
Abstract
Background and purpose:
Benign prostatic hyperplasia (BPH) is the most common urologic disorder affecting older men, necessitating medical or surgical intervention. Limited data exists regarding the effect these surgeries have on the endourologist’s musculoskeletal system following the surgery because of the required difficult posture, prolonged procedures, repetitive movements, and the settings of an adjustable visual display terminal workstation. The aim of our study was to survey the prevalence and possible causes of musculoskeletal disorders among endourologists performing transurethral resection of the prostate (TURP) or laser prostatectomy using either holmium laser enucleation or thulium laser enucleation.
Materials and methods:
An email inviting all members of the Endourological Society to participate in the survey was sent. The questionnaire included different demographic and practice characteristics, with concern regarding performing either TURP or laser prostatectomy and the incidence and type of musculoskeletal incidents following these surgeries. All responses were collected by a commercially available internet based survey host (www.surveymonkey.com) over a period of 6 weeks.
Results:
Of the 121 complete responses, 84 (69%) of endourologists complained of a musculoskeletal disorder following TURP or laser prostatectomy. The most frequent complaint was for neck (64%), followed by back (57%), shoulder (48%), hand (40%), and elbow (18%). The average prostate volume turned out to be the most compelling predictor for musculoskeletal disorder occurrence with an average prostate volume of 76 g operated on by the complaining group compared with 59 g in the noncomplaining group. Those with more severe symptoms were linked to a mean prostate size of 80 g (60–146) and constantly complained of shoulder, neck, or back trouble compared with the less-severely complaining group.
Conclusions:
A high prevalence of musculoskeletal complaints among urologists performing endourologic prostatectomy was confirmed and was found to be proportionally related to the size of the prostate. The integration of an ergonomic specialist inside the operation room to watch and correct the surgeon’s position during endourologic procedures may reduce the endourologist’s exposure to these occupational hazards.
Introduction
Benign prostatic hyperplasia (BPH) is the most common urologic disorder affecting older men. 1 Although many are successfully managed with medical therapy and behavioral modification, a proportion of men will progress to surgical intervention. 2 Advances in minimally invasive urologic instrumentation has allowed urologists to perform either transurethral resection of the prostate (TURP) 3 or laser enucleation of the prostate via either a holmium (HoLEP) 4 or thulium laser. 5
Ergonomic challenges 6 that could lead to musculoskeletal symptoms in endourologic surgeons 7 have been associated with difficult posture, prolonged procedures, 8 repetitive movements, 9 and the settings of an adjustable visual display terminal workstation. 10 Many previous studies have investigated the general principle of musculoskeletal disorders during laparoscopic or endourologic surgeries. 11
The aim of our work was to survey the prevalence and possible causes of musculoskeletal disorders among endourologists performing TURP or laser prostatectomy.
Materials and methods
An email was sent to more than 3000 global members of the Endourological Society inviting them to participate in the survey. The survey consisted of a set of single, multiple choice, and free text questions (see Supplemental Material). Responses were elicited regarding the demographic and practice characteristics, size of treated prostate, surgical volume, operating position, dominant hand, and type of working element. Participants were queried on musculoskeletal symptoms following these surgeries, focusing on the hand/wrist, elbow, shoulder, neck, and lower back.
All responses were collected by a commercially available internet based survey host (www.surveymonkey.com) over a period of 6 weeks. Statistical analyses were performed using JMP™ software utilizing the chi-squared test for comparing discrete variables, whereas the Wilcoxson singed-rank test was used for continuous variables.
Results
From 14 November 2018 to 4 January 2019, 155 responses were received, of which 27 incomplete responses and seven individuals who did not perform BPH procedures were omitted. Respondent demographics and practice characteristics are reported in Table 1. Of 121 complete responses, 84 (69%) endourologists complained of a musculoskeletal symptom following TURP or laser prostatectomy. Although most respondents performed both procedures (TURP n = 121, laser n = 112), more surgeons had more than 10 years’ experience with TURP compared with laser prostatectomy (63% versus 12%).
Different characteristics of complaining and noncomplaining urologists.
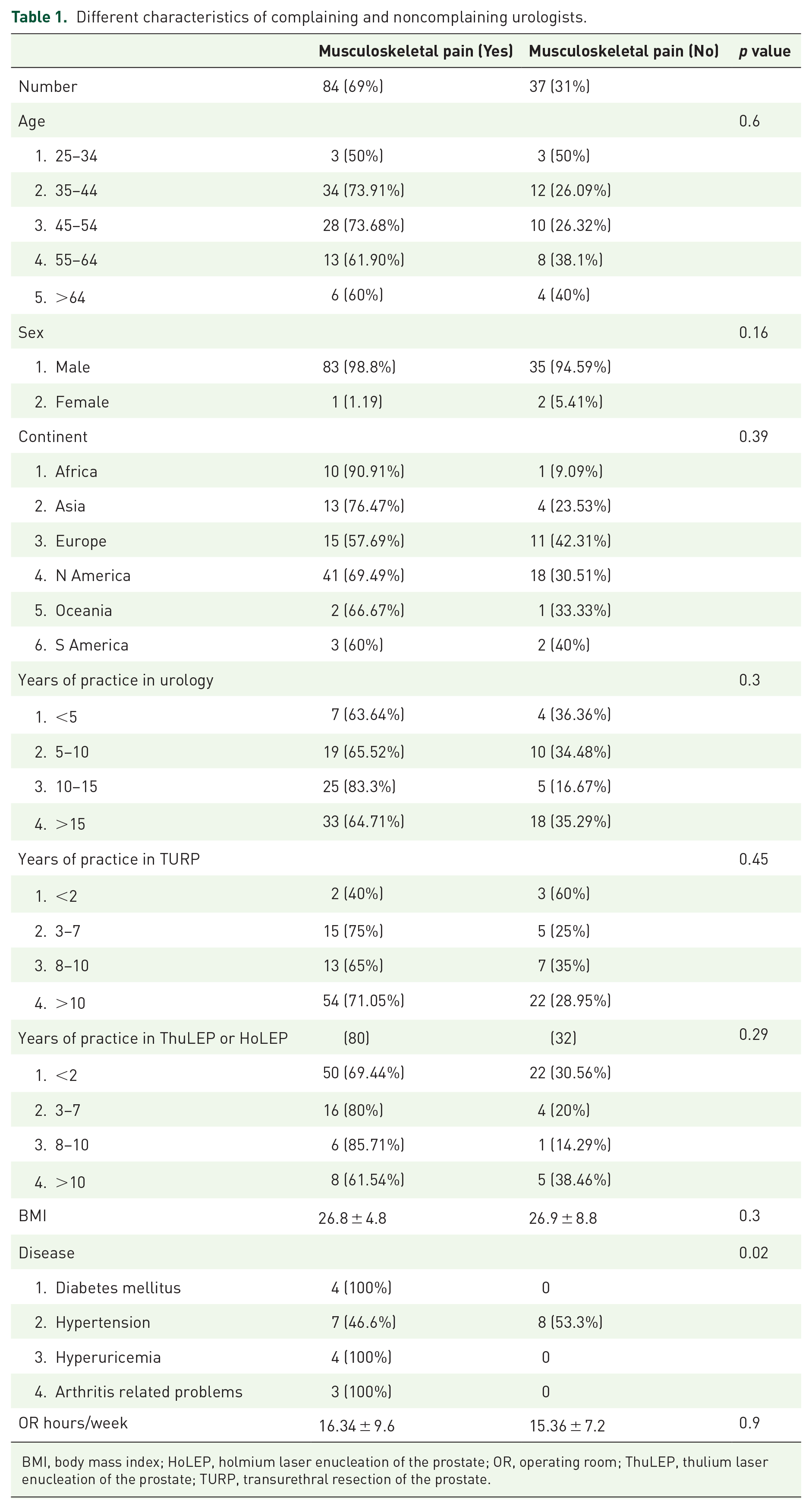
BMI, body mass index; HoLEP, holmium laser enucleation of the prostate; OR, operating room; ThuLEP, thulium laser enucleation of the prostate; TURP, transurethral resection of the prostate.
Endourologists experiencing musculoskeletal symptoms were more likely to suffer from diabetes, hyperuricemia, and arthritis-related problems (Table 1). The number of surgeries and operation room hours, the operating position (standing versus sitting), dominant hand, corrective eye wear, type of the working element, previous surgery in the dominant hand, and type of the endoscopic monitor did not affect the risk of symptoms (Table 2).
Operative related differences between complaining and non-complaining urologists.

HoLEP, holmium laser enucleation of the prostate; ThuLEP, thulium laser enucleation of the prostate; TURP, transurethral resection of the prostate.
Larger estimated average prostate volume resected correlated significantly with the risk of musculoskeletal symptoms (76 g versus 59 g, p = 0.004) and the risk of more severe symptoms. The most frequent region for discomfort was the neck (64%), followed by back (57%), shoulder (48%), hand (40%), and elbow (18%). Five surgeons reported either discontinuing a surgery due to severity of symptoms or postponing additional surgeries that day.
About 53% of endourologists reported using a complementary strategy such as ice, heat and stretching for relieving their symptoms, whereas nonsteroidal anti-inflammatory drugs were used by 20% and muscle relaxants by 11% of surgeons. Most of the surgeons denied attributing their symptoms to a specific brand of working element but 71% either partially or completely attributed their symptoms to performing TURP and laser prostatectomy.
Discussion
The inception of the endoscopic management of bladder outlet obstruction and BPH can be traced to 1926 12 when Maximilian Stern introduced the first resectoscope with the tungsten wire loop. With the advancements of the Hopkins lens system and diathermy machine, TURP replaced open prostatectomy as the gold standard for surgical therapy of BPH. Subsequently, Gilling and Fraundorfer 13 introduced the HoLEP with a shorter hospital stay and more durable urinary symptom improvement. 14
Although endoscopic approaches have been demonstrated to be successful for even the super large prostate,14,15 the increased operative time has been associated with work-related pain and musculoskeletal symptoms in the surgeon. Stucky, 16 reported that performing minimally invasive surgery (MIS) was associated with pain in the back, neck, and shoulder, and a higher risk of fatigue compared with surgeons performing open surgery. To our knowledge, this is the first survey that evaluates the musculoskeletal burden of TURP and laser prostatectomy on the surgeon. We report that 69% of surgeons performing endoscopic BPH procedures experience musculoskeletal pain.
Others have reported that minimally invasive surgeons are prone to a higher risk of neurologic complications such as cervical spinal stenosis, 17 lumbar disc herniation, 18 or carpal tunnel syndrome. 19 Tjiam and colleagues 20 reported that 40% of Endourology Society members had poor or no knowledge of surgical ergonomics. Despite the implementation of endoscopic cameras and video monitors, ergonomic positioning of the monitor and the surgery table is important to minimize the musculoskeletal strain associated with bad posture. 21
In our study, prostate size resected was associated with a higher risk of musculoskeletal symptoms and a higher severity of symptoms if the prostate resected was more than 80 g. This suggests that prolonged sitting or standing in an abnormal position may place an added strain on the surgeon. According to European Association of Urology guidelines, 22 the best results for TURP are obtained if the weight of the prostate gland is below 50–60 g. The residual prostatic weight can lead to negative outcomes following endoscopic prostatectomy. 23 As such, surgeons would be inclined to extend their resection time for larger prostates, leading to a higher risk of strain.
Overall 53% of endourologists reported practicing ergonomic exercises in the form of stretching and rolling to improve their symptoms. Chung and colleagues 24 reported that exercise appears protective only in a dose-related fashion, with those exercising more than four times per week experiencing greater relief of symptoms.
Endourologists from developing regions (Africa, Asia) were more prone to report musculoskeletal symptoms. This could be attributed either to differences in instrumentation, surgical technique or less awareness of ergonomic considerations during surgery.
Our study is limited by the small sample size and low survey response rate. Although we report correlations between musculoskeletal symptoms and comorbidities such as diabetes and arthritis, larger populations would need to be studied to evaluate this relationship.
Conclusion
A high prevalence of musculoskeletal complaints among urologists performing endourologic prostatectomy is confirmed and proportionally related to size of the prostate. The integration of an ergonomic specialist inside the operation room to watch and correct the surgeon’s position during the endourologic procedure may reduce the endourologist’s exposure to these occupational hazards.
Supplemental Material
appendix1 – Supplemental material for Ergonomics and musculoskeletal symptoms in surgeons performing endoscopic procedures for benign prostatic hyperplasia
Supplemental material, appendix1 for Ergonomics and musculoskeletal symptoms in surgeons performing endoscopic procedures for benign prostatic hyperplasia by Mohamed Omar, Mohamed F. Sultan, Eid El Sherif, Mohamed M. Abdallah and Manoj Monga in Therapeutic Advances in Urology
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Ethical approval
Our study did not require an ethical board approval because it didn’t contain human or animal trials.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.