
Abstract
Radical cystectomy (RC) remains a highly morbid urologic procedure, and erectile dysfunction (ED) represents a significant burden for bladder cancer survivors. While inflatable penile prosthesis (IPP) offers a definitive treatment option for post-RC ED, the hostile postoperative anatomy of RC patients poses some technical challenges for IPP implantation. We report the case of a 54-year-old male with high grade bladder cancer who was managed with a robotic-assisted RC with Bricker ileal conduit urinary diversion and simultaneous implantation of a 3-piece IPP. Operative time was 310 min (230 min for the RC and ileal conduit portion, 80 min for IPP implantation). Estimated blood loss was 300 ml. Postoperative course was regular. The patient was discharged home on postoperative day 6. A robotic RC with concomitant IPP implantation can be offered as “one-step” solution to bladder cancer male patients. This approach can potentially offer the advantage of better outcome in terms of sexual function, while minimizing surgical risks, ultimately improving the quality of life of these patients.
Keywords
Introduction
Radical cystectomy (RC) remains a highly morbid urologic procedure, 1 and erectile dysfunction (ED) represents a significant burden for bladder cancer survivor undergoing this demolitive surgery. 2 Over the past few years, robotic surgery has been increasingly implemented in bladder cancer management, driven mainly by a potential advantage in terms of postoperative recovery. 3 Inflatable penile prosthesis (IPP) offers a definitive treatment option for ED that is refractory to medical therapy, 4 but the hostile postoperative anatomy of RC patients might pose some technical challenges for penile prosthesis surgery. 5 Only a few studies have shown that a three-piece inflatable penile prosthesis can be placed safely after significant prior intraabdominal surgery.6,7
As health-related quality-of-life outcomes continue to gain increasing importance in bladder cancer survivors, 8 urologists should discuss and offer IPP as treatment of choice for refractory ED. In this regard, an alternative pathway could be the concomitant implantation of IPP at the time of RC procedure, as already reported in patients undergoing radical prostatectomy for prostate cancer. 9
Herein, we report a case of RARC with intracorporeal ileal conduit urinary diversion and concomitant three-piece penile prosthesis implantation.
Case description
We report the case of a 54-year-old male [body mass index (BMI) = 27 kg/m2], with a past medical history of significant hypertension. He underwent a transurethral resection of bladder in late 2020 due to a trigonal lesion, with pathology finding of high-grade muscle invasive bladder cancer (BC). Given elevated prostate-specific antigen (PSA) at 4.2 ng/ml, he also underwent a transrectal biopsy of the prostate, which showed high-grade prostatic intraepithelial neoplasia (PIN). Clinical staging was completed by performing a computed tomography (CT) with and without contrast and total body bone scan, both negative for metastasis.
Given bulky high-risk BC, patient was offered a non-nerve robotic-assisted RC with Bricker ileal conduit urinary diversion and simultaneous implantation of a three-piece penile prosthesis to remedy fibrosis, after completing a course of neo-adjuvant systemic therapy.
Baseline assessment included a psycho-sexual assessment, which showed patient to be suitable for such an approach. Risks and benefits were discussed extensively with patient who elected to proceed. Moreover, penis measurement was also performed at baseline (14 cm) and documented in the medical chart. The patient was sexually potent at baseline with a Sexual Health Inventory for Men (SHIM) score of 24.
Institutional Review Board (Fondazione “G. Pascale” IRCCS, Naples, Italy) waived approval, given that this was a retrospective chart review. Written informed consent for patient information and images to be published was provided by the patient.
Surgical procedure
Antibiotic prophylaxis with 2 g cefazolin was used 1 h before surgery. Metronidazole 500 was also given at the time of intestinal resection. After cystectomy, and before IPP implantation, gentamicin 160 mg + cefazolin 2 g were administered.
For the robot-assisted RC with intracorporeal ileal conduit, we used a DaVinci Xi system with port configuration as shown in Figure 1. RC and extended bilateral LND (lymph node dissection) were performed. At the end of the RC, the patient was re-positioned, and the field was prepped again with the “no touch” technique. 10

Port placement for the robotic procedure, stoma site, and incision site for the placement of the reservoir.
A bilateral 18 + 1 cm tip Coloplast Titan® touch prosthesis was implanted after measuring the corpora cavernosum. The 125-ml reservoir was placed in the lateral extraperitoneal space through a counter incision medial to the anterior superior iliac spine. The connecting tube was passed through the fascia and into a subcutaneous channel up to scrotum, where it was connected. The length of the erected penis was found to be 14.5 cm, in line with the preoperative measurements (Figure 2). Implantation was easy, given the preserved state of the corpora cavernosa. A scrotal drain was placed. The penis was wrapped with a cohesive bandage (“mummy wrap” technique). 11
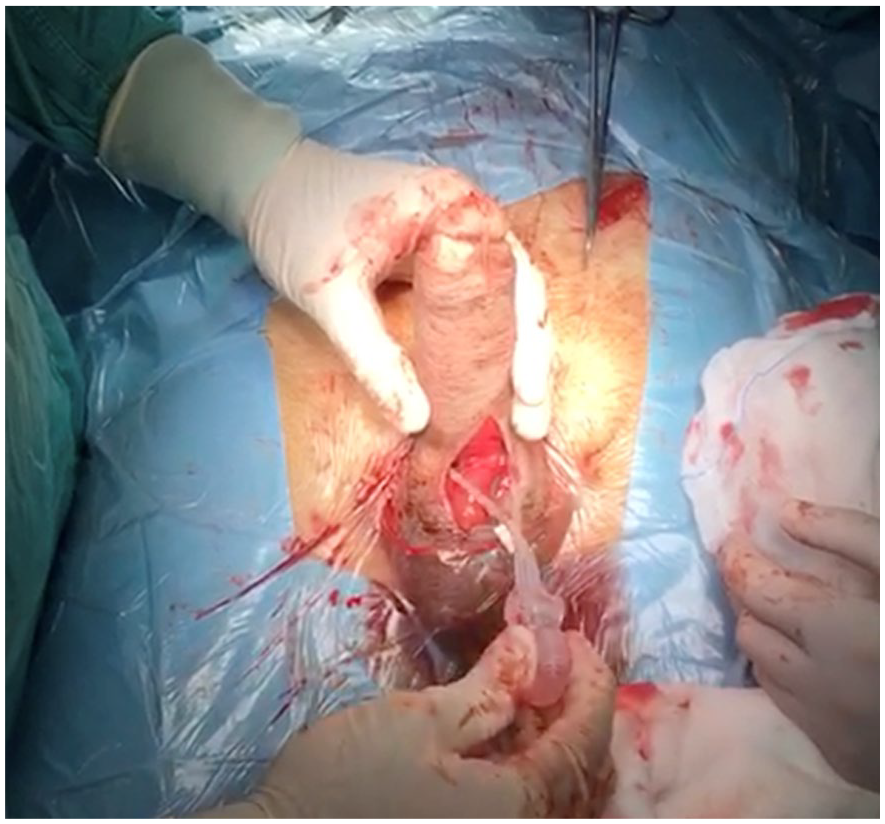
Intraoperative image of implanted IPP.
Results
Operative time was 310 min (230 min for the RC and ileal conduit portion, 80 min for IPP implantation). Estimated blood loss was 300 ml. Postoperative course was regular. Scrotal drain and bandage were removed on the first postoperative day. Early mobilization of the patient was encouraged on postoperative day 1. The patient passed gas on postoperative day 2, and liquid diet was started, and advanced to regular diet on postoperative day 4. The patient was discharged home on postoperative day 6. Daily teaching was performed on how to activate and deactivate the prosthesis, and before discharge, the IPP’s first mentored activation was performed. Pathology showed pT3a disease with negative margins. The patient was disease-free, potent, and sexually active at 6 months, with a SHIM score of 25.
Discussion
To the best of our knowledge, we report the first case of concomitant robotic RC and IPP implantation in a patient with bladder cancer. With adequate pre-surgical counseling, and appropriate surgical technique, a favorable outcome can be achieved. This can represent a management option that allows cancer control while preserving sexual function, therefore minimizing the impact of highly demolitive surgery on a patient’s quality of life.
Some considerations can be made in discussing this case. While the adoption of robotic surgery might allow the surgical morbidity of RC procedure to be minimized, 3 sexual dysfunction remains a major issue, especially in those cases where a nerve-sparing approach is not advisable for oncological reasons. 2 ED radical pelvic surgery remains often refractory to medical therapies, and therefore IPP implantation can be offered as more effective treatment modality. 5
There are only a limited number of series reports on the outcomes of IPP implantation in BC patients after RC. One of the reasons for such limited literature might be the technical challenges that IPP placement procedure can present in these patients. 5 Using a large national claims database, Chappidi et al. found that only a limited portion of RC patients use ED treatments in general, and this is especially true when it comes to IPP. 2 Falcone et al. 6 evaluated the surgical outcomes of IPP implantation in RC patients over a 17-year period in four tertiary referral centers in Italy. Median time elapsed between RC and IPP implantation was 38 months. Reservoir position was extra-peritoneal (using a separate abdominal incision) in 54.8% of cases. Infection and mechanical failure rates were 2.1% and 6.3%, respectively. Loh-Doyle reviewed 80 patients who underwent primary placement of a three-piece IPP (AMS 700) after RC and urinary surgery. 5 An infrapubic approach was used in most patients, with reservoir placement in the lateral retroperitoneal space through a counter incision medial to the anterior superior iliac spine (similarly to the present case). After mean follow up of 53.9 months, only four patients developed infection of the prosthesis that required removal, and five required revision surgery for mechanical failure.
To date, simultaneous implantation of penile prostheses has been described only in patients undergoing radical prostatectomy. Cocci et al. argued that a simultaneous procedure would avoid two admissions, reduce hospitalization time, and guarantee faster recovery of sexual function. 9 In addition, it might prevent the otherwise unavoidable loss of penile length, which is perceived as an issue in BC survivors after RC. 12 This rationale led us to offer this option to our patient, as a major benefit of concomitant surgery is the ability to preserve penile length.
Once concern about offering IPP at the time of RC is certainly related to the risk of infection. Studies exploring increased risk of adverse outcomes with secondary procedures have been reported. 13 Risk of infection should be addressed by implementing a stringent antibiotic prophylaxis protocol, and of course discussed with patient as part of preoperative counseling. One might argue that another strategy for a young patient with normal preoperative erectile function would be to perform a nerve-sparing procedure with attempt at penile rehabilitation. 14 In this present case, cancer characteristics (bulky high-risk disease) and the fact that the patient was very motivated to pursue the option with the highest chances of maximal quick recovery of sexual function, drove our final strategy. This was noted and discussed with the patient.
We acknowledge this to be a single case report, and with lack of long-term follow up. Overall, this experience can stimulate future research effort, ideally within the framework of a case–control prospective study.
Conclusions
Although this is a preliminary experience, a robotic RC with concomitant IPP implantation can be offered as “one-step” solution to male BC patients. This approach can potentially offer the advantage of better outcome in terms of sexual function, while minimizing surgical risks, ultimately improving the quality of life of these patients.
Footnotes
Author contribution statement
All authors made a substantial contribution to the concept or design of the work; or acquisition, analysis or interpretation of data; drafted the article or revised it critically for important intellectual content; and approved the version to be published.
Conflict of interest statement
The author(s) declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.