
Abstract
Background:
Enhanced recovery after surgery (ERAS) protocols decrease the length of hospital stay (LOS) and complications following radical cystectomy (RC). However, the impact of non-modifiable patient factors to postoperative outcome is unclear. This study aimed to identify nonmodifiable patient and disease factors predictive of post-RC outcomes with ERAS protocols.
Methods:
We reviewed our institutional review board-approved prospectively maintained bladder cancer database. Patients with primary urothelial bladder cancer who underwent open RC with ERAS protocol between 2012 and 2016 were identified. Patient demographic and disease-relevant variables were reviewed. Factors predictive of LOS, 30- and 90-day complications and readmission were assessed using univariate and multivariable analyses.
Results:
A total of 289 patients with a median age of 70 years were included, of whom 80.6% were male, 33.6% had Charlson comorbidity index ⩾2. Median LOS was 4 days and 21.1% received intraoperative transfusion. The 30-day complication and readmission rates were 58.8% and 16.6%, respectively. Age >70 (p = 0.02), Charlson comorbidity index ⩾2 (p = 0.005), and intraoperative transfusion (p = 0.03) were significantly associated with LOS. Intraoperative transfusion was significantly associated with 30-day complication and readmission (p = 0.008, p = 0.005, respectively). No factor was found to be significantly associated with 90-day complication or readmission.
Conclusions:
With ERAS protocol, non-modifiable patient and disease factors influence outcomes after RC. Risk adjustment for these factors is important for patient counseling, quality assessment and future reimbursement.
Introduction
Fast-track or enhanced recovery after surgery (ERAS) protocols have been developed to improve perioperative outcomes by addressing issues relevant to surgical performance and recovery in a multimodal multidisciplinary approach. 1 These techniques have proven successful and have been implemented across virtually all surgical disciplines. 2 Within the field of urology, radical cystectomy (RC) has been most targeted for application of ERAS principles due to significant associated morbidity, lengthy postoperative hospitalizations, and high rates of complications and readmission. Applying ERAS protocols among patients undergoing RC has resulted in shortened length of stay (LOS) and decreased gastrointestinal-related complications without significantly impacting complication rates or hospital readmission.3,4 In a contemporary evaluation of outcomes following open radical cystectomy (ORC), postoperative LOS was decreased to median 4 days versus 7 days prior to ERAS implementation, and similar benefits have been demonstrated at additional centers.3,5,6
Nonetheless, RC remains one of the most challenging urological procedures. Beyond the inherent complexity of the procedure, bladder cancer is most prevalent among older patients with multiple comorbidities.7,8 Postoperative complications occur in 28–64% and are noted to be even higher when limited to elderly populations.8–10 Current studies on ERAS highlight the role of perioperative care in determining outcomes and emphasize the value of consistent and standardized care.11–13 However, the impact of nonmodifiable patient factors is more difficult to assess in the context of these confounding factors.
Our institution performs a high volume of RC annually and has a well-established ERAS protocol in which patient care is highly standardized at all levels. In this study, we sought to examine the impact of individual nonmodifiable as well as surgical-related factors among patients undergoing RC in the setting of ERAS to better characterize their role in driving postoperative outcomes.
Materials and methods
Study population
Patients with primary urothelial bladder cancer undergoing ORC, urinary diversion, and bilateral extended pelvic lymph node dissection at our institution by three fellowship-trained urologic oncologists from May 2012 to March 2016 were identified from our institutional review board-approved intent-to-cure bladder cancer database.
ERAS protocol
An institutional ERAS protocol was implemented in May 2012 for all consecutive patients. This protocol has been described previously and includes preoperative, intraoperative, and postoperative components; 3 preoperatively, patients have no bowel preparation but high-protein, high-carbohydrate liquid drinks. Intravenous antibiotics start just before surgery and continue for 24 h postoperatively. After the first 24 h, the patient is transitioned to oral suppressive antibiotics. Fluid intake is minimized intraoperatively after clipping the ureters, with careful monitoring of intravascular fluid volume. If a nasogastric tube was placed preoperatively, it is removed at the end of surgery. On the night of the surgery, patients are started on a clear liquid diet. If tolerated well, they proceed to a regular diet on postoperative day (POD) 1. Patients receive a cholinergic drug (neostigmine) and μ-opioid receptor antagonist (alvimopan) until the first bowel movement.
Discharge and follow up
Discharge criteria following ORC include adequate oral intake (over 1 L/day), bowel movement, pain control and expected laboratory values. Patients are discharged with oral prophylactic antibiotics, deep vein thrombosis prophylaxis and supportive intravenous hydration given by home health nurses every other day for 3 weeks. Postoperative visits are scheduled at 1, 3, 6 and 12–16 weeks. 3
Data collection and analysis
Patient data were captured prospectively by a research operator (GM), including demographics such as age, gender and body mass index (BMI), as well as clinical factors including Charlson comorbidity index (CCMI), American Society of Anesthesiologists (ASA) score and surgical-related factors, such as estimated blood loss (EBL), diversion type and pathology. Postoperative complications were graded according to Clavien–Dindo classification. Clavien–Dindo grades I and II were considered as minor complications; grades III–V were considered as major complications.
Statistical software package SAS®, version 9.4 (SAS Institute Inc., Cary, NC, USA) was applied to all analysis in this study. Pearson’s Chi-square or Fisher’s exact tests were used to examine categorical variables. The Kruskal–Wallis test was used to evaluate continuous variables. A stepwise linear regression was used to identify factors associated with LOS. A stepwise logistic regression was used to identify independent predictors of 30- and 90-day readmission and complications. All p-values reported are two-sided, with p < 0.05 considered statistically significant.
Results
A total of 289 consecutive patients were included in this study. Patient demographics, disease characteristics, surgical data and postoperative outcomes are demonstrated in Table 1. Median patient age was 70 years (range 38–91). The majority of patients were male (80.6%). The median LOS was 4 days (range 3–41). Minor and major complication rates at 30 days were 48.1% and 10.7%, respectively. Minor and major complication rates at 90 days were 54.7% and 21.4%, respectively. Readmission rates at 30 days and 90 days were 16.6% and 30.8%, respectively.
Patient demographics, disease characteristics, surgical data and postoperative outcomes (n = 289).
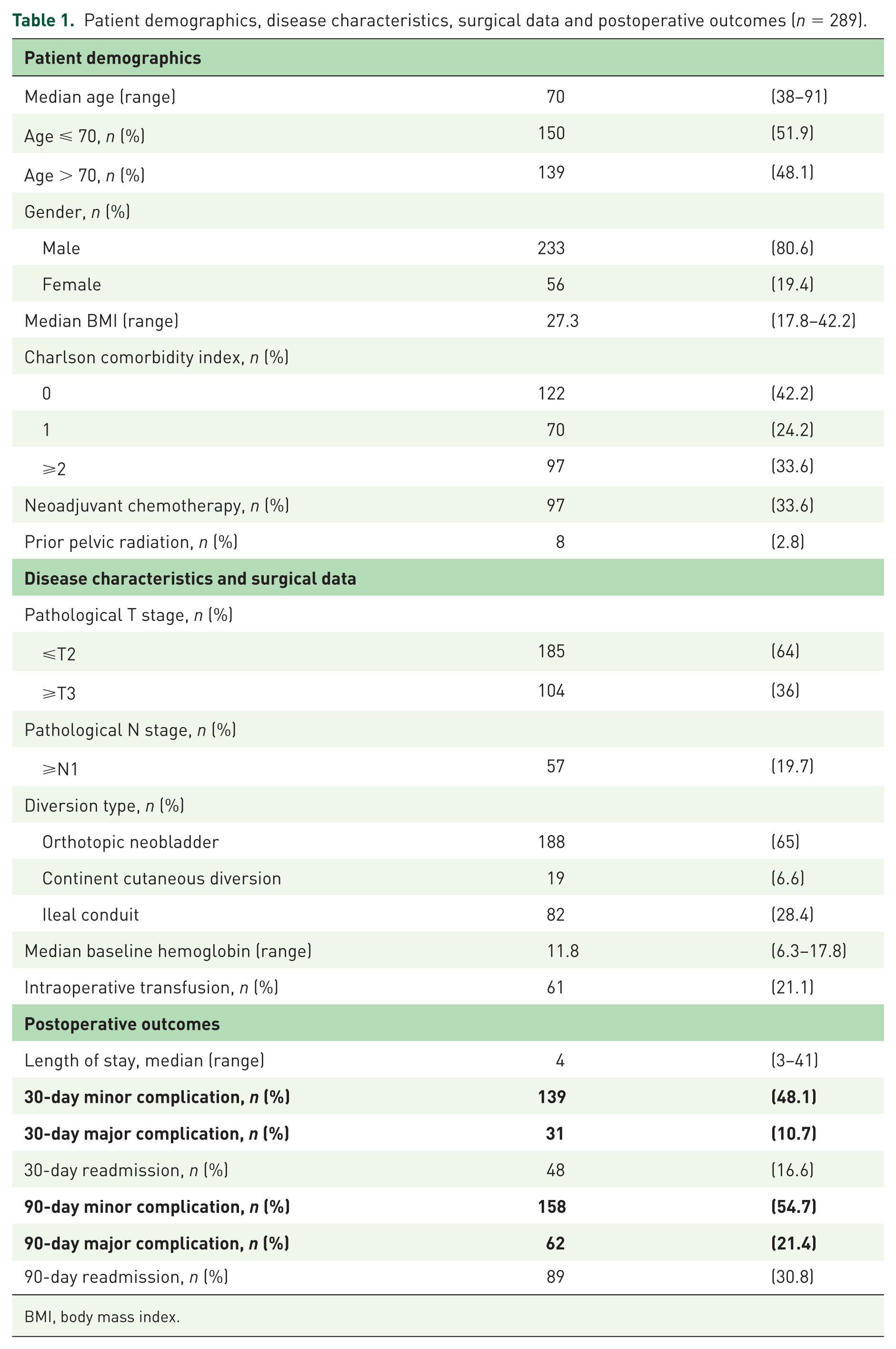
BMI, body mass index.
Length of stay
On univariate linear regression, significant associations with LOS were identified for age > 70 (p < 0.001), CCMI ⩾ 2 (p = 0.004), clinical stage ⩾ cT2 (p = 0.03), nonorthotopic urinary diversion (p < 0.001), and intraoperative transfusion (p = 0.007) (Table 2). On multivariable linear regression, age > 70 (p = 0.02), CCMI ⩾ 2 (p = 0.005), and intraoperative transfusion (p = 0.03) remained significant associations with LOS (Table 2). Parameter estimates (β) for each of these variables were greater than 1, indicating at least one additional day of hospitalization dependent on that variable.
Univariate and multivariable linear regression model of nonmodifiable factors impacting length of stay.

ASA, American Society of Anesthesiologists.
30- and 90-day complications and readmissions
Patients experiencing complications within 30 days postoperatively had lower baseline hemoglobin (HGB) levels (11.4 versus 12.0 g/dl, p = 0.04), higher intraoperative transfusion rate (26.5 versus 13.5%, p = 0.008) and longer LOS (5 versus 4 days, p < 0.001) (Table 3). Similarly, patients readmitted within 30 days postoperatively had lower baseline HGB levels (11.1 versus 11.9 g/dl, p = 0.05) and higher intraoperative transfusion rate (37.5 versus 18.7%, p = 0.006) (Table 4). No significant differences were identified with gender, BMI, ASA score, pathologic stage, diversion type, receipt of neoadjuvant chemotherapy, age or CCMI regarding 30-day complications or readmission. Multivariable logistic regression revealed a significant association between intraoperative transfusion and 30-day complications [odds ratio (OR) 2.32; 95% confidence interval (CI) 1.24–4.34; p = 0.009]. Patients receiving intraoperative transfusion were also significantly more likely to be readmitted within 30 days (OR 2.76; 95% CI 1.41–5.4; p = 0.003). No significant associations were found between variables of interest and 90-day readmission or complications in univariate or multivariate analyses (data not presented).
Demographics and surgical data of patients with and without complications within postoperative day 30.

BMI, body mass index; EBL, estimated blood loss; HCT, hematocrit; HGB, hemoglobin.
Demographics and surgical data of patients with and without readmission within postoperative day 30.
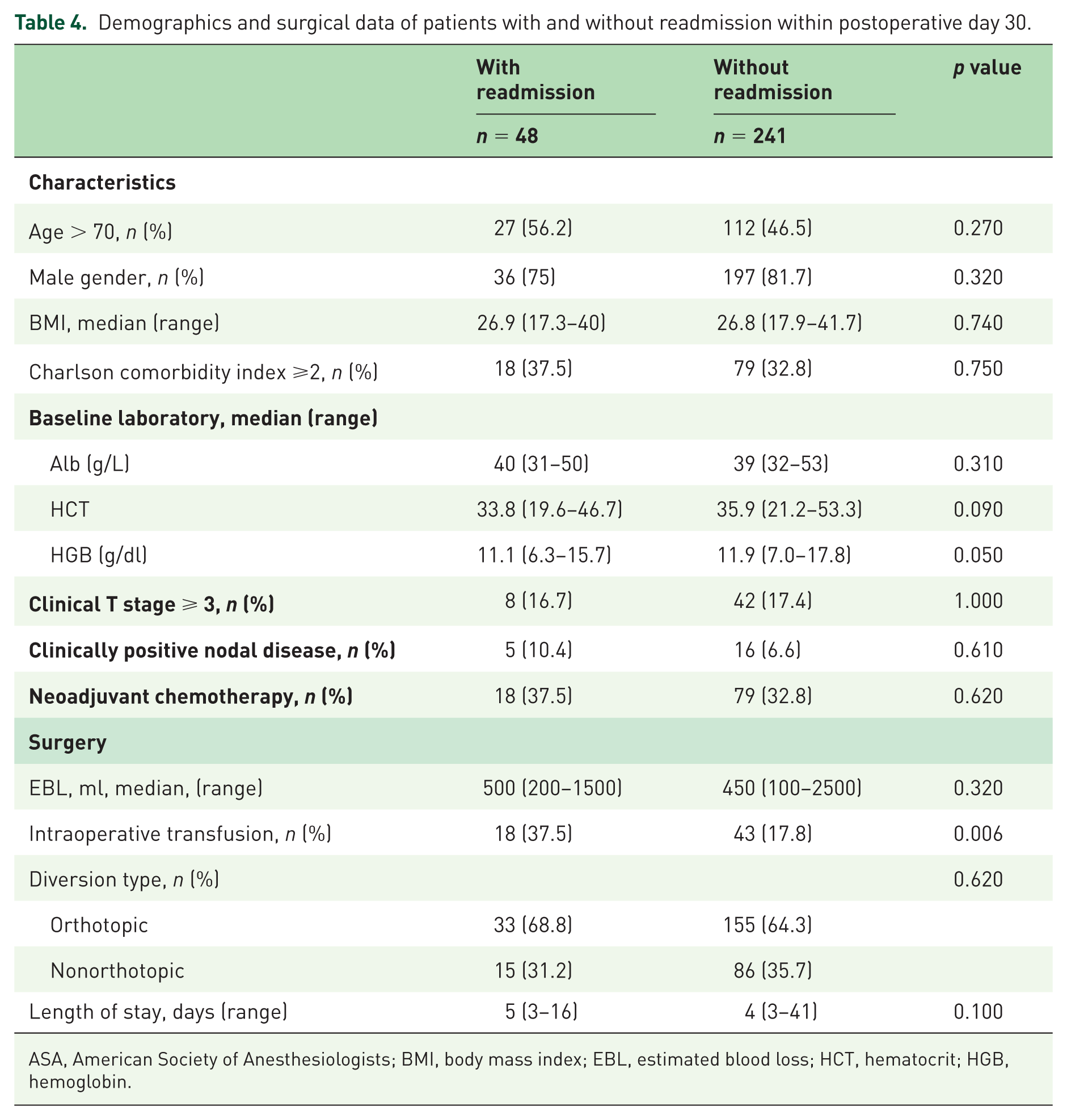
ASA, American Society of Anesthesiologists; BMI, body mass index; EBL, estimated blood loss; HCT, hematocrit; HGB, hemoglobin.
Discussion
Bladder cancer is a serious urological malignancy in the United States, with more than 79,000 new diagnoses and over 16,800 deaths estimated in 2017. 14 Although RC is considered the gold standard treatment for muscle invasive bladder cancer,15,16 it is associated with considerable morbidity. 17 The trends toward care standardization after RC have been driven by widespread introduction and utilization of ERAS protocols along with the demonstrated value of care centralization at high-volume centers of excellence. 13 Cost constraints and an ongoing shift from volume-based to value-based care have served to incentivize institutions and providers to limit expenditures by improving quality in the form of decreased postoperative LOS and minimizing perioperative complications.
Overall effects of these approaches remain to be determined as reimbursement models continue to evolve. Despite recent successes in improving outcomes such as LOS through ERAS protocols, the role of individual patient factors and of surgical variables must be appreciated to facilitate improved counseling and perioperative planning/management, and to inform assessments of quality. Knowing the impact of nonmodifiable factors on LOS, providers can modify preoperative patient counseling regarding expectations and potential alterations to care plans that may enhance patient and family experience and reported outcome. Nonmodifiable factors have been assessed in the setting of renal surgery determining association of older age, African American race, greater ASA score and social insurance status with discharge quality. 18 Another study found higher CCMI and nephrometry score associated with longer LOS following robotic-assisted partial nephrectomy. 19
In the current study, the impact of nonmodifiable and surgical-related factors on perioperative outcomes was evaluated in the context of a standardized surgical approach performed by three fellowship-trained urologic oncologists with an established ERAS pathway. We included only ORC cases in this study to prevent eluding of data and to maintain the homogeneity of the cohort, so that we have a better understanding of the effect of these factors without the confounding effect of the surgical approach. By limiting our analysis to ORC with ERAS, we have also minimized the confounding effect of a minimally invasive approach on assessment of variables of interest.
We looked at nonmodifiable demographic factors such as age and gender, as well as clinically and surgically relevant factors such as preoperative HGB, receipt of intraoperative transfusion and EBL. Defining factors as modifiable or nonmodifiable is important for future potential efforts toward preoperative risk modification. Some factors such as BMI must therefore be evaluated in the context of planned treatment to determine status as nonmodifiable. Given known negative consequences of delay of cystectomy, many factors were deemed nonmodifiable, though they may clearly be modified given adequate resources in the absence of time constraints. 20 Identification of specific predictive factors and determination of capacity for modification is essential and is the topic of ongoing research where factors such as mental health and sarcopenia have been linked to perioperative outcomes from RC.6,21,22 Among the limitations of these studies is an inability to delineate the potential role of perioperative care in compensating for or modifying the impact of the factors of interest. Also in this study, with regards to LOS, we observed that patient age > 70, and increased comorbidity index (CCMI ⩾ 2) were each associated with at least one additional day of hospitalization. The role of perioperative complications on LOS has been well-reported, with postoperative ileus the most common cause for extended hospitalization. 23 However, ERAS pathways and opioid receptor antagonists have greatly lessened gastrointestinal complications following cystectomy. 24 Factors contributing to LOS within an optimized ERAS protocol have therefore not been well-described.
A recent review of Medicare beneficiaries undergoing major surgical interventions found early discharge to be associated with lower total payments per episode, which were not offset by higher subsequent spending, suggesting earlier discharge possible serves to minimize expenditures. 25 However, a study evaluating patients undergoing RC at a single institution prior to ERAS implementation found LOS ⩽5 days to be associated with a significant independent increase in risk of major outpatient complication [hazard ratio (HR) 1.91; 95% CI 1.03–3.56; p = 0.04], and increased risk of readmission (HR 1.60; 95% CI 1.01–2.44; p = 0.048). 26 Therefore, optimizing LOS following RC is not clear and likely varies by individual patient, dependent on a variety of factors in whom anticipated costs must be balanced with distinct patient risk. Ability for providers to modify preoperative patient counseling regarding expectations and potential alterations to care plans will carry direct implications for patient and family experience as well as patient-reported outcomes, an increasingly important consideration in modern healthcare delivery.
Finally, variable outcomes carry direct implications for reimbursement with increased LOS, readmissions, and complications associated with weighty financial consequences. In an era of ongoing healthcare reform, bundled care is among the proposed strategies to improve value and is being actively explored in selected settings. 27 By providing global reimbursement for a procedure and associated perioperative care, provider incentives are better aligned with quality; that is, limiting perioperative complications, LOS and readmissions. Hence, differentiating modifiable and nonmodifiable factors affecting these outcomes will be critical for patients, providers and healthcare systems.
Our study has limitations due to its retrospective nature within a single tertiary referral center. Therefore, findings may not be generalizable to all patient populations. In this study, we were unable to assess the impact of patient race because African American patients were under-represented in our study population, which might lead to bias. In addition, analysis of nonmodifiable variables was limited to those retained within our database. Further study will assist with evaluation of other nonmodifiable patient factors which may be relevant to patient outcomes. As noted, the nonmodifiable nature of some analyzed variables is uncertain. Receipt of intraoperative transfusion, for instance, can certainly be modified in some instances and is dependent on a number of factors that could not be assessed in this review.
Conclusion
Nonmodifiable patient factors including age, comorbidity and intraoperative transfusion account for additional variability in perioperative outcomes of patients with RC and may factor in the development of risk-adjustment, patient counseling and reimbursement models.