
Abstract
Background:
A marker of urothelial damage could be helpful for early detection and monitoring of local toxicity due to intravesical therapy for non-muscle invasive bladder cancer (NMIBC). The aim of the study was to investigate the correlation between fibronectin (FN) gene expression in bladder washings and local toxicity secondary to adjuvant intravesical therapy.
Materials and methods:
Patients undergoing adjuvant intravesical therapy for NMIBC and age-matched healthy patients were enrolled. Real time polymerase chain reaction was performed to analyze FN expression in bladder washings. Local toxicity was classified as: 0–1 mild (no medical therapy), 2 moderate (medical therapy and/or instillation postponed), 3 severe (discontinuation of therapy).
Results:
Seventy-two patients and 21 controls entered the study. A useful pellet was obtained in 58 patients and 18 controls. Intravesical Bacillus Calmette–Guerin (BCG), Epirubicin and Mitomycin C was offered to 69%, 13.8% and 17.2% of patients respectively. Compared with healthy controls (FN = 1.0 fold), overall median FN expression before adjuvant intravesical therapy was 1.73 fold [interquartile range (IQR) 0.8–2.3], while during therapy median FN expression increased to 3.41 (IQR: 1.6–6.1) fold. Considering 40 intermediate and high-risk patients undergoing intravesical BCG, median FN expression before adjuvant treatment was 1.92 [(IQR: 1.0–2.7) fold, increasing up to 4.1 (IQR: 1.9–6.6) during therapy. In more detail, FN increased during BCG therapy, showing a median expression of 4.22 (IQR: 2.2–5.5) and 6.16 (IQR: 2.6–8.7) fold in presence of grade 2 and 3 toxicity respectively, while remaining more or less stable in asymptomatic patients. After receiver operating characteristic curve analysis, FN value of 3.6 fold resulted, corresponding to 75% sensitivity and 69% specificity to predict grade 2–3 toxicity events (area under the curve 0.74, 95% confidence interval 0.63–0.85, p = 0.001).
Conclusion:
Our study validated the correlation between FN expression and urothelial damage. BCG seems to induce a urothelial activation with FN overexpression during adjuvant intravesical therapy. Grade of toxicity was related to FN expression.
Keywords
Introduction
The gold standard adjuvant treatment for intermediate and high-risk non-muscle invasive bladder cancer (NMIBC) is intravesical Bacillus Calmette–Guerin (BCG) immunotherapy. 1 In particular, current available literature highlights the role of BCG in delaying and potentially reducing the risk of tumor progression, especially when a maintenance schedule is offered. 2 Nevertheless, BCG is occasionally burdened by non-negligible local and systemic toxicity such as cystitis, gross hematuria, asthenia, and fever. 3 Whereas most of these symptoms are self-limiting and do not require specific treatments, in some cases they actually represent a significant risk for discontinuation of therapy. Indeed, up to 40% of patients with NMIBC will not complete the optimal treatment schedule due to the onset of local adverse events secondary to the urothelial damage. 4 As a result, in this setting oncologic outcomes could be undermined by interruption of appropriate induction and maintenance regimens.
In order to reduce the rate of patients who discontinue treatment due to side effects, early identification, prevention and effective management of treatment-related toxicity is essential to ensure oncologic efficacy and limit major urothelial damage. Nevertheless, to date we still need a repeatable, not-invasive marker which could timely predict urothelial suffering. Next-generation sequencing technologies and individualized clinical decision-making tools are developing a molecular landscape discovering novel predictive models5–7 and prognostic biomarkers.8–10 Fibronectin (FN) is a biomarker that, among many others, may select those patients more likely to fail their BCG schedule due to development of local toxicity. Indeed, FN is a large dimeric structural glycoprotein, an essential component of the extracellular matrix. 11 At urinary level, FN is involved in BCG attachment to bladder surface.12,13 Moreover, it has been shown that FN levels can increase due to the degradation of the extracellular matrix secondary to urothelial damage. To our knowledge, the levels of FN in NMIBC have never been evaluated after transurethral resection of bladder tumor (TURBT), during adjuvant therapy and during follow-up.
To address this unmet need, in this study we aimed to investigate the feasibility of sequential measurement of FN urothelial cell expression in bladder washing samples after TURBT of NMIBC and during and after adjuvant intravesical therapy. Moreover, we evaluated the predictive role of FN gene expression as a possible biomarker of early urothelial damage, correlating its levels with the different grades of local toxicity.
Materials and methods
Subjects and sample collection
After approval was obtained from the Institutional Review Board of Careggi Hospital (IEC 10166_bio), data from selected patients treated with TURBT plus adjuvant intravesical chemo- or immunotherapy for NMIBC and data from sex- and age-matched healthy controls were prospectively gathered from February 2016 to March 2017. Written informed consent was obtained from all participants before proceeding with enrollment. Demographic, clinical and pathological features were recorded.
According to World Health Organization grading of toxic drug effects and international recommendations for the prevention and management of intravesical therapy-associated adverse events, 14 local toxicity was classified as:
Grade 0: no local toxicity;
Grade 1: mild toxicity (no medical therapy and no changes in instillations schedule necessary);
Grade 2: moderate (medication support and/or suspension of instillations until resolution of symptoms);
Grade 3: severe (discontinuation of therapy).
Patients experiencing grade 2 toxicity were treated in the first instance with non-steroidal anti-inflammatory drugs and empirical antibiotic therapy, according to European Association of Urology (EAU) Guidelines. 1
Early instillation of Mitomycin C (40 mg diluted in 40 ml) was administered within 6 h after TURBT when indicated. Intravesical adjuvant chemotherapy (Mitomycin C 40 mg diluted in 40 ml or Epirubicin 80 mg diluted in 50 ml) and immunotherapy with BCG (RIVM-Medac, 50 mg diluted in 50 ml) were started within 4 weeks after TURBT. Patients at intermediate and high risk were all treated with intravesical BCG. Six weekly instillations were offered.
An explorative analysis on 27 subjects not included in the study population was performed before the beginning of the present study to better standardize the procedure. In particular, both urine and bladder washings were collected to determine the best specimen to complete FN gene expression analysis. Because of the excessive heterogeneity of urine and its frequent contamination undermining RNA quality, bladder washing was selected. Samples were collected by a Nelaton Ch 12 catheter performing two consecutive bladder washings with 50 ml of saline solution immediately before the first and the sixth instillation during induction, and at the time of the first 3-month cystoscopy. In the case of grade 2 or 3 toxicity, one or more additional samples of bladder washing were collected at the time of reported symptoms. Each sample was identified by a progressive number. The laboratory personnel and the biologists were blinded to clinical data and the urologists were not informed about the analysis results.
Sample processing
After collection, bladder washing samples were immediately stored in ice and then moved to a laboratory for sample processing. Samples were processed according to our previously described standard protocol 15 (Figure 1). In detail, bladder washings were centrifuged at 4°C for 10 min at 1500 rev/min and, after elimination of supernatant, washed in cold phosphate buffer saline solution and centrifuged once more. The cellular pellet retrieved was then collected and stored at −80°C until RNA extraction, performed using a miRNeasy Mini Kit (Qiagen®).
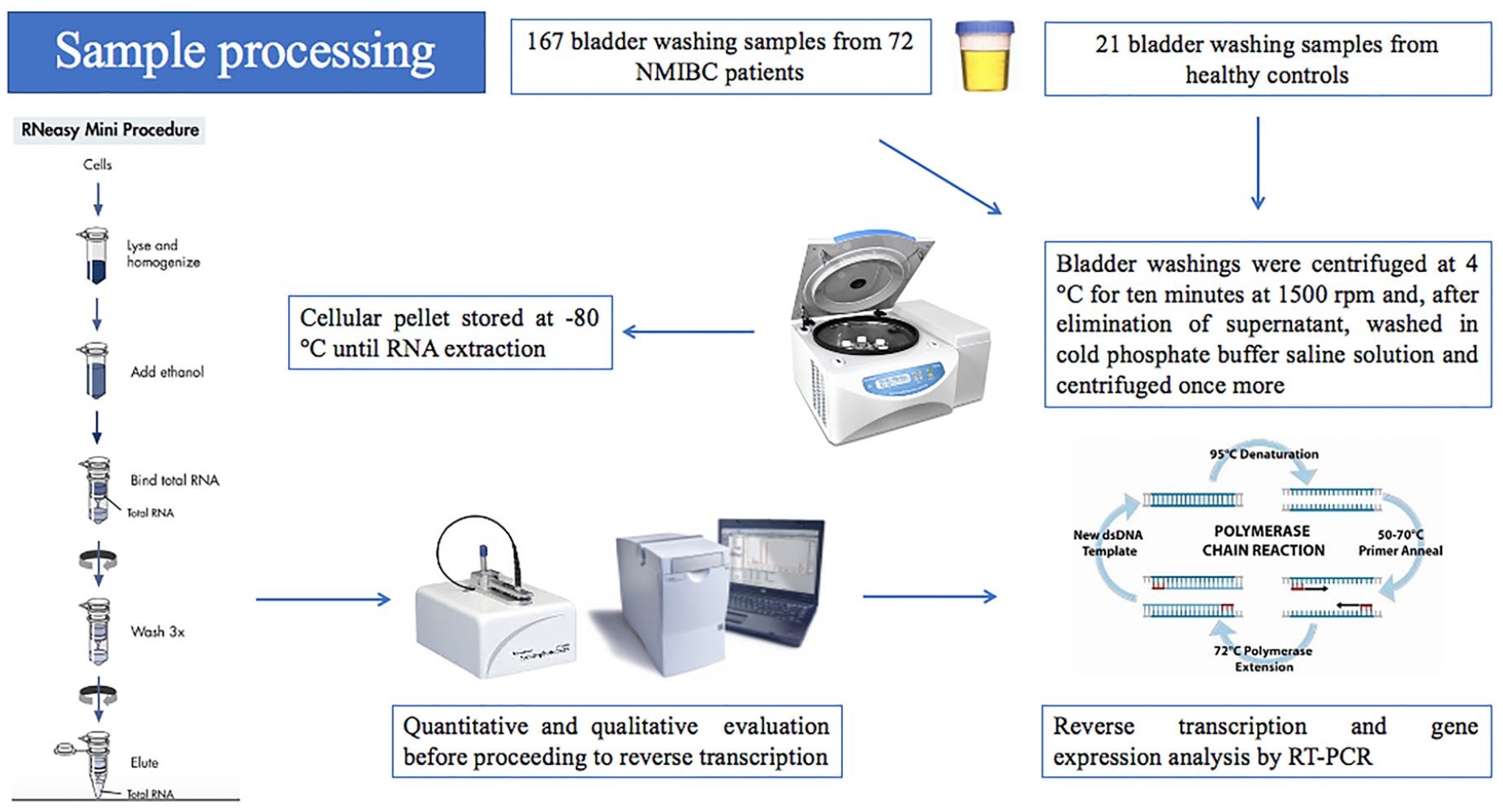
Samples processing according to our standardized standard protocol.
Before moving to reverse transcription to DNA, the extracted RNA had to fulfill definite quantitative and qualitative criteria, evaluated by a Nanodrop Spectrophotometer ND-2000. In particular, the concentration of RNA (500 ng/ml was the minimum required for the miRNeasy Mini kit), the degree of protein contamination and the degree of contamination from solvents and organic compounds were thoroughly checked. 16 Only good quality pellet samples proceeded to reverse transcription to DNA, while those not satisfying the above-mentioned standards were excluded from the final analyses. Reverse transcription was performed by “High Capacity cDNA Reverse Transcription Kit” (Life Technologies®) and the subsequent gene expression analysis was then performed by real time polymerase chain reaction (RT-PCR) using the coiled DNA obtained from reverse transcription. RT-PCR was accomplished according to the method of the comparative quantification (ΔΔCt), using cyclophilin as endogenous control. Moreover, every reaction was arranged in triplicate, as a further quality assurance. FN cell gene expression was calculated in folds of change as compared with the median value in healthy controls (considered equal to 1.0 fold).
Statistical analysis
First, descriptive statistics were obtained reporting medians [and interquartile ranges (IQRs)] for continuous variables, and frequencies and proportions for categorical variables, as appropriate. Continuous variables were compared by the Student independent t test or the Mann–Whitney U test based on their normal or not-normal distribution, respectively. Normality of variables’ distribution was tested by the Kolmogorov–Smirnov test. Differences between median FN values observed were compared using one-way analysis of variance test.
According to the presence and grade of local toxicity, patients were divided into two different groups (toxicity grade 0–1 versus 2–3). Receiver operating characteristic (ROC) curve analysis was performed in order to assess the best threshold value of FN to predict toxicity grade 2–3.
Multivariate logistic regression analysis to evaluate differential impact of tumor-related features and local toxicity on FN increase was performed, including the following co-variates: gender (male versus female), pT stage (Ta versus T1), presence of carcinoma in situ (CIS) no versus yes), tumor grade (low grade versus high grade), prior recurrence status (primary versus recurrent), number of tumors (single versus multiple), tumor size (<3 cm versus >3 cm), intravesical drug employed (Mitomycin C versus Epirubicin versus BCG) and local toxicity severity (grade 0–1 versus grade 2 versus grade 3). Discrimination threshold for non-significant versus significant FN increase was set using the area under the ROC curve.
The probability of survival was assessed by the Kaplan–Meier method, with the log-rank test (Mantel–Cox) used to estimate differences among levels of the analysed variables.
Statistical significance was set as p < 0.05. All tests were two-sided. Analyses were carried out using SPSS v. 24 (IBM SPSS Statistics for Mac, IBM Corp., Armonk, NY, USA).
Results
One-hundred and eighty-eight samples were collected from 72 patients and from 21 healthy controls. An adequate cellular pellet to perform FN expression analysis was obtained in 58 patients (80.5%) and 18 controls (85.7%) for a total of 156 samples. Tumor and bladder washings characteristics are reported in Table 1. Overall, Ta, T1 and primary CIS were reported in 22 (37.9%), 32 (55.2%) and four (6.9%) patients, primary in 30 (51.7%), recurrent in 28 (48.3%) respectively. CIS was synchronous in eight (13.8%) patients. Median tumor size was 1.6 cm (IQR 1.1–3.6).
Availability of adequate samples for fibronectin evaluation (a). Tumor related features in 58 patients treated with transurethral resection for bladder cancer and intravesical adjuvant therapy (b).

CIS, carcinoma in situ ; F, female; IQR, interquartile range; M, male.
With respect to the EAU prognostic risk classes, intravesical BCG, Epirubicin and Mitomycin C were offered to 40, 8, and 10 patients, respectively. Overall, the median FN expression was 1.73 (IQR: 0.8–2.3; p = 0.001), 3.41 (IQR: 1.6–6.1; p < 0.001) and 2.51 (IQR: 1.4–3.5; p < 0.001) folds of change compared with healthy controls before, during, and after adjuvant treatment, respectively. Considering 40 intermediate and high-risk patients undergoing intravesical BCG, median FN gene expression before adjuvant treatment was 1.92 (IQR: 1.0–2.7) folds increasing up to 4.1 (IQR: 1.9–6.6) during therapy and dropping to 2.9 (IQR: 1.2–3.9) folds at 3-month evaluation.
During adjuvant treatment, patients treated with BCG showed a median FN expression of 4.1 (IQR 1.9–6.6) as compared with 2.2 (IQR: 0.9–2.6) and 1.9 (IQR: 0.6–2.4) folds of change in patients treated with Mitomycin C and Epirubicin, respectively (p = 0.001). After adjuvant treatment, patients undergoing BCG adjuvant therapy had a median FN expression of 2.9 (IQR 1.2–3.9) compared with 1.8 (0.7–2.4) and 1.7 (0.5–2.3) folds of change in patients treated with Mitomycin C and Epirubicin, respectively (p = 0.001) (Table 2). Overall, 15 (25.9%), 8 (13.8%) and four (6.9%) patients reported grade 1, 2, and 3 toxicity, respectively. No grade 2–3 toxicity events were recorded among patients treated with intravesical chemotherapy. In more detail, FN gene expression was significantly raised up to a level of 4.22 (IQR: 2.2–5.5) and 6.16 (IQR: 2.6–8.7) folds in presence of grade 2 and 3 toxicity respectively, while slightly increasing in asymptomatic patients (median FN 2.32; IQR: 1.4–3.1; p < 0.001). FN gene expressions according to different adjuvant treatment schedules, local toxicity, and tumor-related features are reported in Table 2. At 3-month follow up visit, median FN gene expression decreased to 2.8 (IQR: 1.5–3.6), 3.3 (IQR: 1.9–5.9) and 2.0 (IQR: 0.9–3.3) folds of change in patients with grade 2 and 3 local toxicity and those not reporting local toxicity, respectively (p = 0.01) (Figure 2).
Median and interquartile range of fibronectin expression (folds of change) compared with age- and gender-adjusted controls observed in the whole cohort of 58 non-muscle invasive bladder cancer patients and in groups stratified according to adjuvant intravesical therapy offered (a), grade of toxicity (b), and tumor-related features (c).

p-Value was calculated on FN expression in patients versus healthy controls.
BCG, Bacillus Calmette–Guérin; CIS, carcinoma in situ; IQR, interquartile range; MMC, Mitomycin C.

Fibronectin gene expression according to grade of toxicity before, during, and after adjuvant therapy.
After ROC curve, FN value of 3.6 folds resulted, corresponding to a 75% sensitivity and 69% specificity to predict grade 2–3 toxicity events [area under the ROC curve 0.74, 95% confidence interval (CI) 0.63–0.85, p = 0.001] (Figure 3). At multivariable analysis, tumor size >3 cm [odds ratio (OR): 1.36, 95% CI 1.23–10.32, p = 0.02], adjuvant therapy with BCG (OR: 1.28, 95% CI 1.14, 7.32, p = 0.03), toxicity grade 2 (OR: 1.66, 95% CI 1.11, 4.65, p = 0.001) and grade 3 (OR: 2.12, 95% CI 1.24, 6.34, p = 0.001) were independently associated with a significant increase in FN during therapy (Table 3).
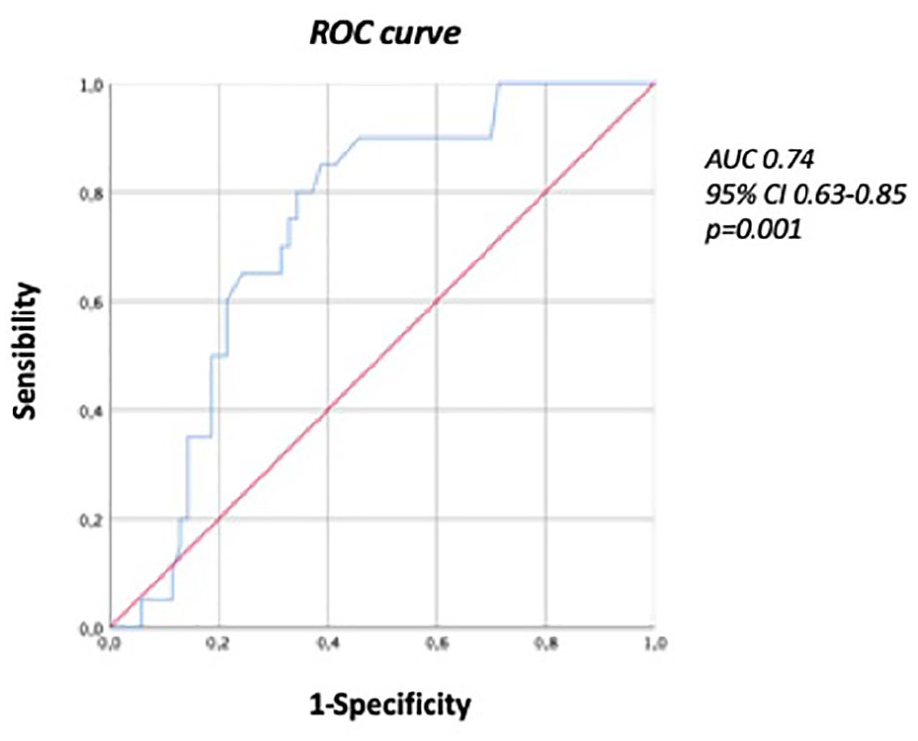
Area under the receiving operating characteristics curve to assess the best sensibility and specificity of fibronectin to predict toxicity grade 2–3.
Multivariable analysis exploring differential impact of tumor-related features and local toxicity on fibronectin increase.
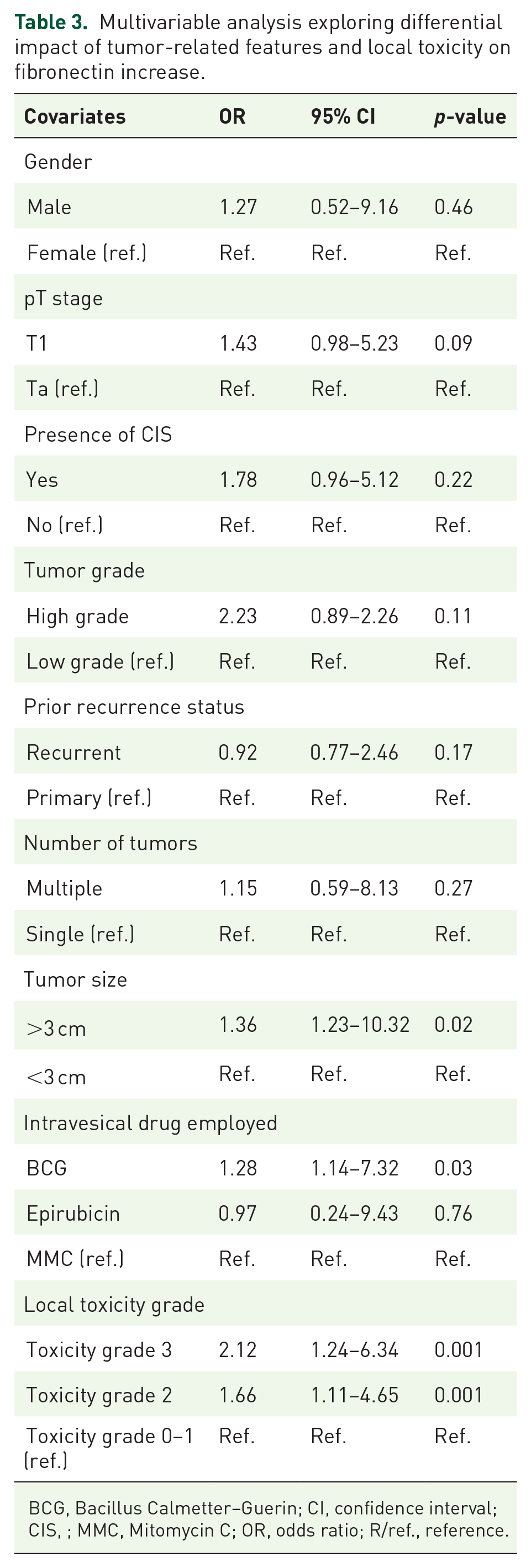
BCG, Bacillus Calmetter–Guerin; CI, confidence interval; CIS, ; MMC, Mitomycin C; OR, odds ratio; R/ref., reference.
At a median follow-up of 19 (IQR: 9–34) months, 14 (24.1%) patients showed disease recurrence. Patients experiencing toxicity grade 3, and thus discontinuing adjuvant therapy schedule, had a significantly lower recurrence-free survival compared with those experiencing toxicity grade 0–1 and 2 (25% versus 50% versus 78.4% respectively; p = 0.006) (Supplemental material Figure 1 online).
Discussion
Adjuvant intravesical chemo- or immunotherapy remains an important mainstay for patients affected by NMIBC since its use has been correlated with consistent reduction in the risk of bladder tumor recurrence and progression.1,17,18 However, a meaningful proportion of subjects will ultimately experience treatment-related adverse events which may prevent accomplishment of correct induction and maintenance schemes. As a result, prevention and management of side effects are pivotal to guarantee optimal oncologic outcomes. 19 In this regard, we still need a repeatable, non-invasive, reliable biomarker able to timely predict urothelial damage related to local toxicity during adjuvant intravesical therapy.
To the best of our knowledge, this is the first experience of exploring the feasibility and predictive role of sequential measurement of FN urothelial gene expression in bladder washing of NMIBC patients as a potential biomarker of early urothelial damage during adjuvant intravesical therapy. A key finding of our study is that a proper cellular pellet to assess FN expression was recovered in nearly 85% of patients’ and controls’ bladder washings, corroborating the feasibility of FN serial evaluation.
Not surprisingly, a significantly higher FN expression was confirmed in NMIBC patients, as compared with healthy controls. Indeed, FN represents the principal mesenchymal extracellular matrix glycoprotein implicated in cell adhesion, migration, and differentiation.11,20 FN is associated with tumorigenesis and progression in bladder cancer, 21 although the underlying mechanisms remain largely unknown. At the level of urinary tract, in the case of bladder tumor, levels of FN can rise due to the degradation of the extracellular matrix,22,23 with higher expression correlated with tumor stage and grade.24,25 Higher FN gene expression at the level urinary tract has already been associated with poorer outcomes after radical cystectomy. 26 Moreover, previous researches pointed out that the measurement of urine FN could be a potential diagnostic test for bladder cancer detection. 27
In our experience, we demonstrated that higher levels of FN can be found in bladder washings of NMIBC treated with intravesical adjuvant therapy due to urothelial damage related to local therapy, with significantly higher FN gene expression in patients undergoing adjuvant BCG, as compared with intravesical chemotherapy. In more detail, FN increased during BCG therapy up to a median gene expression of 4.22 and 6.16 folds of change during therapy in the presence of grade 2 and 3 toxicity. These findings strongly suggest that FN on bladder washing might represent an early marker of predictable local toxicity during adjuvant therapy after TURBT. Multivariable analysis confirmed that grade 2–3 local toxicity was the strongest factor independently associated with a significant FN increase during adjuvant therapy. Actually, also intravesical BCG and tumor size >3 cm resulted as independent predictors of FN rise during treatment schedule, albeit with lower odds. Conversely, tumor grade and stage were not independently associated with FN increase. This is in slight contrast with previous studies correlating FN expression with pathological features.22,24 One possible explanation could be that our study tried to analyze FN expression on the residual urothelium after TURBT, while the above-mentioned studies evaluated urinary FN with the bladder tumor still in place. Indeed, unlike tumor stage and grade, tumor size might correlate with FN increase due to a more extensive tumor resection, thus assuming a higher irritative damage involving the urothelium. Of note, tumor size was the only tumor-related feature showing a statistically significant difference in FN expression before first instillation. Taken together, our results suggest that FN expression by residual urothelium after TURBT might be more influenced by those factors intrinsically correlated with an irritative damage such a larger bladder resection, intravesical BCG, and, of course, severity of local discomfort during adjuvant therapy. On the contrary, in line with our multivariable model, tumor stage and grade might not necessarily predispose to increased bladder irritation. As such, their impact on FN increase during adjuvant therapy could be less important than previously thought.
In this light, FN gene expression promises to be a useful marker to (1) timely identify patients with reduced urothelial integrity due to local toxicity; (2) accurately quantify the degree of urothelial damage during adjuvant therapy; (3) confirm the restoration of the integrity of the urothelium at the end of intravesical therapy and (4) ensure the resumption of therapy without risk of further toxicity.
Indeed, early identification and potential prevention of side effects related to intravesical adjuvant therapy is an essential measure to increase the proportion of patients who can complete their treatment schedule. In this regard, a biomarker able to timely recognize local toxicity might help urologists to early treat local symptoms, ensuring lower rates of discontinuation therapy.
The present study was not devoid of limitations. First, the relatively small sample size might have undermined the final reliability of reported results. The numbers are too small to obtain definitive data on the correlation between FN behavior and patients’ discomfort during intravesical therapy but our preliminary results are encouraging and of clinical interest. Second, the laboratory method to obtain FN cell expression still appears to be quite elaborate and, as such, it might not be applicable to all center-related scenarios. Third, baseline urinary scores were not evaluated. This may have negatively influenced the trustworthiness of reported results, since baseline voiding symptoms could be related to the overall compliance of adjuvant treatment schedule.
Acknowledging these limitations, the current paper represents the first report to validate FN gene expression as a repeatable, non-invasive biomarker to timely recognize and objectively quantify the grade of local toxicity secondary to intravesical adjuvant treatment. Further translational studies with wider cohorts and with longer follow-up data will be needed to confirm our preliminary results.
Conclusion
In our experience, FN gene expression resulted as strictly related to the intensity of urothelial damage, reaching higher expression levels in the case of severe toxicity induced by intravesical therapy. In this regard, FN gene expression in bladder washings might represent an accurate marker of urothelial damage induced by adjuvant intravesical therapy.
Supplemental Material
sj-jpg-1-tau-10.1177_1756287221995683 – Supplemental material for Fibronectin urothelial gene expression as a new reliable biomarker for early detection of local toxicity secondary to adjuvant intravesical therapy for non-muscle invasive bladder cancer
Supplemental material, sj-jpg-1-tau-10.1177_1756287221995683 for Fibronectin urothelial gene expression as a new reliable biomarker for early detection of local toxicity secondary to adjuvant intravesical therapy for non-muscle invasive bladder cancer by Fabrizio Di Maida, Cristina Scalici Gesolfo, Riccardo Tellini, Andrea Mari, Chiara Sanfilippo, Luca Lambertini, Antonio Andrea Grosso, Marco Carini, Andrea Minervini and Vincenzo Serretta in Therapeutic Advances in Urology
Footnotes
Acknowledgements
We would like to thank GSTU (Gruppo Studio Tumori Urologici) Foundation for their administrative, material and technical support.
Authors’ contributions
Conception and design, F.D.M. and V.S.; Acquisition of data, C.S.G., R.T., L.L. and A.A.G.; Analysis and interpretation of data, F.D.M., A.M. and V.S.; Statistical analysis, F.D.M. and C.S.; Drafting of the manuscript, F.D.M. and C.S.G.; Critical revision of the manuscript, A.M., M.C. and A.M.; Supervision, A.M. and V.S.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.