
Abstract
Erectile dysfunction (ED) impacts over 100 million men worldwide and occurs at a higher incidence in men with hypertension. Beta blockers are one of several antihypertensive drug classes associated with ED. Nebivolol is a beta blocker with vasodilating properties mediated through endothelial release of nitric oxide which facilitates penile erection. Thus, nebivolol may offer an advantage over other beta blockers in the patient with hypertension and ED. A literature search comparing nebivolol with other beta blockers identified four European studies of limited duration, with the longest study being 28 weeks. Survey scores for erectile function showed significant improvement in erectile function with nebivolol in two of the studies, while the other two studies showed erectile function did not significantly worsen with nebivolol as compared with other beta blocker agents. One study showed improved erectile function scores, possibly due to the presence of a Hawthorne effect. Based on this small sample of studies, nebivolol may be of use in the patient with or at risk of developing ED, when a practitioner specifically wants to use a beta blocker as add-on antihypertensive treatment.
Introduction
Erectile dysfunction (ED) is defined as the persistent inability to attain or maintain penile erection sufficient for satisfactory sexual performance, and is estimated to affect more than 30 million men in the United States (US) and 100 million men worldwide [Doumas et al. 2006]. Men with hypertension have a higher incidence of ED compared with those without hypertension [Cordero et al. 2010]. Furthermore, certain antihypertensive medications may exacerbate the problem of ED [Boydak et al. 2005]. Antihypertensive agents associated with a greater risk for ED include beta blockers, centrally acting alpha agonists, and thiazide diuretics [Fogari et al. 2001, 2004].
Beta blockers are widely prescribed to treat not only hypertension, but also for mortality reduction in patients with heart failure or a history of myocardial infarction [Ko et al. 2002]. Beta blockers differ with respect to their mechanisms of action, especially in terms of beta-1 adrenoceptor selectivity and vasoactive effects [Brixius et al. 2007]. First generation beta blockers are nonbeta receptor selective (e.g. propranolol), whereas second generation beta blockers are more beta-1 adrenoreceptor selective (e.g. metoprolol, atenolol). Third generation agents not only have beta adrenoreceptor-blocking activity, but have additional vasodilating properties (e.g. carvedilol, labetalol, nebivolol) [Stoschitzky, 2010; Fongemie and Felix-Getzik, 2015]. The vasodilating properties of nebivolol (Bystolic®) arise from its ability to stimulate endothelial release of nitric oxide. This is important, since endothelial release of nitric oxide in response to stimulation of nonadrenergic, noncholinergic neurons is probably the principle mechanism leading to relaxation of smooth muscle in the corpus cavernosum, thereby permitting penile erection [Boydak et al. 2005]. Therefore, nebivolol by its mechanism of action may offer an advantage over other beta blockers when used to treat the patient with hypertension and ED. In this review, we discuss the evidence comparing nebivolol with other beta blocker agents in hypertensive men with ED.
Comparative studies with other beta blockers
Searches of MEDLINE and International Pharmaceutical Abstracts (1966–June 2016) were performed using the terms nebivolol, beta blockers, and ED. The literature search produced four studies which compared the occurrence of ED in patients taking nebivolol with other beta blockers (see Table 1).
Summary of human trials.
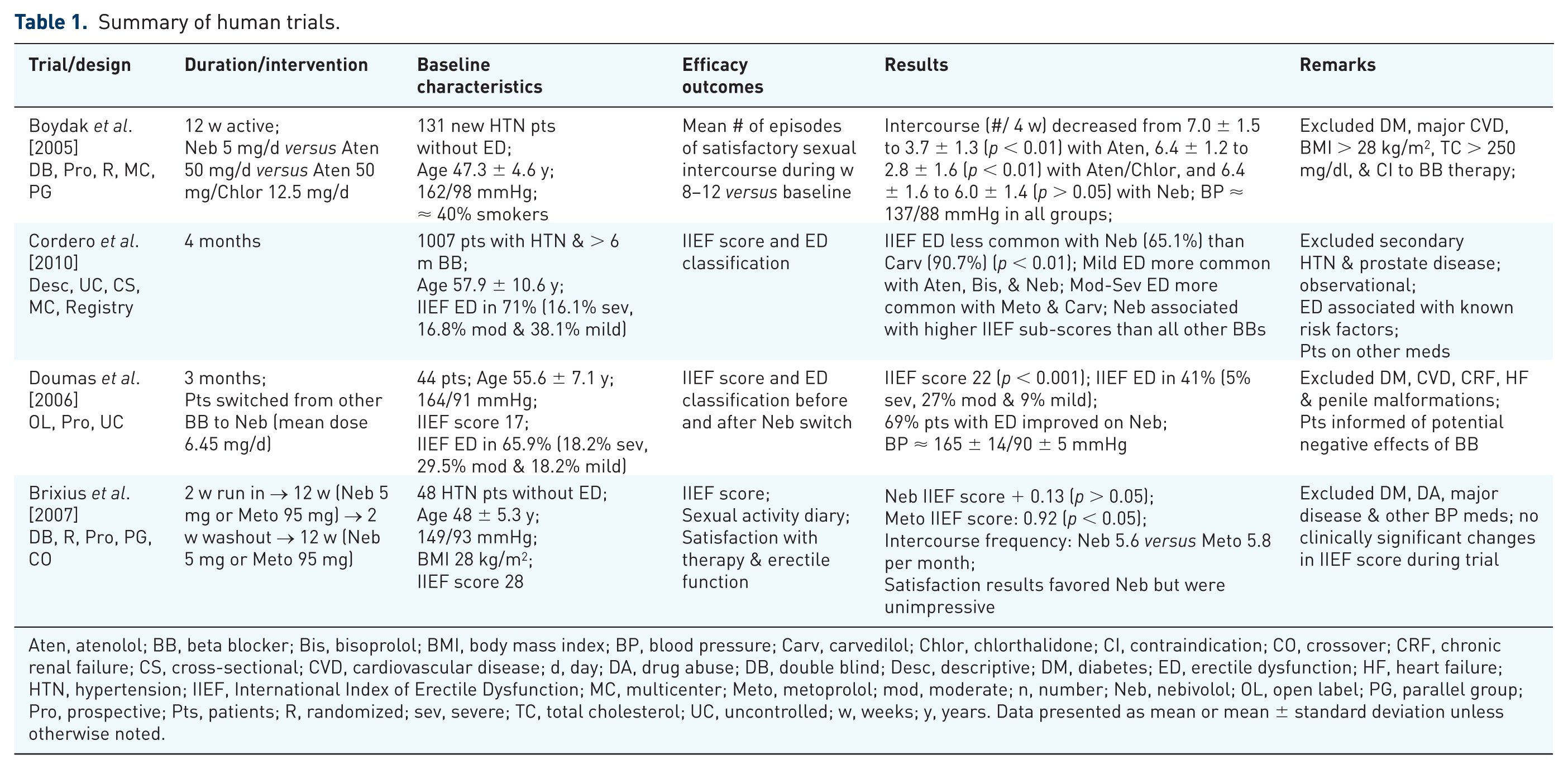
Aten, atenolol; BB, beta blocker; Bis, bisoprolol; BMI, body mass index; BP, blood pressure; Carv, carvedilol; Chlor, chlorthalidone; CI, contraindication; CO, crossover; CRF, chronic renal failure; CS, cross-sectional; CVD, cardiovascular disease; d, day; DA, drug abuse; DB, double blind; Desc, descriptive; DM, diabetes; ED, erectile dysfunction; HF, heart failure; HTN, hypertension; IIEF, International Index of Erectile Dysfunction; MC, multicenter; Meto, metoprolol; mod, moderate; n, number; Neb, nebivolol; OL, open label; PG, parallel group; Pro, prospective; Pts, patients; R, randomized; sev, severe; TC, total cholesterol; UC, uncontrolled; w, weeks; y, years. Data presented as mean or mean ± standard deviation unless otherwise noted.
A double-blind study was conducted involving 131 married men with newly diagnosed hypertension. After a 4-week placebo run-in period, patients were randomized to receive 12 weeks of therapy with nebivolol 5 mg/day (n = 43), atenolol 50 mg/day (n = 44), or atenolol 50 mg/day plus chlorthalidone 12.5 mg/day (n = 44). Erectile function (instances of successful intercourse/month) was assessed by a questionnaire at baseline and at the end of the double-blind treatment period. The sexual function questions came from the Measurement of Quality of Life in Hypertensive Patients: A Practical Approach [Bulpitt and Fletcher, 1990]. Results showed the mean number of episodes of satisfactory sexual intercourse was significantly decreased from baseline in those receiving atenolol (from 7.0 to 3.7; p < 0.01) and atenolol plus chlorthalidone (from 6.4 to 2.8; p < 0.01); whereas, the number of episodes remained constant in the group receiving nebivolol (6.4 at baseline and 6.0 during last month of treatment) [Boydak et al. 2005].
A cross-sectional, observational multicenter study was conducted in 1007 male patients (mean age 57.9 years) with a history of hypertension being actively treated with a beta blocker agent for at least the prior 6 months. The study inclusion period lasted 4 months and ED was assessed via the 15-item International Index of Erectile Dysfunction (IIEF) questionnaire. Parameters assessed with the IIEF questionnaire include erectile function, orgasmic function, sexual desire, satisfaction with intercourse, and global satisfaction. Analyzing the score sum of the six survey questions dealing with erectile function allows the classification of ED into four categories: No ED (26–30 points), mild ED (17–25 points), moderate ED (11–16 points) and severe ED (6–10 points). Reported beta blockers used during the 4-month inclusion period were atenolol (27.9%), bisoprolol (25.9%), carvedilol (15.3%), metoprolol (3.0%), nebivolol (23.6%) and others (0.5%). Study results showed patients without ED were more frequently treated with nebivolol (34.9%) than carvedilol (10.3%) (p < 0.01). This was the only between-drug comparison to achieve a statistically significant difference. Patients treated with nebivolol obtained higher scores in every IIEF parameter compared to those taking other beta blocker agents (p < 0.01) [Cordero et al. 2010].
An open, prospective outpatient study of 44 men (age range 31–65 years) with essential hypertension being treated with beta blockers (atenolol, metoprolol, bisoprolol) for at least 6 months was conducted, where they were given the IIEF questionnaire. Patients were told that erectile function may be affected by beta blocker therapy and the aim of the study was to investigate the effect of another beta blocker (nebivolol) on erectile function. After the previous beta blockers were discontinued, patients were given nebivolol (mean dose 6.45 mg/day) for 3 months, after which they again completed the IIEF questionnaire. At baseline, ED of any degree was found in 65.9% of patients (18.2% severe, 29.5% moderate, and 18.2% mild). After being switched to nebivolol, ED was found in 41% of patients (5% severe, 27% moderate, and 9% mild). The mean IIEF score (17 versus 22) showed erectile function had a statistically significant (p < 0.001) improvement after 3 months of taking nebivolol (20 out of 29 patients (69.0%)) [Doumas et al. 2006].
In the final study, 48 heterosexual men (age range 40–55 years) with hypertension were randomized to two different treatment groups following a 2-weeks’ placebo run-in period. The first group received nebivolol 5 mg daily for 12 weeks, followed by placebo for 2 weeks and then metoprolol succinate 95 mg daily for 12 weeks. The second group received metoprolol succinate 95 mg daily for 12 weeks, followed by placebo for 2 weeks and then nebivolol 5 mg daily for 12 weeks. Patients had clinic visits at screening, at the baseline randomization visit and every 4 weeks during the active treatment periods. Patients were given the IIEF questionnaire at each visit. When all measurements obtained between the start and the end of the treatment period were aggregated, nebivolol did not significantly alter the mean erectile function subscore (+0.13 points) of the IIEF questionnaire; whereas, the score significantly decreased in those taking metoprolol by −0.92 points (p < 0.05) [Brixius et al. 2007].
Discussion
There are few data on the potential benefits of nebivolol for ED. The four studies available did report positive results, with two of the studies showing significant improvement in erectile function with nebivolol and the other two studies showing erectile function did not significantly worsen with nebivolol as compared with other beta blocker agents.
The study by Doumas and colleagues was the only one that showed the erectile function score improved after taking nebivolol despite the patients having knowledge that erectile function may be affected by beta blocker therapy [Doumas et al. 2006]. This may have been due in part to the Hawthorne Effect. The Hawthorne Effect is defined as the alteration of behavior of patients due to their awareness of being observed. In the case of ED, prior patient knowledge that a beta blocker may cause the side effect of ED may influence its reported occurrence [McCambridge et al. 2014]. This poses the question of what clinical significance does the Hawthorne Effect have in a patient with ED taking a beta blocker? There are two previous studies involving beta blockers where the Hawthorne effect was studied in relation to the incidence of ED. In the first study, 114 men without ED but with newly diagnosed hypertension were randomized into three groups and treated for approximately 60 days with metoprolol 100 mg daily. Group 1 patients knew they were being given metoprolol and knew ED was a possible side effect. Group 2 patients knew the drug name but were not told of a possible ED side effect. Group 3 patients knew neither the drug name nor a possible ED side effect. After 60 days the ED incidence according to the IIEF questionnaire was 32% in group 1, 13% in group 2, and 8% in group 3 (p < 0.01) [Cocco, 2009]. In another study with the same design, 96 men with newly diagnosed cardiovascular disease were treated with atenolol 50 mg daily for three months. At the end of the study the incidence of ED was 31.2% in the group who knew of the drug they were receiving as well as the possible ED side effect compared to just 15.6% in those told only the drug name and 3.1% in those told neither the drug name or potential for ED (p < 0.01) [Silvestrie et al. 2003]. To clarify the impact of the Hawthorne Effect, more studies are needed comparing ED incidence between nebivolol and other beta blockers in which patients are made aware of the possible ED side effect at the beginning of the study.
In addition, a number of other questions remain in regard to use of nebivolol in the patient with ED. What impact would concomitant use of nebivolol with a phosphodiesterease-5 inhibitor (e.g. sildenafil) have on ED, particularly in patients with diabetes and hypertension? Limited laboratory data have shown the ability of nebivolol to potentiate the relaxation activity of phosphodiesterase-5 inhibitors on human penile tissue in patients with a history of diabetes [Martinez-Salamanca et al. 2014]. Can the results of these four studies be extrapolated to an ED patient taking nebivolol long term, given the longest studied time period in these four studies was 28 weeks [Brixius et al. 2007]? Can the results of these studies be extrapolated to patients in the US? Finally, what type of patient would be the best candidate for nebivolol? Recent guidelines and recommendations for the treatment of hypertension state that beta blockers are not recommended for the initial treatment of hypertension, and are second-line agents behind thiazide diuretics, calcium channel blockers, angiotensin converting-enzyme inhibitors, and angiotensin II receptor blockers [James et al. 2014].
In the US, nebivolol is only indicated for the treatment of hypertension. Nebivolol is indicated for the treatment of heart failure in other countries. Numerous small-duration trials with nebivolol have shown beneficial hemodynamic effects. However, there are few long-term trials showing that these effects translate into long-term clinical benefits. This fact, in addition to a lack of head-to-head trials with beta blockers indicated for heart failure and ischemic heart disease have limited the clinical use of nebivolol in the US [Fongemie and Felix-Getzik, 2015].
Beta blockers are still widely taken by millions of Americans with about 128 million yearly prescriptions filled as recently as 2009 [Consumer Reports Health.org, 2011]. Based on the small sample of studies we found, it appears nebivolol may benefit patients with ED when a practitioner specifically wants to use a beta blocker as add-on antihypertensive treatment. It appears that counseling patients that there is limited data indicating ED will not worsen while taking nebivolol is appropriate.
Conclusion
Nebivolol has a unique mechanism of action involving release of nitric oxide, resulting in penile vasodilation, which may be beneficial in the male patient with a history of hypertension and ED. Limited short-term studies comparing nebivolol with other beta blockers indicate erectile function did not worsen and may improve. Many questions remain to be answered before nebivolol can be considered the recommended beta blocker in this patient population.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.