
Abstract
Aim:
This meta-analysis aimed to evaluate the efficacy of magnetic stimulation (MS) in treating female stress urinary incontinence (SUI) and providing an alternative treatment for patients who are unwilling to undergo surgery.
Methods:
Randomized controlled trials (RCTs) that evaluated MS as a remedy for female SUI were retrieved from various electronic databases, including MEDLINE, EMBASE, and the Cochrane Controlled Trial Registry system. Moreover, reference lists for related papers were carefully screened for relevant studies.
Results:
A total of six RCTs evaluating the effect of MS in treating female SUI were included in this study. Compared with the placebo group, the MS group exhibited higher quality-of-life scores [mean difference (MD) 0.59, 95% credibility interval (CI) 0.23–0.95; p = 0.001] and lower International Consultation on Incontinence Questionnaire scores (MD −3.93, 95% CI −5.85 to −2.01; p < 0.0001). Moreover, they exhibited a higher objective cure rate (odds ratio 8.49, 95% CI 3.08–23.37). In addition, MS treatment reduced the number of episodes of urinary incontinence (MD −1.42, 95% CI −2.24 to −0.59; p = 0.0007) and urine loss on pad test (MD −4.67, 95% CI −8.05 to −1.28; p = 0.007). There were no significant treatment-related adverse reactions.
Conclusion:
This study evaluated the efficacy and safety of MS in the treatment of female SUI. The results have important implications for patients who do not wish to undergo surgical therapy. We found that MS treatment for SUI has positive outcomes, however, future studies should aim at establishing the best protocol for optimizing the therapeutic effect.
Introduction
Urinary incontinence (UI), defined by the International Continence Society and International Urogynecological Association as involuntary urination, is a common, chronic, and distressing disorder that lessens the quality of life (QoL), much like chronic diseases such as stroke.1–3 Among the three main types of UI identified by the Standardization Steering Committee, the most common is stress urinary incontinence (SUI). 4 Even though its incidence rate varies among different locations, it has exhibited a tremendous yearly increase, which causes significant negative economic and social impacts.5,6
Conservative and surgical therapies are the main options for managing female SUI. Burch and urethral sling procedures are regarded as primary surgical procedures with a high cure rate of between 70% and 90%. 7 Due to complications associated with invasive procedures, such as pelvic pain and difficulties in urinating, however, surgery is not a preferable therapeutic option. According to the 2017 European Association of Urology guidelines on UI therapy, pelvic floor muscle training (PFMT), bladder training, electrical stimulation (ES), magnetic stimulation (MS), and posterior tibial nerve stimulation are potential therapeutic options for SUI. 8 PFMT, which has been proven to be effective in previous randomized controlled trials (RCTs),9–12 has been recommended as the initial therapeutic option for SUI by the American Urological Association (AUA) and Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU). Improvement in clinical outcomes for SUI after PFMT range from 50% to 70%; however, due to poor compliance, the cure rate does not exceed 15–30%.13,14 Notably, ES, a replacement therapy, has a success rate of 48–70%. 15 Due to the discomfort or pain associated with high-intensity percutaneous currents, the use of ES as a therapeutic option is limited.16–20 In 1998, the US Food and Drug Administration recommended MS as the first choice therapeutic option for SUI. 21 Since then, clinical applications for MS have improved due to its associated security, automatic contraction, absence of malaise from probe insertion, and ease of administration.
Various clinical trials have evaluated the efficacy of MS in ameliorating female SUI with positive outcomes. One systematic review 22 evaluated the effect of MS on the treatment of SUI, but did not adequately provide the number of included RCTs, analysis of outcome indicators, or the therapeutic mechanism of MS. The above analyses only involved studies written in English, which potentially could have omitted several other relevant studies. We, therefore, conducted a meta-analysis, which not only summarized the data from published reviews, but also integrated the data from other newly published RCTs to evaluate comprehensively the effects of MS on SUI in terms of improving QoL and reducing the incidence and severity of UI. By summarizing reports in other relevant literature, we further discuss the mechanism of MS in the treatment of SUI and put forward reasonable suggestions for the treatment plan.
Materials and methods
Search strategy
This meta-analysis was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 23 All RCTs evaluating the association between SUI and MS, and published up to 1 March 2021 were independently reviewed by two authors. Appropriate trials were extracted from electronic databases, including MEDLINE, EMBASE, and the Cochrane Controlled Trials Register, using various combinations of Medical Subject Heading terms. The search terms used were ‘magnetic stimulation’, ‘stress urinary incontinence’, and ‘RCTs’. Repeated studies were excluded from analysis. A third party was involved to mediate any arising disputes. There were no language restrictions for the included studies.
Inclusion criteria and trial selection
The inclusion criteria for the RCTs were: (a) those evaluating the curative effect of MS as a remedy for female SUI; (b) those with full content and relevant data that could be acquired; (c) those with authentic data, chiefly incorporating the sum of subjects and the meritorious consequences of each index. Provided the same outcomes were issued in various journals or at diverse times, the updated research results were absorbed in this meta-analysis. Results from the same group of researchers were included once.
Quality assessment
The Jadad score and the Cochrane bias risk assessment tool were used to evaluate the methodological quality of all included RCTs.24,25 Generation of randomization sequences and incomplete outcome data were involved in quality standardization. Moreover, blinding, allocation concealment, along with freedom from selective reporting and other biases, were incorporated (Table 1).
Details of included studies.
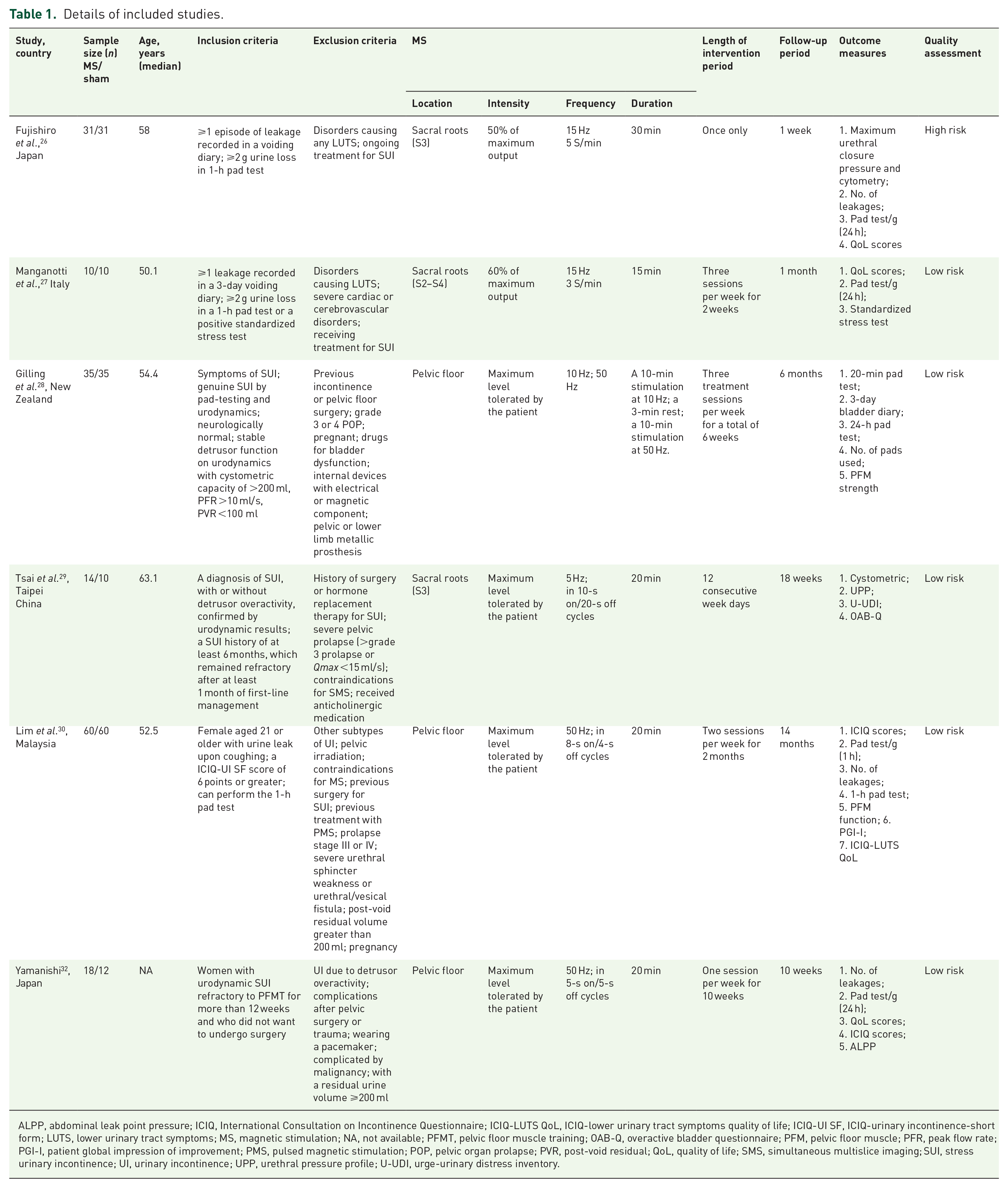
ALPP, abdominal leak point pressure; ICIQ, International Consultation on Incontinence Questionnaire; ICIQ-LUTS QoL, ICIQ-lower urinary tract symptoms quality of life; ICIQ-UI SF, ICIQ-urinary incontinence-short form; LUTS, lower urinary tract symptoms; MS, magnetic stimulation; NA, not available; PFMT, pelvic floor muscle training; OAB-Q, overactive bladder questionnaire; PFM, pelvic floor muscle; PFR, peak flow rate; PGI-I, patient global impression of improvement; PMS, pulsed magnetic stimulation; POP, pelvic organ prolapse; PVR, post-void residual; QoL, quality of life; SMS, simultaneous multislice imaging; SUI, stress urinary incontinence; UI, urinary incontinence; UPP, urethral pressure profile; U-UDI, urge-urinary distress inventory.
Data extraction
Two reviewers used predefined data extraction forms to independently extract data. Disagreements were resolved through mediation by a senior author. The extracted data included: (a) year of publication, first author’s name and country of origin; (b) the type of remedy to which participants had access; (c) therapeutic plan; (d) SUI results; (e) duration of follow up; (f) the total number of participants in each group.
Statistical analysis
Review Manager version 5.3.0 (Cochrane Collaboration, Oxford, UK) was used for data analysis. Fixed- or random-effect models were adopted for appraising indicators. Mean difference (MD) was used to interpret continuous data and odds ratios (ORs) for dichotomous outcomes, coupled with 95% CI. 31 The I-square (I2) test was used to evaluate the effect of heterogeneity on the meta-analysis results. In cases where the I2 value was greater than 50%, a random-effects model was used, whereas if the I2 value was less than 50%, a fixed-effects model was used to evaluate the data. p ⩽ 0.05 was set as the threshold for statistical significance.
Results
Characteristics of the trials
Based on the inclusion and exclusion criteria, a total of 352 articles were extracted. However, after a review of all titles and abstracts, a total of 89 articles were excluded. Due to lack of data, a total of 25 articles were excluded from the remaining 32 articles. Two reviewers separately rated the absolute papers and made a selection following the criteria. Of the remaining 25 articles, 14 articles were excluded for not using appropriate outcome indicators, 6 articles were excluded for not being RCTs, and 5 articles were excluded for using subgroups that were not suitable for analysis. Finally, seven articles containing six RCTs assessing the efficacy of MS for female patients with SUI26–30,32,33 were included in this study. The selection and elimination PRISMA flowchart is presented in Figure 1. Characteristics of the studies are presented in Table 1. The risk of bias graph and summary are shown in Figure 2.

Flowchart of the study selection process.
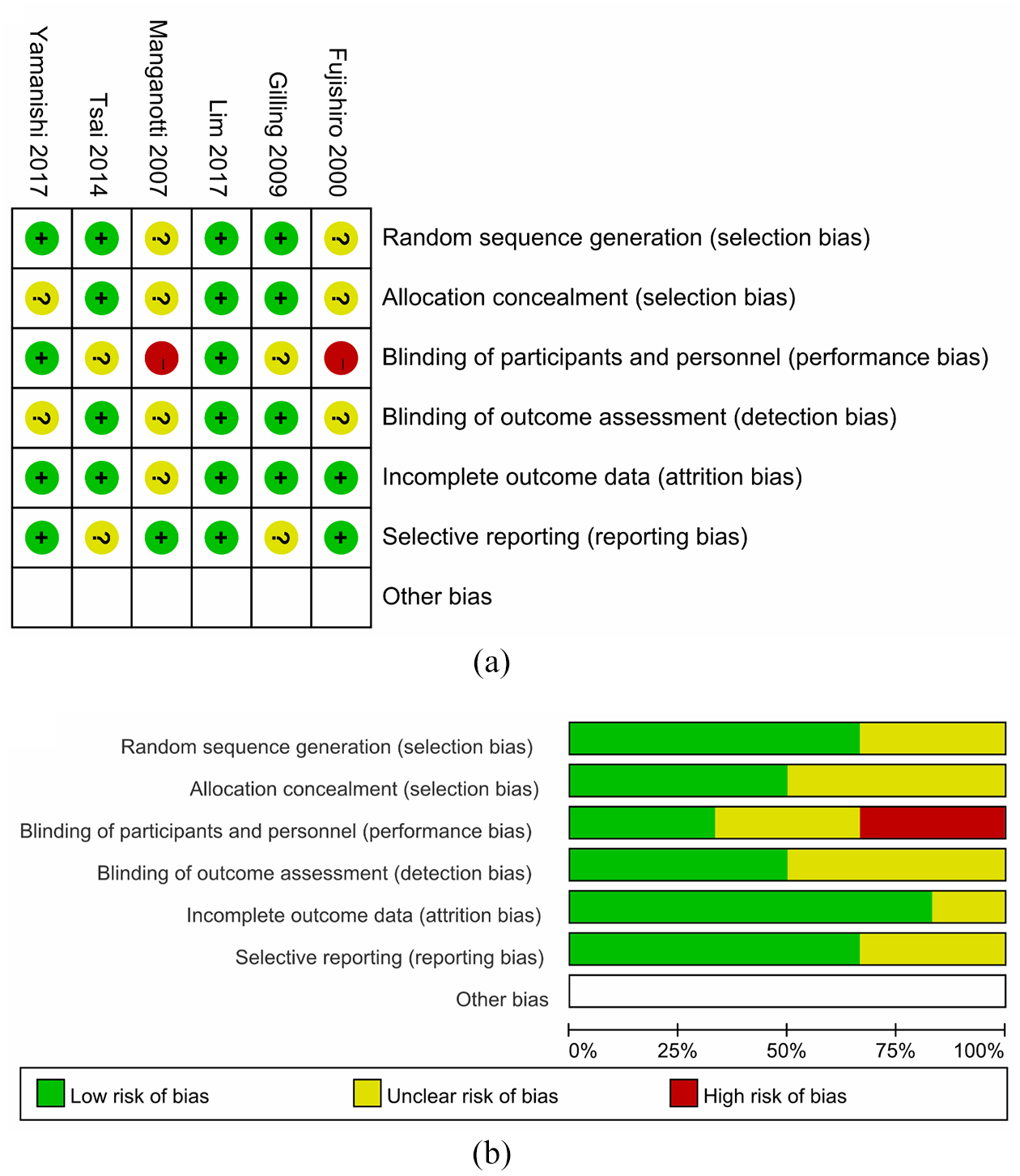
(a) Risk of bias summary: review authors’ judgements about each risk of bias item for each included study. (b) Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies.
QoL scores
QoL scores were extracted from 6 articles involving 336 participants (174 in the MS group and 162 in the sham group). We used a random-effects model to evaluate these RCTs, but the I2 test implied heterogeneity (Figure 3(a)). The study by Lim et al. 33 had the greatest effect. Eliminating this study and using the fixed-effects model remarkably reduced the I2 to 39%. The MD was 0.59, while the 95% CI was 0.23–0.95 (p = 0.001) (Figure 3(b)), implying that MS therapy improved QoL. Then, we performed subgroup analysis of the location of MS to understand the impact on QoL scores, which showed an MD of 0.59, whereas the 95% CI was 0.00–1.18 (p = 0.05) in sacral roots and the MD was 2.7 while the 95% CI was 0.15–5.25 (p = 0.04) in the pelvic floor (Figure 3(c)). These findings indicate that the effect was slightly different due to different stimulation positions of the MS and sham groups.
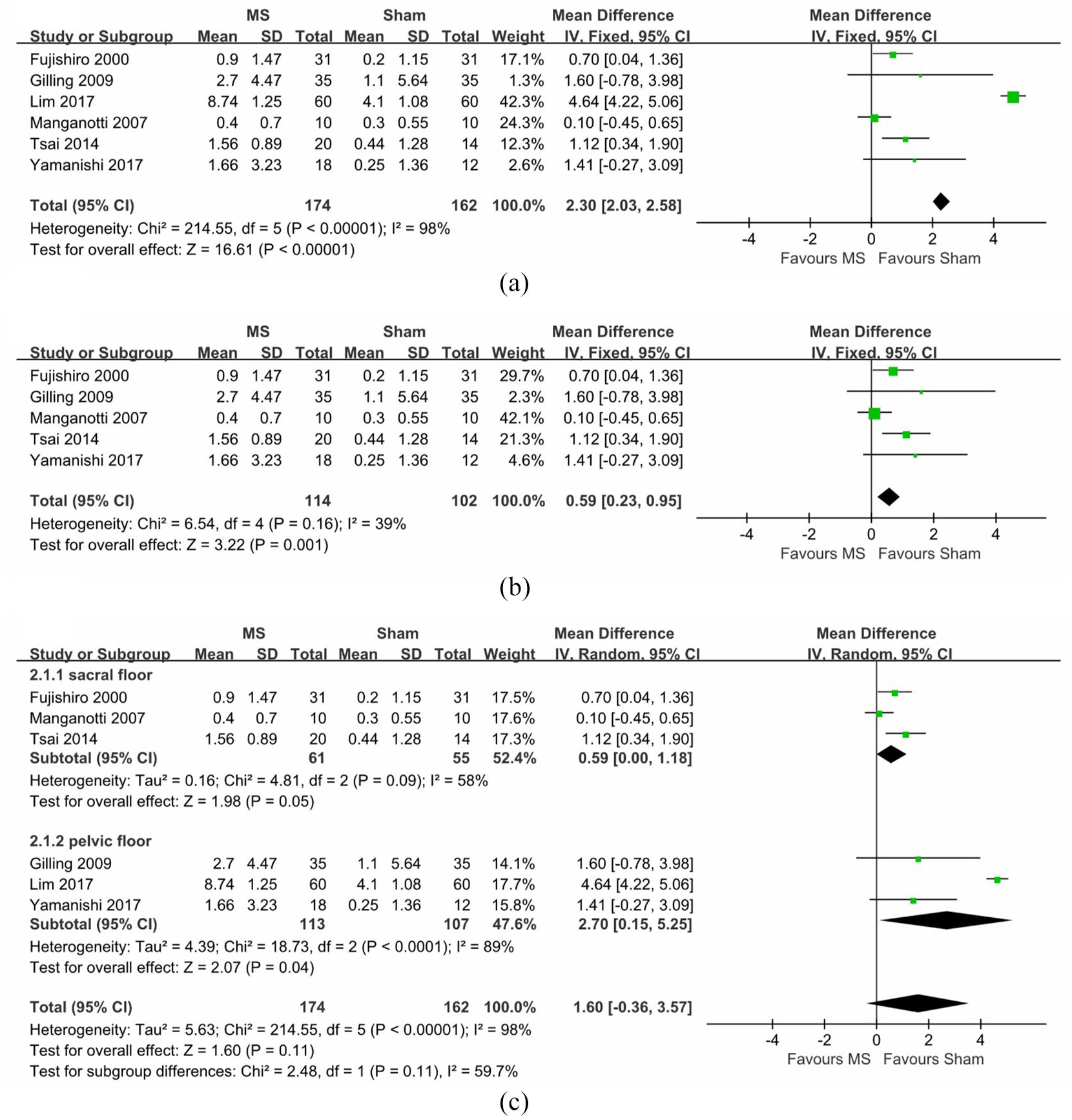
Forest plot comparing the change in (a) QoL scores, (b) QoL scores after omitting study, (c) QoL scores in subgroup analysis of the location of MS between active and sham groups.
Pad test
A total of 5 RCTs involving 197 participants (107 in the MS group and 90 in the sham group) had their pad-test data. Statistical heterogeneity was high, I2 of 47% (p = 0.42) (Figure 4(a)). Given the high heterogeneity between studies, we performed sensitivity analysis. The cross-sectional trial of Manganotti et al. 27 was the only one that was removed. After omission of the study, we found an MD of −4.67 and 95% CI of −8.05 to −1.28 (p = 0.007), without heterogeneity (Figure 4(b)). Patients in the MS treatment group had significantly less urine loss on pad test than those in the placebo group.

(a) Forest plot comparing the change in (a) pad test, (b) pad test after the omitting study, (c) number of leaks, (d) ICIQ scores, (e) objective cure rate between the active and sham groups.
Leaks
Three studies involving 127 participants (72 in the MS group and 55 in the sham group) presented their data on the sum of leaks/week through a voiding diary. A fixed-effects model was selected for analysis. Compared with the sham group, the MS group exhibited a valid decline (MD −1.42; 95% CI −2.24 to −0.59; p = 0.0007), and there was no heterogeneity (Figure 4(c)).
ICIQ scores
Pooled RCTs involving 185 participants (101 in the MS group and 84 in the sham group) presented data on ICIQ scores. A fixed-effects model was introduced to rate these RCTs, notably, the MD was −3.93 and 95% CI was −5.85 to −2.01 (p < 0.0001) (Figure 4(d)). These findings show that ICIQ scores were lower in MS-treated patients.
Objective cure rate
Pooled RCTs with data for objective cure (leakage less than 1 g on the 1-h pad test) rate were used to evaluate the improvement in incontinence symptoms. Patients treated with MS were more likely to be associated with a higher objective cure rate (OR 8.49, 95% CI 3.08 23.37; p < 0.0001) (Figure 4(e)).
Discussion
Despite the small sample sizes and non-uniform treatment regimens used in the majority of the tests, pooled analysis of the data showed that in terms of overall efficacy, the efficacy of MS for SUI was always superior to that of the sham group.
QoL scores, as the most popular indicator for evaluating female SUI treatment, was greatly improved in the MS group compared with the sham group. Studies that assessed QoL reported encouraging results. In their study, Hos¸can et al. 34 reported that the mean QoL score increased from 61.6 to 75.4 after MS (p = 0.003). Elsewhere, Lo et al. 35 used the Urge-Urinary Distress Inventory (U-UDI) to measure QoL. They found an improvement in total UDI-6 scores. The King’s Health Questionnaire is also popular when calculating QoL. 36 Irrespective of which questionnaire was used to evaluate QoL, results tended to be positive. In addition, the ICIQ score questionnaire is highly recommended by the 5th ICI. 37 Due to the rise in in-depth and precise experiments, more meaningful data will emerge, which will enhance our judgement on the efficacy of MS.
Even though studies by Gilling et al. 28 and Yamanishi et al. 32 did not report effective findings, whereas that by Manganotti et al. 27 showed high heterogeneity, pooled data exhibited a positive result in urine loss on pad test. In a single report, deteriorative outcomes in 35.5% of women with SUI based on pad tests were found. 38 However, the study lacked motivation and had a high dropout rate of 35.4%. Another study concluded that the 24-h pad test had no advantage in predicting diacrisis of SUI. 39 A potential breakthrough however was reported by Hos¸can et al. 34 who found that pad weight was reduced from 14.4 ± 10.7 g to 6.5 ± 5.1 g at 3 months in the MS group. Notably, the pad test has many detection schemes, which may lead to deviations in measurement results. Generally, the pad test is controversial and is not a stable test indicator, therefore, more studies are needed to establish the best detection process.
The frequency of incontinence is a vital objective indicator for assessing the reliability of MS treatment. Although our meta-analysis included three RCTs, pooled data showed that the reduction in frequency of SUI was statistically significant. Galloway et al. 40 found a significant reduction in the median number of pads, as well as a significant reduction in leakage events and frequency of detrusor instability, which concurs with our findings and supports the effectiveness of MS in reducing the frequency of incontinence.
A large proportion of patients with moderate or below SUI mostly present with external urethral sphincter (EUS) and pelvic floor muscle weakness. 41 EUS has complete neuromuscular innervation and can be used to cope with movement by increasing its size and strength. 42 Eddy currents can be induced by transcutaneous MS in the pelvis from where they flow into tissues, thereby depolarizing the axons. As a peripheral motor nerve axon, the impulse passes to the motor endplate, inducing the mandatory release of acetylcholine. Then, homologous muscle fibers depolarize and contract.40,43 MS may modify the activity in pelvic floor muscle groups, as well as the discharge pattern and frequency of motor nerve fibers responsible for resting tension of the pelvic floor and sphincter. Moreover, MS is associated with a significant increase in bladder volume, which may be attributed to acute activation of the inhibitory detrusor reflex pathway after stimulation of the pudendal afferent nerve. Fujishiro et al. 26 and Tsai et al. 29 reported changes in bladder volume and maximum urethral closure pressure after MS treatment. Bladder capacity in the MS group was significantly higher than that in the sham operation group. Determination of maximum urethral closing pressure, however, did not draw the same conclusion. Elsewhere, Fujishiro et al. 26 reported that the maximum urethral closure pressure did not increase, however, their findings were disapproved by Tsai et al. 29 who concluded that it did. This may be correlated to the different methods of measurement used in the two studies.
The low level of standardization of the MS protocol is challenging. Different studies used different stimulus intensities, frequencies, locations, and durations. Until now, the optimal frequency and duration of the pulse remain controversial. It has been shown that frequencies of 20–50 Hz are effective for SUI, and satisfactory pelvic floor contraction during SUI treatment requires a higher dose of 50 Hz.44,45 Therefore, the treatment may not be as effective as expected in three RCTs using stimuli at frequencies ranging from 5 Hz to 15 Hz. We performed subgroup analysis of QoL scores for the two different stimulation sites of sacral roots and pelvic floor, and the results revealed little difference between the two groups. Based on the above findings, we preliminarily suggested that the stimulation site might affect the therapeutic effect, and that the pelvic floor may exhibit better outcomes. However, studies have not evaluated the effects of different stimulus sites. Therefore, there is a need to determine whether outcome indicators can be improved by stimulating other parts, apart from sacral roots and pelvic floor. Treatment and follow-up duration varied across studies, which inevitably led to differences in outcomes. Galloway et al. 46 concluded that active MS of the pelvic floor twice a week for 6 weeks improved SUI, which remained effective after 3 months. It has also been reported that the benefits of MS worsen over time,40,46,47 perhaps because of the treatment regimen. Therefore, to improve the effectiveness of MS treatment and to promote MS in clinical treatment, an appropriate MS protocol must be developed.
In addition, patients subjected to MS therapy were found to exhibit a higher objective cure rate. It has been reported that the cure rate and improvement rate after Electromagnetic stimulation (EMS) treatment were not much better than those after PFMT treatment. 42 Moreover, Hos¸can et al. 34 reported a 29.7% cure rate. However, after 3 months, they reported a 48.1% improvement rate, as well as an extraordinary improvement in QoL. Suzuki et al. 48 reported a cure rate of 20% in the MS group after active treatment. The results could not be used to disparage MS treatment for patients who were all non-responders to PFMT or drug therapy. This can be explained by active contractions produced by the PFMT exercise muscle strength, which is better than passive contraction induced by MS. Therefore, the therapeutic effect is not satisfactory.
Reported side effects of MS, including lower limbs, abdominal, and back pain, among others, were not severe or life threatening. 38 Fewer side effects associated with MS were reported in the included articles, suggesting that it is relatively safe and tolerable.
This meta-analysis has some limitations. We noted that the quality of the included studies was flawed, in terms of study designs, patient selection, blinding, publication bias, and outcome data. Our results are based on unadjusted estimates. More accurate results will originate from adjustments of other confounders, such as gender, body mass index, lifestyle, and age among others. More RCTs with abundant sample sizes are needed to validate our findings. Additional RCTs should be performed to ascertain the virtue and defects of MS in treating female SUI.
Conclusion
We found that MS may be beneficial in the clinical management of female SUI, especially for patients who do not consent to surgery. More clinical trials are needed to determine the appropriate protocol for optimizing the therapeutic effect.
Footnotes
Author contributions
KS and GW: designing the study; analyzing the extracted data; writing the first manuscript draft.
DZ: searching the literature; extracting and analyzing the data.
TQW and JW: analyzing the data; providing critical scientific input.
HR and YC: resolving discrepancies about the quality of the included studies; reviewing the manuscript; providing critical scientific input.
All authors approved the final version of this manuscript.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the National Natural Science Foundation of China (Nos. 81870525; 81572835), Taishan Scholars Program of Shandong Province (No. tsqn201909199).