
Abstract
Background:
The model for end-stage liver disease (MELD) has been widely used to predict the mortality and morbidity of various surgical procedures.
Objectives:
We aimed to correlate a high preoperative MELD score with adverse 30-day postoperative complications following radical cystectomy.
Design and Methods:
Patients who underwent elective, non-emergency radical cystectomy were identified from the American College of Surgeons–National Surgical Quality Improvement Program (ACS-NSQIP) database from 2005 to 2017. Patients were categorized according to a calculated MELD score. The primary outcomes of this study were 30-day postoperative mortality, morbidity, and length of hospital stay following radical cystectomy. For further sensitivity analysis, propensity score matching was used to yield a total of 1387 matched pairs and primary outcomes were also assessed in the matched cohort.
Results:
Compared with patients with a MELD < 10, those with MELD ⩾ 10 had significantly higher rates of mortality [odds ratio (OR) = 1.71, p = 0.004], major complications (OR = 1.42, p < 0.001), and prolonged hospital stay (OR = 1.29, p < 0.001) on multivariate analysis. Following risk-adjustment for race, propensity-matched groups revealed that patients with MELD score ⩾ 10 were significantly associated with higher mortality (OR = 1.85, p = 0.008), major complications (OR = 1.34, p < 0.001), yet similar length of hospital stay (OR = 1.17, p = 0.072).
Conclusion:
MELD score ⩾ 10 is associated with higher mortality and morbidity in patients undergoing radical cystectomy compared with lower MELD scores. Risk-stratification using MELD score may assist clinicians in identifying high-risk patients to provide adequate preoperative counseling, optimize perioperative conditions, and even consider nonsurgical alternatives.
Introduction
Bladder cancer (BC) is the second-most common cause of death among all genitourinary tumors and ranks 10th among the most common malignancies in the world. 1 The predominant form of BC manifests as urothelial carcinoma, with a 5-year overall survival rate for localized, regional, and distant disease reported to be 91%, 48%, and 8%, respectively. 2 Radical cystectomy (RC) with extended lymphadenectomy is the gold standard treatment modality for muscle invasive BC (MIBC), as well as non-muscle invasive BC (NMIBC) that do not respond to transurethral resection of bladder tumor (TURBT) and intravesical therapy. 3 It is generally known that RC entails a highly comorbid procedure associated with several complications and significant rates of postoperative morbidities and mortalities.4,5 The ability to identify high-risk patients enables clinicians to optimize perioperative care and even consider alternative approaches to RC, such as bladder-sparing trimodal therapy. 6 As such, patient selection strategies that are based on objective measures of pre-operative risks of surgery are highly warranted. Model for end-stage liver disease (MELD) was originally introduced in 1999 as a 3-month survival predictor model in patients undergoing transjugular intrahepatic portosystemic shunting (TIPS)7,8 and was calculated from routinely derived serum chemistries; it was further adjusted to be used in liver transplant recipient selection.9,10 MELD was also shown to predict adverse surgical outcomes in patients regardless of their liver state, where it was found to be an independent predictor of morbidity and mortality in patients undergoing emergent or elective colorectal surgery,11–13 pancreatoduodenectomy, 14 gastrectomy, 15 and lower extremity bypass. 16 Few studies have explored MELD score as an independent predictor of morbidity and mortality in RC. One case-series demonstrated that three patients with liver cirrhosis undergoing RC demonstrated an increased likelihood of complications with higher MELD scores. 17 Others have recommended that patients with localized BC and MELD > 10 differ from RC and pursue alternatives. 18
Using the American College of Surgeons–National Surgical Quality Improvement Program (ACS-NSQIP) database, we sought to explore the MELD score’s ability to accurately risk-stratify patients undergoing RC and be an independent predictor of 30-day postoperative outcomes following RC.
Materials and methods
Study design and patient population
Our cohort was retrospectively derived from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) Participant Use Data Files (PUFs) between the years 2005 and 2017. We selected patients who underwent elective, non-emergent RC using the following Current Procedural Terminology (CPT) codes: 51570, 51575, 51580, 51585, 51590, 51595, and 51596. Urinary diversion (UD) methods were coded according to their corresponding CPT codes: 51585 [ureterosigmoidostomy (USD) or ureterocutaneous diversion (UCD) with lymph node dissection (LND)], 51590 [ileal conduit (IC) or sigmoid bladder (SB)], 51595 (IC or SB with LND), and 51596 [neobladder (NB)]. We excluded patients who had missing laboratory values included in the MELD score, and those who underwent other concomitant procedures such as chemotherapy or radiotherapy. The ACS-NSQIP database is a nationally validated, risk-adjusted, outcome-based program that encompasses 963 centers and more than 65 collaboratives both inside and outside the United States. The ACS-NSQIP database is managed by a board of surgical clinical experts who are responsible for collection and maintenance of the data. Interrater reliability (IRR) audits occur at participant centers to periodically review data files ensuring the highest quality and standards possible.
Ethics approval
Patient consent and Institutional Review Board (IRB) approval were not required as the data are de-identified.
Patient demographics and variables
Patient demographics, pre-operative laboratory values, medical comorbidities, and preoperative events and UD were reported. Patient demographics included age, body mass index (BMI), sex, race, history of smoking within 1-year status, and American Society of Anesthesiologists’ (ASA) classification. Patient comorbidities included diabetes, history of chronic obstructive pulmonary disease (COPD), congestive heart failure, hypertension requiring medication, acute renal failure, steroid use, weight loss defined as > 10% weight loss in the last 6 months, and bleeding disorders. Pre-operative events recorded include blood transfusion of packed red blood cells 72 h before surgery, pre-operative dialysis, and systemic sepsis. UD included IC or SB with or without LND, NB, and USD or UCD with LND. Missing values were imputed using mean or median for continuous variables and mode for categorical variables. Values were imputed only if they amounted to < 10% from the total amount of values in the variable. If a variable had > 10% missing values, it was excluded from the analysis.
MELD score calculation
MELD score was calculated using preoperative serum creatinine, bilirubin, and international normalized ratio (INR). MELD score was calculated using the standard United Network for Organ Sharing (UNOS)-based formula: MELD = 3.78 × ln [bilirubin (mg/dL)] + 11.2 × ln [INR] + 9.57 × ln [creatinine (mg/dL)] + 6.43. The result was rounded to the nearest integer. All values less than 1.0 were rounded up to 1.0 to avoid a negative score and creatinine values > 4 mg/dL were trimmed down to 4.0 mg/dL in a previously validated manner. 14 Patients were then categorized into two groups depending on the MELD score: < 10 and ⩾ 10. The numerical cutoff of 10 was chosen based on previous literature that clearly correlated that cut-off with worse postoperative mortality.19,20
Outcomes
We sought to compare 30-day outcomes that included mortality, major morbidity, and prolonged length of hospital stay defined as greater than 11 days (75th percentile). Major morbidity included deep surgical site infection (SSI), organ SSI, wound disturbance, pneumonia, unplanned intubation, pulmonary embolism, failure to wean off ventilator > 48 h, acute renal failure, renal insufficiency, cardiac arrest requiring cardiopulmonary resuscitation (CPR), myocardial infarction, bleeding requiring transfusion, sepsis, septic shock, or deep vein thrombosis (DVT).
Statistical analysis and model construction
Patient demographics, comorbidities, pre-operative incidences, diversion type, and 30-day outcomes were compared between the two MELD groups. Categorical variables were compared using chi-square test and presented as count and percentages while continuous variables were analyzed using independent t-test and presented as mean and standard error of the mean. Next, to assess for confounding variables and effect modifiers on our outcomes of interest, we performed multivariate logistic regression models controlling for differences in demographics, comorbidities, pre-operative events, and UD type. Multivariate logistic regression models were adjusted for age, race, sex, ASA, smoking status, diabetes, congestive heart failure, hypertension, acute renal failure, dialysis, weight loss, bleeding disorder, blood transfusion, and diversion type.
Propensity score matching
As a sensitivity analysis, we performed propensity score matching by 1:1 match between the two MELD groups. The variables we included for the propensity matching were age, race, sex, ASA, diabetes, smoking status, congestive heart failure, hypertension, acute renal failure, dialysis, weight loss, bleeding disorder, blood transfusion, and diversion type. For variables that did not successfully match, we performed a multivariate logistic regression for those variables in the propensity-matched cohorts. Significance level was set at < 0.05 for all analyses. Statistical analyses were performed using the IBM SPSS statistical package (version 28, IBM Corp., Armonk N.Y., USA).
Data availability
The ACS-NSQIP data are subject to a data use agreement. To access the dataset, a request to the ACS-NSQIP participant use form should be placed at the following link (https://www.facs.org/quality-programs/acs-nsqip/participant-use). The American University of Beirut Medical Center (AUBMC) is enrolled in ACS-NSQIP as a participating center. As such, the data were made available by the ACS-NSQIP center and the AUBMC Department of Surgery after signing the data use agreement.
Results
Patients demographics and general characteristics stratified by MELD score
Between 2005 and 2017, out of 7120 cystectomy cases, 5038 elective cystectomy cases had quantifiable MELD scores. MELD groups included 3486 patients with MELD < 10 and 1552 patients with MELD ⩾ 10. In our study, all categorical variables had no missing values and continuous variables not related to the MELD score calculations were imputed such as no variable consisted of > 10% missing values. Overall, individuals with MELD scores ⩾ 10 were older, males, ASA class > 2, diabetic, history of congestive heart failure, hypertensive, with acute renal failure, > 10% weight loss, with bleeding disorders, pre-operative bleeding transfusion, and dialysis. Patients with MELD scores ⩾ 10 were also more likely to undergo IC or SB with or without LND and less likely to undergo NB (p < 0.007). After propensity score matching, the matched cohort consisted of 2764 patients where two MELD groups matched on all factors except for race (Table 1).
Characteristics of patients who underwent cystectomy between the years 2005 and 2017 stratified by MELD score.
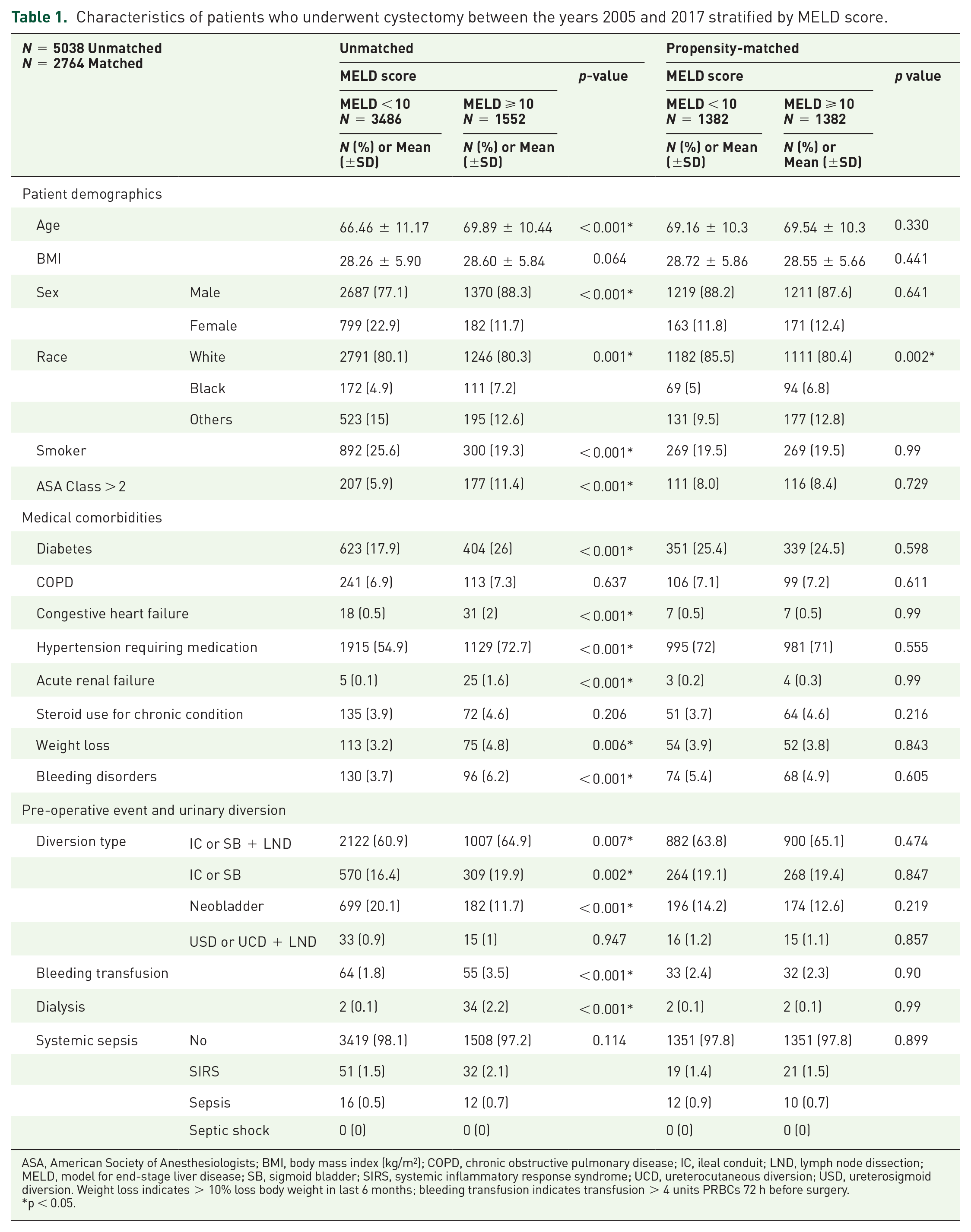
ASA, American Society of Anesthesiologists; BMI, body mass index (kg/m2); COPD, chronic obstructive pulmonary disease; IC, ileal conduit; LND, lymph node dissection; MELD, model for end-stage liver disease; SB, sigmoid bladder; SIRS, systemic inflammatory response syndrome; UCD, ureterocutaneous diversion; USD, ureterosigmoid diversion. Weight loss indicates > 10% loss body weight in last 6 months; bleeding transfusion indicates transfusion > 4 units PRBCs 72 h before surgery.*p < 0.05.
Thirty-day postoperative outcomes stratified by MELD score
In the unmatched cohorts, patients with MELD ⩾ 10 had significantly higher rates of mortality (4.4%, p < 0.001), major morbidity (61.0%, p < 0.001), and prolonged length of stay (31.9 days, p < 0.001) as compared with those with MELD < 10 (Table 2). After propensity score matching, we were left with a total of 2764 patients (1382 per group). In this cohort, a similar trend was seen where patients with MELD ⩾ 10 still had significantly higher rates of mortality (3%, p = 0.006) and major morbidity (59.3%, p < 0.001) as compared with those with MELD < 10. As for length of hospital stay, patients with MELD ⩾ 10 had higher rates of prolonged hospitals stays (> 11 days; 30.5%, p = 0.026) when compared with MELD < 10.
Description of the main postoperative outcomes stratified by MELD score.

CPR, cardiopulmonary resuscitation; DVT, deep vein thrombosis; MELD, model for end-stage liver disease; SSI, surgical site infection.
Prolonged length of stay is defined as length of stay greater than 11 days.
Major morbidity is the composite outcome of postoperative incidence of major complications include deep surgical site infection, organ surgical infection, wound disturbance, pneumonia, unplanned intubation, pulmonary embolism, failure to wean off ventilator > 48 h, renal insufficiency, acute renal failure, cardiac arrest requiring CPR, myocardial infarction, bleeding requiring transfusion, sepsis, septic shock, or deep vein thrombosis.
Failure to wean indicates failure to wean off ventilator > 48 h.*p < 0.05.
Multivariate analysis of outcomes in unmatched and propensity-matched cohorts
In the unmatched cohort, a multivariate logistic regression was performed to control for age, race, sex, diabetes, smoker, congestive heart failure, hypertension, acute renal failure, dialysis, weight loss, bleeding disorder, blood transfusion, ASA, and diversion type (Table 3). The model showed that patients with MELD ⩾ 10 had higher odds of mortality (OR = 1.71, p = 0.004), major morbidity (OR = 1.42, p < 0.001), and prolonged length of stay (OR = 1.29, p < 0.001) as compared with those with MELD < 10. For the propensity-matched cohorts, a multivariate logistic regression was performed to control for race. The model showed that patients with MELD ⩾ 10 had higher odds of mortality (OR = 1.85, p = 0.008) and major morbidity (OR = 1.34, p < 0.001); whereas differences in length of hospital did not reach statistical significance (OR = 1.17, p = 0.072).
Univariable and multivariable analysis of characteristics and risk factors of patients who have undergone cystectomy between 2005 and 2017 stratified by MELD score.

MELD, model for end-stage liver disease; Ref: reference.
Univariate logistic regression model.
Multivariate logistic model adjusted for age, race, sex, diabetes, smoker, congestive heart failure, hypertension, acute renal failure, dialysis, weight loss, bleeding disorder, blood transfusion, ASA (American Society of Anesthesiologists’ classification), urinary diversion type.
Multivariate logistic regression model adjusted for race.
Major morbidity is the composite outcome of postoperative incidence of major complications include deep surgical site infection, organ surgical infection, wound disturbance, pneumonia, unplanned intubation, pulmonary embolism, failure to wean off ventilator > 48 h, renal insufficiency, acute renal failure, cardiac arrest requiring CPR (cardiopulmonary resuscitation), myocardial infarction, bleeding requiring transfusion, sepsis, septic shock, or deep vein thrombosis.*p < 0.05.
Discussion
There exists an increasing interest for pre-operative risk stratification for which various attempts were made to develop and validate scores as independent predictors of overall complications. These include frailty and comorbidity indices such as the five-item frailty score, Charlson comorbidity index, and Johns Hopkins Adjusted Clinical Groups frailty index.21–23
Baseline liver disease is associated with a higher risk of perioperative complications and long-term postoperative adverse outcomes in non-hepatic surgeries.19,24–27 And so, the idea of quantifying a patient’s preoperative risk by using an already available liver disease score arose. The UNOS-stratified MELD score (⩽ 10, 11–18, 19–24, 25–35, and > 36), with a higher score associated with an increase in estimated 3-month mortality rates.28,29 MELD is already known to accurately risk-stratify patients with liver cirrhosis undergoing abdominal, musculoskeletal, cardiovascular, and urologic surgeries;20,30–34 in fact, irrespective of underlying liver disease, it was shown to be an independent predictor of morbidity and mortality in patients undergoing several emergency or elective procedures.11–16
Higher MELD scores are independently associated with an increased 30-day mortality and morbidity following gastrectomy and colorectal surgery,11,13 whereas a MELD score > 11 was associated with a twofold increase in mortality for patients undergoing pancreatectomy. 14 In addition, Krafcik et al. 16 correlated a higher MELD score with prolonged hospital stay in patients undergoing lower extremity bypass.
Similarly, the results presented in this study highlight the role of MELD scores in predicting outcomes following elective RC where a MELD score ⩾ 10 revealed to be an independent predictor of overall mortality, major morbidity, and prolonged hospital stay following RC. Our findings revealed that irrespective of underlying liver disease, patients undergoing RC with MELD scores ⩾ 10 performed poorly in the postoperative setting as compared with those with MELD < 10. Furthermore, patients with MELD ⩾ 10 had prolonged length of stay and were at a higher risk of mortality and major morbidity such as deep incisional surgical site infections, unplanned intubation, renal insufficiency, renal failure, septic shock, and bleeding requiring transfusion.
In addition, perioperative mortality after RC within 30 days of surgery or prior to hospital discharge has decreased from 20% in 1970 to nearly 1–2% in recent studies, whereas perioperative mortality within 60- and 90-days post-surgery remains higher at 2.4% and 3.9%, respectively.35,36 As such, several attempts were made to determine variables that can predict mortality following RC. Many of those variables were difficult to quantify such as the surgeon’s experience and the institution’s surgical volume.36,37 Similarly, attempts at finding variables to predict prolonged hospital length of stay following RC were equally difficult to quantify. 38 On the contrary, MELD score provides a noninvasive objective tool to help identify high-risk patients for perioperative complications and prolonged hospital length of stay.
Furthermore, other factors that could influence outcomes post-RC include surgical approach. Robotic-assisted RC (RARC) has been found to be comparable with open RC (ORC) in terms of peri-operative outcomes, progression free-survival, and health-related quality of life indicators.39–41 One randomized clinical trial demonstrated that RARC with intracorporeal UD displayed lower peri-operative transfusion rates (22% versus 41%) as compared with ORC. 42 In addition, an interim analysis of the same trial showed that RARC and ORC displayed similar patient-reported quality of life domains. 43 Nevertheless, patients undergoing ORC displayed a decrease in role functioning and higher symptom scales after 1 year; however, RARC candidates reported an increase in urinary symptoms and problems. 43 In our study, the type of surgical approach could have influenced peri-operative outcomes between the different MELD categories. Unfortunately, the NSQIP dataset lacks CPT codes that help indicate the surgical approach utilized (open, robotic, or laparoscopic) and this could be a subject of future research when comparing surgical techniques in RC.
The type of UD during RC is an essential predictor of peri-operative complications as it adds great complexity to an already complicated procedure. Different types of UDs have been compared in regard to patient selection, peri-operative complications and quality of life parameters. Studies have shown that IC patients are generally older with greater comorbidities and complications and report poorer quality of life when compared with NB candidates. 44 One study showed that the complication rate of NB was around 58% with most common complications being infectious, genitourinary, gastrointestinal, and wound related ones. 45 Furthermore, NB have been shown to be more technically demanding procedures with longer operative times and hospital stays when compared with IC.44,46 Regarding overall morbidity and mortality, NB have displayed similar rates when compared with IC with greater infectious complications in the NB group as compared with wound complications in the IC group.46–48 Whereas other studies have indicated superiority of incontinent diversions to continent diversions. 49 In our study, patients with lower MELD scores were in fact younger and generally less comorbid before propensity score matching and were more likely to undergo NBs and less likely to undergo IC as compared with individuals with higher MELD scores. However, after matching for diversion types, the two groups displayed consistent results. Further randomized studies are required with homogenized patient populations whereby morbidity and mortality can be further compared.
Pre-operative MELD scores can be used as a prognostic marker of peri-operative complications regardless of a pre-existing liver disease. Given the aforementioned results, clinicians may consider using the MELD score as a convenient and available model to risk-stratify patients, provide proper patient counseling, and consider less invasive alternatives such as trimodal therapy. 6
Limitations
Several limitations exist in our study and results must be interpreted within the context of the study design. First, our study is based on a retrospective analysis using the ACS-NSQIP database and might be subject to selection bias. Second, the ACS-NSQIP database misses out on important factors such as tumor stage and complexity, which may alter outcomes significantly and impact morbidity and mortality after surgery. Third, MELD score was originally optimized to select cirrhotic patients for TIPS and later for liver transplantation. It’s recent extrapolation to be used as a risk assessor for non-transplant surgeries may be influenced by many factors including a recent illness or dehydration. 14 Furthermore, the NSQIP dataset lacks CPT codes indicating the surgical approach during RC (open, robotic, or laparoscopic). Hence, a comparison between different surgical approaches was not possible. In addition, alcohol intake was not reported in NSQIP datasets after 2012, which is considered an important exclusion criterion from MELD scores. The final limitation is the follow-up interval where the ACS NSQIP user file registers a 30-day outcomes follow-up rather than the usual 90-day outcomes follow-up.
Conclusion
The findings presented in this study highlight the role of applying an established scoring system to pre-operatively identify high-risk patients for RC. The ability of MELD score to accurately risk-stratify 30-days surgical outcomes in a large patient cohort may assist clinicians in identifying high-risk patients to provide adequate preoperative counseling, optimize perioperative conditions, and even consider nonsurgical alternatives. It also sheds light on the implications of subclinical liver disease on 30-day postoperative complications. Future studies are needed to develop a complex model that integrate several scores as a prognostic modality for RC patients.