serum IL-6 can better distinguish sepsis from septic shock and has higher prognostic value than PCT, and the 28-day mortality of the high IL-6 group (IL-6 ⩾ 348.92 pg/mL) was significantly higher than that of the low IL-6 group (IL-6 <348.92 pg/mL). 53 IL-6 has important value in the prediction and early diagnosis of urosepsis, and has good clinical effect. In clinical practice, the advantages of IL-6 and PCT should be fully combined to improve the timeliness and accuracy of sepsis diagnosis and guide more rapid and effective treatment.
PCT
PCT is the propeptide of calcitonin, a glycoprotein composed of 116 amino acids, with a relative molecular weight of about 13 × 103. Under normal conditions, serum PCT values are <0.1 ng/mL, but in patients with sepsis, cells of parenchymal organs, including hepatocytes, kidney cells, adipocytes, and muscle cells, under the action of inflammatory cytokines, produce a large amount of PCT which are released into the blood, which significantly increases the serum PCT level and is positively correlated with the changes in the disease. 14 Unlike CRP and other acute-phase reactants, available data suggest that PCT levels are rarely increased by viral infection, suggesting that PCT may be useful in distinguishing bacterial and viral infections. 15 Patients with bacterial sepsis have significantly higher PCT levels than non-septic patients,54,55 and in bacterial infections, circulating PCT levels increase thousands of times. 14
Serum PCT concentrations were barely detectable at 0, 1, and 2 h post-infection (p < 10 pg/mL), detected at 4 h, peaked at 6 h, and plateaued at 8 h and 24 h (p < 0.01), with a half-life close to 24 h, the highest concentration can reach 1000 ng/mL.16,17 Therefore, if sepsis is suspected, blood samples should be quickly collected for PCT testing to confirm the presence of infection as soon as possible, and timely and effective treatment measures should be taken to save the patient’s life. In the progression of infectious disease severity, PCT concentrations vary from low to high with infection severity. 56 In sepsis, elevated PCT levels are associated with disease severity and mortality. Compared with other inflammatory markers such as IL-6 or CRP, PCT is more accurate in diagnosing sepsis. 14 When infection is under control and concentrations of endotoxins and pro-inflammatory mediators are reduced, PCT concentrations decrease, 57 and if treated appropriately, PCT levels decrease by approximately 50% per day. 58 When the normal human serum PCT value is less than 0.05 ng/mL and the PCT increases from 0.5 ng/mL to more than 2 ng/mL, systemic infection is considered.
However, in patients with severe hepatic or renal dysfunction or in the first few days after surgery/trauma, a PCT of 0.5–2 ng/mL is considered normal. Infection and SIRS are highly suspected when PCT levels are 2–10 ng/mL, and sepsis or septic shock are highly likely (over 90%) when PCT is >10 ng/mL.59,60 For patients with acute onset of urosepsis, acute symptoms, and low serum PCT levels, it is recommended to review PCT 6–12 h later. A prospective study by Anand et al. confirmed the role of PCT in differentiating culture-negative sepsis from non-infectious SIRS, and PCT could accurately distinguish culture-negative and culture-positive sepsis from non-infectious SIRS, thereby contributing to the early diagnosis and effective management of these diseases.
In the culture-negative group, the optimal cut-off point for PCT was 1.43 ng/mL (92% sensitivity; 83% negative predictive value). 61 The average value of serum PCT in patients with urinary tract infection complicated with bacteremia was (8.08 ± 16.37) ng/mL, and the sensitivity, specificity, positive predictive value, and negative predictive value of urinary tract infection and negative predictive value with PCT ⩾ 1.16 ng/mL as the diagnostic criteria, Bacteremia was 100%, 97%, 84%, and 100%, which were significantly better than serum Lac, CRP, and WBC levels. 62 High levels of PCT can be used as biomarkers for diagnosing urosepsis and identifying severe bacterial infections, and continuous dynamic measurement of PCT levels can effectively guide the use of antibiotics in urosepsis. 63
The high timeliness, sensitivity, and specificity of PCT can provide effective laboratory evidence for early warning and diagnosis of urosepsis in clinical work. For patients with suspected urosepsis, serum PCT should be detected immediately. However, PCT is not a universal and perfect biomarker, as any cellular injury, whether direct tissue damage or non-infectious ischemia-reperfusion injury, results in elevated PCT. 58 This can lead to clinician misdiagnosis and unnecessary antibiotic use. In addition, PCT has no clear value in the diagnosis of sepsis during its use, so when using PCT as a biomarker for diagnosing urosepsis, it should always be combined with the clinical results of patients to avoid misjudgment.
CRP
CRP is an aglycosylated protein with a pentameric structure that is mainly released by the liver in response to IL-6, IL-1, and tumor necrosis factor (TNF)-α following inflammatory injury. 64 In normal health, CRP levels are usually low (generally below 10 mg/L). 51 When inflammation, infection, or tissue damage occurs in the body, CRP rises within 12–24 h and peaks within 2–3 days, increasing to 1000-fold normal levels.65–67 Compared with uncomplicated urinary tract infection, patients with urosepsis have significantly higher CRP. 18 A prospective study by Povoa found that CRP levels correlated with the severity of infection. The cut-off value of CRP was 8.7 mg/dL, and the sensitivity and specificity of CRP for diagnosing infection were 93.4% and 86.1%, respectively. Specificity increased to 100% when body temperature exceeded 38.2°C. A follow-up study by the same team further validated the CRP cut-off value of 8.7 mg/dL and concluded that it had an 88% risk of infection. 68 And higher CRP [p < 0.001, odds ratio (OR) = 1.015] were independent predictive factors for increased 28-day mortality in sepsis patients. 19 Although CRP is not as sensitive as PCT and IL-6 in urosepsis 63 and has a certain lag, 69 it can still be used as an auxiliary diagnostic factor to help diagnose urosepsis. In particular, dynamic and continuous monitoring of changes in PCT, IL-6, and CRP in clinical practice can greatly help diagnose urosepsis and understand the progression of infection.
Lactic acid (Lac)
Lac is a product of anaerobic metabolism of hypoxic cells in tissues. 70 Accelerated anaerobic glycolysis in urosepsis with hypotension, cellular hypoxia, and hypoperfusion of tissues and organs can lead to elevated Lac levels, manifesting as hyperlactatemia. In addition, the metabolism of Lac depends on liver and kidney function. In urosepsis patients, organ function and Lac clearance are impaired, which also leads to elevated serum Lac. 71 Lac is an independent risk factor for death in patients with urosepsis 20 and is closely related to patient prognosis. Lac levels have long been used in sepsis screening and management to help physicians make clinical decisions. The addition of Lac levels to the quick SOFA (qSOFA) score improved the validity of predicting the occurrence of sepsis, 21 making the ability of the qSOFA score to predict sepsis comparable to that of the SOFA score. 72
The normal value of serum Lac should be <2.0 mmol/L. Relevant studies have shown that when serum Lac is elevated in sepsis patients, the patients tend to have poorer prognosis and higher mortality.73,74 An initial Lac ⩾4.0 mmol/L was associated with a six-fold increased risk of mortality in the acute phase 22 and to some extent represented hypoperfusion in the tissues of septic patients, which was included in the 2016 sepsis and septic shock guidelines for early identification. 1 In patients with septic shock, the initial Lac level and 6-h Lac clearance are associated with 28-day mortality, and it is suggested that Lac should be normalized within 6 h after fluid resuscitation, 23 which can reduce patient mortality, and early normalization of Lac and Lac clearance greater than 50% are reliable predictors of survival in patients with sepsis. 24
Undeniably, serum Lac can be effectively used to predict prognosis, facilitate treatment, and understand the course of sepsis. 75 But when hyperlactatemia is not caused by tissue hypoperfusion, fluid resuscitation and Lac removal can be detrimental. 72 Current sepsis guidelines still emphasize Lac as a marker of low perfusion rate, and for many clinicians, elevated Lac has become almost synonymous with sepsis, followed by fluid resuscitation and empiric antibiotic administration, which is incorrect. Better use of Lac monitoring will serve as an early warning sign for clinicians to reassess end-organ perfusion and fluid responsiveness and look for the cause of Lac elevations for timely intervention.
Other markers
LncRNAs (long non-coding RNAs)
LncRNAs are a class of non-coding RNAs over 200 nucleotides in length without open reading frames. 76 They cannot be translated into proteins, but they have a variety of important physiological functions. With the development of high-throughput sequencing technology and gene chips, more and more studies have confirmed that lncRNAs are closely related to sepsis.77,78 LncRNAs can modulate sepsis by modulating different signaling pathways. For example, taurine upregulation 1 (TUG1) can reduce sepsis-induced inflammation and apoptosis by targeting Mir-34b-5p and Grb2-associated binding protein (GAB1). 79 During sepsis, the expression of metastasis-associated lung adenocarcinoma transcript 1 (MALAT1) is increased, and the combination of MALAT1 and Mir-23a can upregulate the expression of mast cell-expressed membrane protein 1 (MCEMP1), 80 thus promoting sepsis inflammatory response of the disease.
Previous studies have shown that MALAT1 expression is positively correlated with APACHE II score (p < 0.001) and SOFA score (p < 0.001), 77 suggesting that MALAT1 may be a biomarker for the diagnosis of uremia. Scholars have also discovered the role of lncRNAs in the prognosis of patients with urosepsis. For example, LncRNA ENST00000504301.1 is more expressed in sepsis survivors than LncRNAENST00000452391.1. LncRNANEAT1 is expressed at higher levels in deceased sepsis patients than in sepsis survivors.81,82 The circulating lncRNA ZFAS1 has shown good diagnostic and predictive value in sepsis and is inversely associated with disease risk and severity. 83 Huang et al. found that when peripheral blood mononuclear cells (PBMCs) from sepsis patients were stimulated with lipopolysaccharide in vitro, the expression of nuclear paraspeckle assembly transcript 1 (NEAT1) increased rapidly and peaked 2 h after endotoxin treatment. In contrast, PCT takes 12–48 h to peak. 25 The LncRNA NEAT1 can be used as a combined biomarker in patients with sepsis. 84 RNA-Seq (RNA sequencing technology) study based on the expression profile of endotoxin-responsive LncRNA in human microvascular endothelial cells found that LncRNA EGO and HOTAIRM1 were heterogeneously expressed at 3 h, while LNC-IL7R was significantly upregulated at 24 h. 26 All these suggest the feasibility of lncRNAs as diagnostic biomarkers for urosepsis. In addition, quantitative polymerase chain reaction (QPCR) can rapidly quantify lncRNAs in patient blood in a shorter time than bacterial culture, which is an advantage of lncRNAs as biomarkers for urosepsis.
However, studies to elucidate the specific mechanisms of these lncRNAs in sepsis are still lacking. We should pay more attention to the molecular mechanism of LncRNAs and better understand the role of LncRNAs in sepsis to tap the great potential of LncRNAs in the diagnosis and treatment of urosepsis.
PTX3 (Pentraxi3)
Pentraxins are a family of polymeric proteins, divided into short and long pennectins. CRP is the prototype of the short pentamer subfamily, while PTX3 is the prototype long pentamer. 85 The difference is that CRP is produced in the liver, whereas PTX3 is produced in peripheral tissues. 86 PTX3 is an acute-phase protein that is barely detectable (<1 ng/mL) in normal human plasma, 87 and its plasma concentration increases rapidly under various inflammatory conditions, including sepsis, circulating in patients with sepsis PTX3 levels are elevated, and this value is even higher in patients with septic shock, reaching as high as 100 ng/mL 27 and even exceeding 800 ng/mL.28,88,89 Serum PTX3 levels have been shown to predict death from sepsis and septic shock.86,90,91 High serum PTX3 levels were associated with the severity of sepsis, and patients with high PTX3 levels on admission had a higher 90-day mortality rate than those with the lowest 25% levels. 92
Programmed death ligand-1
Programmed death ligand-1 (PD-L1) is a ligand for PD-1, a type 1 transmembrane protein of the immunoglobulin superfamily expressed on various immune cells.93,94 Studies have shown that PD-L1 and PD-1 expression is increased in lymphocytes of patients with sepsis, 29 which may reflect the severity and clinical outcomes of patients with sepsis.30,31 Determining monocyte PD-L1 expression has been shown to be a promising independent prognostic marker in patients with septic shock. 95
Conclusion
Biomarkers such as WBC, NLR, PCT, IL-6, CRP, lactate, and LncRNA all play specific roles in the early diagnosis or prognosis of urosepsis. For WBC, we do not just have to focus on abnormally elevated WBC counts in the blood. A sharp decline in WBC should be more alarming as it may indicate severe urosepsis. NLR values are superior to pure blood WBC counts in predicting infection severity, and we can combine the two to help predict the onset of urosepsis. PCT can distinguish between bacterial and non-bacterial sepsis and can also be used to determine the severity of sepsis and guide the use of antibiotics based on changes in PCT values; IL-6 first develops from infection to sepsis and is superior to PCT in predicting patient mortality; and CRP combined body temperature (>38.2°C) can be used to diagnose urosepsis. The three play a role in different stages of infection, and their combined use can determine the progression of patients with urosepsis. Elevated Lac values in patients with urine-derived sepsis usually indicate a poor prognosis, and we should actively look for and treat-elevated lactate concentrations. New markers such as LncRNA and PD-L1 can be used to diagnose sepsis, and PTX3 can predict septic shock, but the mechanisms of these three biomarkers in the sepsis process have not been specifically elaborated and require further study for clinical use.