
Abstract
Management of carcinoma in situ of the bladder remains a complex and challenging endeavor due to its high rate of recurrence and progression. Although it is typically grouped with other nonmuscle invasive bladder cancers, its higher grade and aggressiveness make it a unique clinical entity. Intravesical bacillus Calmette-Guérin is the standard first-line treatment given its superiority to other agents. However, high rates of bacillus Calmette-Guérin failure highlight the need for additional therapies. Radical cystectomy has traditional been the standard second-line therapy, but additional intravesical therapies may be more appealing for non-surgical candidates and patients refusing cystectomy. The subject of this review is the treatment strategies and available therapies currently available for carcinoma in situ of the bladder. It discusses alternative intravesical treatment options for patients whose condition has failed to respond to bacillus Calmette-Guérin therapy and who are unfit or unwilling to undergo cystectomy.
Keywords
Introduction
In 2015, there are an estimated 74,000 new cases of bladder cancer worldwide and 16,000 deaths (http://www.cancer.org/cancer/bladdercancer/detailedguide/bladder-cancer-key-statistics). A majority of urothelial cell carcinoma (UCC) of the bladder will have nonmuscle-invasive disease, which is usually associated with excellent prognosis. However, carcinoma in situ (CIS) is a type of nonmuscle-invasive bladder cancer (NMIBC) that is of higher grade and increases the risk of recurrence and progression. At diagnosis, approximately 10% of patients with bladder cancer present with CIS [Kirkali et al. 2005]. It is a flat, high-grade, and aggressive UCC that carries a risk of subsequent metastasis. Within 5 years of diagnosis, 40–60% of patients develop invasive disease with an average risk of progression of 54% among studies [Utz et al. 1970; Stanisic et al. 1987; Lamm et al. 1998]. However, after intravesical bacillus Calmette-Guérin (BCG) therapy, a decrease in risk of progression to 9.8% has been reported in patients with CIS (p = 0.001) [Sylvester et al. 2002].
The management of CIS continues to present with many challenges. Although intravesical BCG has been accepted as first-line therapy per the American Urological Association (AUA) and European Association of Urology (EAU) guidelines [Hall et al. 2007; Babjuk et al. 2013], this can be complicated by recurrence and progression. The AUA and EUA guidelines also recommend radical cystectomy (RC) as second-line treatment, as other therapies are considered oncologically inferior at this time [Hall et al. 2007; Babjuk et al. 2013]. But there is increasing data for the multitude of developments in intravesical therapies for BCG failure in nonsurgical candidates, which are summarized in Table 1. This review focuses on the management of CIS of the bladder and recent developments for treatment.
Intravesical therapies for CIS of the bladder.

BCG, bacillus Calmette-Guérin; CIS, carcinoma in situ; IFN, interferon, MCNA, Mycobacterium phlei cell wall nucleic acid complex; MMC, mitomycin C.
Bacillus Calmette-Guérin
BCG is an attenuated strain of Mycobacterium bovis that was developed in 1906 and was administered as a vaccine to prevent tuberculosis by 1921. Attempts to use BCG as therapy for various cancers began in the 1970s, including acute lymphoblastic leukemia and melanoma [Mathe et al. 1969; Morton et al. 1974]. The mechanism of action of BCG remains incompletely understood but is thought to involve immune activation [Redelman-Sidi et al. 2014]. After intra-vesical administration, BCG is internalized by urothelial cells, triggering a cascade of cytokine production, including interleukin (IL)-1, 2, 6, 8, tumor necrosis factor, interferon (IFN)-γ, and granulocyte macrophage colony-stimulating factor (GM-CSF). Immune cells such as neutrophils, macrophages, dendritic cells, and CD4+ lymphocytes are subsequently recruited to the site, resulting in cytotoxicity to bladder cancer cells.
Intravesical BCG therapy
Intravesical BCG has been shown to be effective against CIS and is recommended as first-line therapy in the AUA and EAU guidelines [Hall et al. 2007; Babjuk et al. 2013]. The role and efficacy of BCG induction plus maintenance therapy for treatment of CIS was determined by the Southwest Oncology Group (SWOG) 8507 trial [Lamm et al. 2000]. This was a prospective and randomized trial comparing induction BCG therapy with induction plus maintenance therapy in CIS and high-grade NMIBC. Treatment would begin at least 1 week following tumor resection with weekly treatments for a total of 6 weeks for the induction course. Maintenance BCG was scheduled with sets of three successive weekly treatments at 3 months, 6 months, and every 6 months to 3 years from the start of induction therapy. In patients with CIS, there was no difference in complete response rates at 3 months after induction therapy (56.9% versus 54.7%) between the no maintenance and maintenance arms, respectively (p = 0.8). At 6 months, however, the complete response rate increased to 83.8% in the maintenance arm and 68.1% in the no maintenance arm (p = 0.004).
In addition, a meta-analysis of randomized trials comparing risk of progression in NMIBC showed a decreased risk of progression of CIS after BCG therapy [Sylvester et al. 2002]. The endpoint was defined as progression to T2 disease or higher, lymph node or distant metastasis. Although the risk for progression was low for CIS at 13.9%, BCG treatment reduced progression to 9.8% (p = 0.001). Interestingly, only patients receiving maintenance BCG benefited and there was no difference in treatment effect for overall or disease-specific survival.
Furthermore, intravesical BCG has been shown to be superior to intravesical chemotherapy. This was reviewed in a meta-analysis of nine randomized trials comparing intravesical BCG with intravesical chemotherapy in patients with CIS [Sylvester et al. 2005]. Intravesical chemotherapy agents included mitomycin C, epirubicin, and adriamycin. Of 298 patients on BCG, 68.1% had a compete response compared with 51.5% of patients on chemotherapy at 3- or 6-month follow up. Forty-seven percent of patients receiving BCG also had no evidence of disease at a median follow up of 3.6 years compared with 26% of patients on chemotherapy. Among complete responders, there was a reduction of 53% in the odds of recurrence on BCG [odds ratio 0.47, 95% confidence interval (CI) 0.31–0.73, p = 0.0008]. It is also important to note that BCG appeared to be superior only in the trials in which maintenance BCG was given.
Maintenance BCG can come at a price due to its long treatment course and significant associated toxicity. The SWOG 8507 trial reported only a 16% completion rate of the full 3-year course [Lamm et al. 2000]. The withholding of maintenance treatment was typically due to side effects such as severe or prolonged dysuria, fever, or malaise. Therefore, there have been studies investigating the added benefit of maintenance BCG [Herr et al. 2011]. A large cohort of 816 patients with noninvasive bladder cancer from Memorial Sloan-Kettering Cancer Center receiving BCG without maintenance was found to compare favorably with trials in which comparable patients received maintenance therapy. The 2- and 5-year recurrence-free rate was 76% and 49%, respectively. However, there was an emphasis placed on repeat resections with fulguration of all disease and evaluation at 6 months after induction therapy.
Another strategy that has been investigated by the European Organization for Research and Treatment of Cancer (EORTC) to optimize efficacy of BCG while minimizing toxicity is to administer treatments at a lower dose. A recent randomized controlled noninferiority trial compared the efficacy of one-third dose with full-dose BCG therapy in a 1-year or 3-year course [Oddens et al. 2013]. In contrast to SWOG 8507, 35.2% of patients completed a 3-year course of full-dose BCG in the EORTC trial. There was no difference in toxicity between one-third dose and full strength, and interestingly, there was also no difference in progression (p = 0.85) or survival rates (p = 0.56) in any of the treatment arms. However, the 3-year course of full-dose BCG was found to be more effective in high-risk patients than a 1-year course (p = 0.0087). This is important to note as CIS is classified as high-risk disease. Therefore, 3-year maintenance therapy remains the standard of care.
Predicting response to intravesical BCG has been limited as validated markers are currently unavailable. A few studies have investigated the role of urine cytokines following therapy [Saint et al. 2002; Watanabe et al. 2003; Videira et al. 2009]. In addition, biomarkers such as Ki-67 and p53 have also been investigated as potential prognostic markers for BCG success [Zlotta et al. 1999]. Prediction of BCG response has also been proposed using correlation of pretreatment immunologic tumor microenvironment to treatment success. Given that BCG is expected to trigger a T-helper 1 (Th1) response, a study demonstrated that tumors with a preexisting Th2 response and without a Th1 response would most benefit from BCG therapy [Nunez-Nateras et al. 2014].
BCG failure
It has been reported that over 50% of patients receiving BCG treatments will not be disease free and deemed to ‘fail’ BCG [Sylvester et al. 2005]. BCG failure is technically described as recurrence of tumor after BCG therapy. However, this definition is complicated by the fact that failure comes in many forms with different implications regarding therapy options and prognosis. There have been attempts to classify BCG failure to provide a framework for management. O’Donnell and colleagues stratified the definition into four categories [O’Donnell, 2007]: BCG intolerance; BCG resistance; BCG relapsing; BCG refractory.
BCG intolerance refers to recurrence after an incomplete course of therapy shortened by serious adverse events or symptomatic intolerance. This is typically recurrent disease in the setting of inadequate BCG treatment due to drug toxicity and can occur during induction or maintenance. The most common toxicities encountered include dysuria, fevers, and malaise [Lamm et al. 1995]. It has been reported that only 32.7% complete a full 3-year treatment course with 20.3% stopping treatment due to toxicity [Van der Meijden et al. 2003].
BCG resistance is defined as recurrence or persistence at 3 months from therapy and with resolution of disease at 6 months from BCG retreatment. It has been found that 6 months post-induction is the minimum treatment period to identify high-risk tumors as truly refractory. In a cohort of 93 patients, Herr and Dalbagni found that patients with tumor present at 6 months have a higher rate of failure at 24 months compared with having tumor present at 3 months (p = 0.0001) [Herr and Dalbagni, 2003].
Patients are defined as having BCG-relapsing disease when there is recurrence after achieving a complete response at 6 months after treatment. They can be further classified as early relapse (within 12 months of treatment), intermediate relapse (within 12–24 months of treatment), and late relapse (over 24 months after treatment).
The disease is considered BCG refractory when there is absence of complete response by 6 months after BCG induction. This also includes progression of disease by 3 months after the first cycle of BCG. BCG-refractory is suggested to have worse outcomes than BCG-relapsing disease. In a prospective cohort multi-institutional study of 32 patients, patients with BCG-refractory disease receiving mycobacterial cell wall DNA complex instillations had progression-free survival of 18 months. Patients with BCG-relapsing disease who received another induction of BCG therapy had a progression-free survival of 52 months (p = 0.001) [Herr et al. 2015].
Recently, a molecular definition of BCG failure has been introduced to enhance clinical trial designs for NMIBC [Kamat et al. 2015]. This incorporates fluorescence in situ hybridization (FISH) testing to predict BCG failure. A total of 143 patients were followed for 2 years during intravesical BCG therapy. Patients with a positive FISH test at 3 months were more likely to develop tumor recurrence (p < 0.001). The authors concluded that a positive early FISH test and negative 3-month cystoscopy results can be considered to have molecular BCG failure.
Second-line intravesical therapy
Although these classifications can be helpful, it is ultimately up to the urologist who determines whether ‘BCG failure’ has occurred. Before consideration of additional therapy, the upper tracts and the prostatic urethra must also be ruled out as possible sites of disease [Merz et al. 1995; Huguet et al. 2005; Giannarini et al. 2014]. Huguet and colleagues highlighted the importance of tumor involvement of the prostatic urethra [Huguet et al. 2005]. Five-year disease-specific survival in high-risk NMIBC was found to be 20% in patients with prostatic urethral tumor involvement compared with 78% survival in patients without prostatic urethral involvement (p < 0.0002).
After the decision has been made to pursue additional non-BCG therapy, there are additional factors to consider in determining who should receive more intravesical therapy. Appropriate candidates may include patients who are poor surgical candidates with significant medical comorbidity or advanced age, or those who refuse cystectomy despite understanding of the risks involved. In addition, patients whose disease recurs long after having a complete response to BCG treatment (>2 years), had recurrence with low-grade disease or minimal high-grade disease, or still at a relatively early treatment period may also be considered for additional intravesical options.
Valrubicin
Valrubicin is the only US Food and Drug Admin-istration (FDA)-approved agent for BCG-refractory CIS of the bladder. It is a derivative of the anthracycline doxorubicin that rapidly penetrates cell membranes and has antineoplastic activity through its effect on nucleic acid metabolism [Greenberg et al. 1997].
Its use in patients with BCG-refractory CIS was investigated in a phase I–II trial [Greenberg et al. 1997]. A dose of 200–900 mg valrubicin was instilled intravesically every week for 6 weeks. Systemic absorption and toxicity was found to be minimal. Thirteen out of 32 patients (41%) achieved a complete response. FDA approval was based on a pivotal phase III trial that included 90 patients with CIS despite multiple courses of intravesical therapies [Steinberg et al. 2000]. Complete response was found in 21% of patients. At last evaluation (30 months mean follow up), 8% remained disease free while 79/90 (88%) had recurrence with 56% undergoing eventual cystectomy. Only two patients had recurrence with progression to T2 disease. A subsequent trial also demonstrated effectiveness in BCG failure. In a phase II/III open-label study of 80 patients, complete response was 18% at 6 months with 25% of overall patients eventually undergoing cystectomy [Dinney et al. 2013b]. In addition, a recent multicenter retrospective review of valrubicin use in BCG-refractory CIS provided a good description of therapy in actual clinical practice [Cookson et al. 2014]. In this study, there was a 6-month disease-free rate of 30% after valrubicin. Cystectomy after therapy was also reduced in this study (13%) compared with prior studies. So although valrubicin does show some effectiveness in cases of BCG failure, it is mainly an option for those unable to tolerate cystectomy.
Intravesical BCG plus IFNα
Prior investigators have reported use of BCG and Interferon alpha (INFα) therapy after BCG failure and have shown a 50–60% complete response rate [Luciani et al. 2001; Lam et al. 2003; Punnen et al. 2003]. In a subsequent large phase II trial on this combination therapy, 45% of patients with BCG failure and 59% of patients naïve to BCG remained disease free at a median of 24-month follow up [Joudi et al. 2006]. Unfavorable factors that were significant for recurrence after BCG and INFα therapy included multifocality, large size (>5 cm), presence of T1, and prior BCG failure more than once [Joudi et al. 2006; Rosevear et al. 2011].
However, combination therapy with INFα should not be used as first-line therapy as it has not been shown to be effective. A multicenter, prospective study randomized 670 patients who were BCG naïve with NMIBC to receive BCG or BCG plus INFα. At 24-month median follow up, there was no difference in recurrence-free survival between the two groups [Nepple et al. 2010]. There is also limited efficacy for CIS after two BCG failures and it is important to note that patients with significant unfavorable risk factors mentioned earlier are most difficult to deal with, as combination therapy with INFα is the least effective.
Intravesical gemcitabine
Intravesical gemcitabine is a pyrimidine analog that has shown efficacy against BCG failure in high-risk NMIBC [Di Lorenzo et al. 2010]. In a phase II trial of 30 patients with NMIBC refractory to BCG therapy, 50% achieved a complete response with a median follow up of 19 months. However, this was not shown to be durable as only 2/30 (7%) maintained complete response at 23 and 29 months, respectively [Dalbagni et al. 2006]. In a subsequent SWOG phase II trial for gemcitabine in recurrent NMIBC after two prior courses of BCG, 28% and 21% of 47 patients were disease free at 1 and 2 years, respectively, with CIS present in 60% of patients [Skinner et al. 2013]. This is comparable to the complete response rates of 18–21% in prior valrubicin studies, suggesting that gemcitabine may be a suitable alternative [Steinberg et al. 2000; Dinney et al. 2013b].
Intravesical taxane and mycobacterial cell wall extract
Docetaxel is a cytotoxic chemotherapy agent that has shown potential in BCG failure in a phase I trial [Mckiernan et al. 2006]. This trial enrolled 18 patients whose condition had failed to respond to two courses of BCG or BCG plus INFα. Fifty-six percent of patients had no evidence of disease at post-treatment cystoscopy and biopsy with minimal toxicity. Barlow and colleagues reported their experience of intravesical docetaxel after BCG failure [Barlow et al. 2013]. With a median follow up of 39 months, 32 of 54 (59%) patients had a complete response after induction therapy with 25% recurrence-free survival at 3 years. Fifty-four percent of these patients had a history of CIS and 83% had a history of high-grade disease.
Paclitaxel is a taxane-type agent with potential neoplastic activity when bound to albumin. A phase I study in recurrent high-grade NMIBC after failure of at least one standard intravesical regimen showed that nanoparticle albumin-bound paclitaxel had increased solubility and lower toxicity compared with docetaxel [Mckiernan et al. 2011]. A subsequent phase II trial showed a 35.7% complete response rate in a cohort of 28 patients with NMIBC and previous BCG failure [Mckiernan et al. 2014].
Cell wall extract from Mycobacterium phlei has shown antineoplastic activity after BCG failure. A total of 55 patients underwent weekly intravesical emulsified M. phlei cell wall DNA complex instillations. All but three patients had a history of CIS. A total of 62%, 49%, and 41% of patients had a complete response at 3, 6, and 13 months, respectively [Morales et al. 2009]. A subsequent multicenter open-label single-arm study was performed using M. phlei cell wall nucleic acid complex [Morales et al. 2015]. Of 129 patients, 91 patients had CIS with most of the patients having disease that failed to respond to prior BCG therapy. Disease-free survival was 25% and 19% at 1 and 2 years, respectively. Progression-free survival rate was evaluated and found to be 87.3%, 79.8%, and 77.7% at 1, 2, and 3 years, respectively.
Studies on intravesical taxanes and M. phlei extracts are limited with small treatment arms. Additional studies are necessary in the future to determine the ideal treatment schedule and efficacy.
Electromotive and hyperthermic therapy with mitomycin C
Electromotive drug administration is based on the enhancement of intravesical chemotherapy transport with a current gradient between the drug and bladder wall. Acceleration of mitomycin C (MMC) transport with electromotive therapy was investigated in a prospective randomized study [Di Stasi et al. 2003]. A total of 108 patients with CIS were randomized to three arms after transurethral resection and multiple biopsies: electromotive MMC instillation, passive MMC instillation, or BCG instillation. Complete response at 6 months was observed in 31% of passive MMC patients, 58% of electromotive MMC patients, and 64% of BCG patients. A subsequent randomized controlled trial investigated the comparison of BCG alone with sequential BCG and electromotive MMC for high-risk NMIBC [Di Stasi et al. 2006]. Patients received either induction BCG or BCG for 2 weeks followed by three cycles of weekly electromotive MMC. In 212 patients, the disease-free survival was 69 months versus 21 months in BCG plus electromotive MMC and BCG alone, respectively. Recurrence was also significantly lower in BCG plus electromotive MMC than BCG alone at 41.9% versus 57.9%, respectively. In addition, with the recent announcement of BCG shortage, electromotive MMC has emerged as a potential alternative to intravesical therapy [Mostafid et al. 2015]. Although this is an option in Canada and other countries, it is not currently available in the United States.
Hyperthermic therapy is typically done with the Synergo system, in which an intravesical microwave applicator is used to provide hyperthermia to the urothelium. It is used in combination therapy with MMC and is thought to improve MMC efficacy due to direct cytotoxic effect from hyperthermia and increasing drug permeability [Paroni et al. 2001; Van der Heijden et al. 2004]. There have been reports of hyperthermic therapy with MMC after BCG failure, but they have been inconsistent with heterogenous results [Van der Heijden et al. 2004; Alfred Witjes et al. 2009; Halachmi et al. 2011]. Furthermore, electromotive therapy and hyperthermic therapy with MMC are both relatively unknown in the USA and reports are largely from Europe.
Radiation therapy
Radiation therapy has been proposed as an option for high-grade NMIBC. Weiss and colleagues followed 141 patients with high-risk T1 bladder cancer treated with radiation therapy or platinum-based chemoradiation therapy [Weiss et al. 2006]. Persistent disease and tumor recurrence after complete response at 5 and 10 years was 49% and 64%, respectively for this cohort. Forty-eight of these patients also had associated CIS and were found to have no difference in complete response or recurrence compared with patients without CIS. In addition, a multicenter randomized trial was conducted with radiotherapy in patients with high-grade T1 bladder cancer [Harland et al. 2007]. In this study, 133 of 210 patients were diagnosed with multifocal disease or CIS. In this subgroup, patients were randomized to intravesical therapy or radiotherapy and found no difference in progression-free survival (p = 0.78) or overall survival (0.193).
Combination intravesical therapy
Multiagent chemotherapy is typically standard in most cases of systemic chemotherapy, but has not been widely described in intravesical chemotherapy. A multi-institutional retrospective study reported their experience with combination intravesical chemotherapy in a series of 47 patients [Lightfoot et al. 2014]. These patients underwent 6 weekly treatments of sequential intravesical gemcitabine and MMC chemotherapy. Ten of 47 patients were BCG naïve due to a history of high-dose immunosuppression. At 1- and 2-year follow up, 48% and 38% were recurrence free. A retrospective review of 27 patients at a single institution also underwent sequential intravesical gemcitabine and MMC chemotherapy for BCG failure and found a complete response of 37% at a medium follow up of 22 months [Cockerill et al. 2015].
A randomized prospective trial reported their experience with sequential combination of MMC and BCG in NMIBC [Solsona et al. 2015]. This trial was conducted with 407 patients randomized to receiving MMC followed by BCG versus receiving BCG alone. The disease relapse rate was decreased from 33.9% to 20.6% with significantly improved disease-free interval in sequential combination therapy (hazard ratio 0.57, 95% CI 0.39–0.83, p = 0.003). However, combination therapy resulted in higher toxicity, with a 17% increase in grade 3 toxicity (p < 0.001).
Furthermore, a recent study published their initial experience with sequential intravesical gemcitabine and docetaxel in a series of 45 patients with NMIBC [Steinberg et al. 2015]. With a median follow up of 15 months, 54% of patients had no bladder cancer recurrence at 1 year and 34% at 2 years.
Radical cystectomy
Currently, it is not clear whether delayed radical cystectomy (RC) after failed BCG therapy results in differences in overall survival compared with immediate cystectomy in CIS of the bladder [De Jager et al. 1991; Hassan et al. 2004; Cheng et al. 1999]. Therefore, RC is accepted as a second-line therapy for CIS after intravesical BCG [Hall et al. 2007; Babjuk et al. 2013]. But the decision to proceed is often complicated by many factors such as its morbidity, patient comorbidities, and socioeconomic issues.
The decision process to undergo RC is often difficult for patients and physicians and is especially true regarding its timing. However, there are criteria that have been proposed in determining which patients should undergo a timely cystectomy. These include patients with rapid relapsing or refractory disease (<6 months), T1 disease on repeat transurethral resection, high-volume multifocal high-grade disease, presence of lymphovascular invasion with T1 disease, unfavorable or mixed histology (e.g. micropapillary disease), and poor patient compliance [Chang and Cookson, 2005].
The rationale for timely cystectomy in NMIBC has largely been due to balancing the risks of understaging and progression. It has been reported in some series that primary CIS may be understaged at the time of cystectomy in over 30% of patients [Huang et al. 2009; Tilki et al. 2010]. The aggressiveness of CIS has been demonstrated in other studies and progression has not been minimal. In a series of 86 patients with NMIBC, 53% of patients had disease progression after BCG therapy and 36% underwent eventual RC within 15 years [Cookson et al. 1997]. Furthermore, outcomes for patients with pathologic CIS and T1 have been very favorable. The 10-year disease-free survival rates have been reported to be up to 90% [Bianco et al. 2004; Hassan et al. 2004; Shariat et al. 2006; Zehnder et al. 2014].
There are many studies that investigated the potential survival benefit of avoiding the delay of RC. It has been shown that cystectomy delay from initial bladder cancer diagnosis in muscle-invasive disease leads to poorer outcomes [Chang et al. 2003; May et al. 2004; Lee et al. 2006]. This remains true for high-risk nonmuscle-invasive disease [Herr and Sogani, 2001]. Herr and Sogani compared outcomes in early versus delayed RC in a series of 90 patients who underwent eventual cystectomy after failed transurethral resection and BCG therapy [Herr and Sogani, 2001]. Thirty-five of these patients underwent cystectomy for recurrent nonmuscle-invasive tumors. They report a survival of 92% if RC was within 2 years of initial BCG therapy and 56% survival if RC was after 2 years (p = 0.03). In addition, 55 patients underwent RC due to progression to invasive disease. In this subgroup, 41% of patients survived if RC was within 2 years of initial BCG compared with 18% survival if RC was after 2 years (p = 0.04).
Although it may seem clear to undergo timely RC in many patients with BCG failure, there are caveats to consider in noninvasive disease. As physicians balance risks of under-treatment in understaged patients, the potential for overtreatment must also be considered. In addition, RC continues to be associated with significant morbidity and should not be considered lightly as potential treatment [Stimson et al. 2010]. This is especially true in patients with significant comorbidities and often makes radical treatment contraindicated [O’Donnell, 2007]. Furthermore, there is also a subgroup of patients who simply refuse RC in order to avoid lifestyle consequences of surgery [O’Donnell, 2007].
Clinical trials
For patients whose condition has failed to respond to BCG therapy and have exhausted second-line intravesical therapies, clinical trials remain a viable option for those who remain poor cystectomy candidates or simply refuse RC. Novel approaches for treatment currently explored include cytotoxic agents, gene therapy, vaccine-based therapy, and nanoparticle-based delivery systems. These respective trials for CIS of the bladder are summarized in Table 2.
Clinical trials for CIS of the bladder.
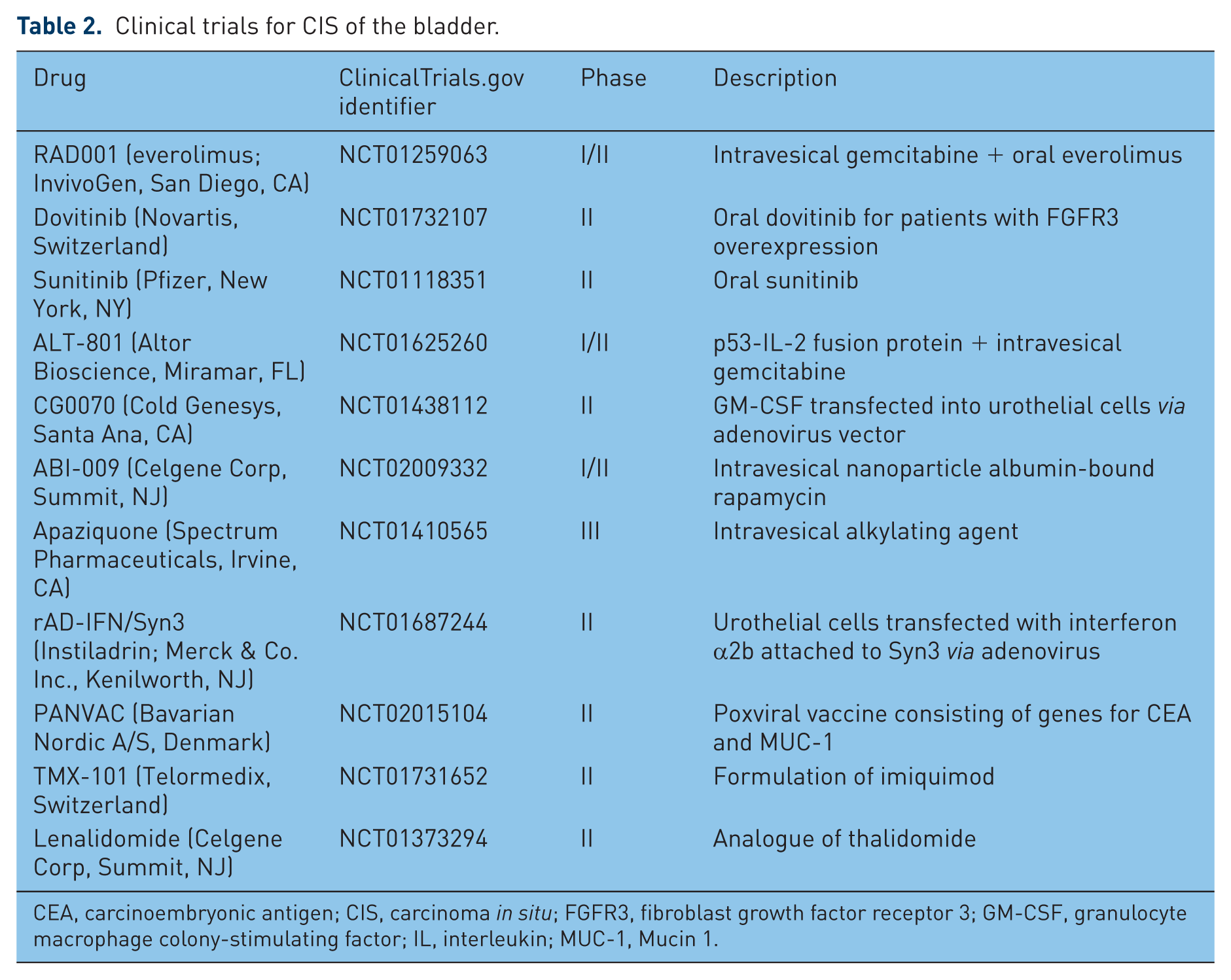
CEA, carcinoembryonic antigen; CIS, carcinoma in situ; FGFR3, fibroblast growth factor receptor 3; GM-CSF, granulocyte macrophage colony-stimulating factor; IL, interleukin; MUC-1, Mucin 1.
RAD001 (everolimus) is an inhibitor of mammalian target of Rapamycin (mTOR) that plays a key role in controlling cancer growth. A study investigated the effects of incubating everolimus and gemcitabine either alone or in combination in two human bladder cancer cell lines. The combination of everolimus and gemcitabine significantly reduced proliferation of bladder cancer cells compared with either agent alone [Pinto-Leite et al. 2012]. This led to a phase I/II study of oral everolimus and intravesical gemcitabine in BCG-refractory CIS of the bladder currently in progress [ClinicalTrials.gov identifier: NCT01259063].
Dovitinib is an oral multitargeted tyrosine kinase inhibitor that binds fibroblast growth factor receptor 3 (FGFR3) among others. It has been reported that FGFR3 overexpression has been found in approximately 50% of muscle-invasive bladder cancers [Tomlinson et al. 2007]. This led to a phase II trial of oral dovitinib in advanced bladder cancers, but was terminated after determining there was limited activity in patients regardless of FGFR3 mutation status [Milowsky et al. 2014]. However, a phase II trial of dovitinib is currently underway in patients with BCG refractory NMIBC with FGFR3 mutations or overexpression [ClinicalTrials.gov identifier: NCT01732107]. Sunitinib is another tyrosine kinase inhibitor that is also being investigated in a phase II trial in patients with BCG-refractory NMIBC [ClinicalTrials.gov identifier: NCT01118351].
ALT-801 is a p53-IL-2 fusion protein that targets cancer cells that overexpress p53. A recent phase I study of ALT-801 monotherapy in metastatic malignancies indicated it was well tolerated when given daily for two 4-day cycles [Fishman et al. 2011]. This drug is currently being tested in a phase I/II trial in combination with gemcitabine for patients with BCG failure [ClinicalTrials.gov identifier: NCT01625260].
Apaziquone is an alkylating agent that has potential antitumor activity versus bladder cancer cells. Apaziquone is activated by deoxythymidine diaphorase, an enzyme that is preferentially expressed in bladder cancer cells, providing targeted therapy. In a phase II study, 34.7% and 44.9% of patients showed recurrent tumors at 12 and 18 months, respectively. Progression to muscle-invasive disease was observed in only one patient [Hendricksen et al. 2012]. A phase III trial is underway investigating multiple instillations as adjuvant therapy [ClinicalTrials.gov identifier: NCT01410565].
Recombinant adenovirus-mediated IFNα2b protein (rAD-INFα) attached to SCH 209702 (Syn3) has been shown to enhance the rate of adenoviral-mediated intravesical delivery [Benedict et al. 2004; Nagabhushan et al. 2007]. A subsequent phase I trial involving 17 patients demonstrated minimal adverse effects as the drug was well tolerated [Dinney et al. 2013a]. A subsequent phase II trial is underway to assess the efficacy of rAD-INFα with Syn3 given intravesically in patients with BCG-refractory NMIBC [ClinicalTrials.gov identifier: NCT01687244].
CG0070 is a recombinant adenovirus that leads to GM-CSF expression, resulting in antitumor activity [Ramesh et al. 2006]. A phase I trial of 35 patients showed high levels of GM-CSF and CG0070 genomes detected in urine [Burke et al. 2012]. Although complete response rate was found to be 48.6% at 10.4 months, it should be noted that it was not designed to investigate efficacy. A phase II/III trial is currently underway investigating the efficacy of GC0070 in patients with CIS whose condition has failed to respond to BCG [ClinicalTrials.gov identifier: NCT01438112].
Nanoparticles are small molecules that interact with the urothelium and promote drug delivery through a controlled release system. The addition of albumin to nanoparticles has been proposed to increase drug delivery to tumor cells, facilitating drug transport through interactions with albumin receptors [Sparreboom et al. 2005]. One such drug that investigated the use of nanoparticle-based therapy is rapamycin, which has demonstrated antitumor activity in a mouse model for bladder cancer [Seager et al. 2009]. Albumin-bound rapamycin (ABI-009) is currently being investigated in a phase I/II trial in patients with recurrent NMIBC and BCG refractory disease [ClinicalTrials.gov identifier: NCT02009332].
PANVAC is a recombinant poxviral vaccine containing genes for mucin 1 (MUC 1) and carcinoembryonic antigen, along with costimulatory molecules. Using a vaccine targeting these proteins found in solid tumors may induce an immune response against tumors overexpressing these genes. A trial is currently recruiting to investigate the efficacy of BCG given in combination with PANVAC [ClinicalTrials.gov identifier: NCT02015104].
TMX-101 is a formulation of imiquimod, a toll-like receptor 7 agonist that has shown some evidence of antitumor activity [Smith et al. 2007]. In a phase I trial of 16 patients, TMX-101 has demonstrated safety in patients with NMIBC [Falke et al. 2013]. A phase II trial is currently underway investigating effect of TMX-101 in CIS bladder cancer [ClinicalTrials.gov identifier: NCT01731652].
Lenalidomide is an analogue of thalidomide that inhibits angiogenesis, induces tumor cell apoptosis, and has an immunomodulatory role. A study investigating lenalidomide showed augmentation to the BCG response in an in vivo mouse model [Jinesh et al. 2013]. Efficacy of oral lenalidomide to intravesical BCG is currently being investigated in a phase II trial [ClinicalTrials.gov identifier: NCT01373294].
Conclusion
CIS of the bladder is a difficult and complex disease that requires close monitoring and extensive discussion regarding treatment options. BCG failures are often heterogeneous and present a difficult therapeutic dilemma. Repeat resections (cT1), BCG maintenance, and dose/regimen alterations may improve tolerability and maintain efficacy. Alternative intravesical therapy may be applicable in select cases and new agents continue to be investigated. RC remains an important option for many patients and should not be unnecessarily delayed.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.