
Abstract
Background:
The three-way indwelling urinary catheter (IUC) is used for continuous bladder irrigation and is considered the cornerstone for clinical treatment of patients with macroscopic hematuria. Although there seems to be a logical relationship between catheter size and efficacy of irrigation and drainage, we often observe relevant variations in these parameters between different brands of catheters available on the market. The aim of this study was to compare the mechanical properties of different models of latex and silicone three-way catheters in an in vitro setting that resembles clinical use.
Methods:
Three different three-way catheters were evaluated: Gold Silicone-Coated Rusch® (Model A), 100% Silicone Rusch® (Model B) and X-Flow Coloplast® (Model C). Irrigation channel, drainage channel, and overall cross-sectional areas were all digitally measured. Irrigation and drainage channel flow rates were measured and correlated with their corresponding catheter cross-sectional area values.
Results:
Different catheter models of the same caliber have different internal irrigation port diameters, internal drainage port diameters and internal cuff port diameters. The Model C IUC internal irrigation port diameter is significantly larger than models A and B. When flows were evaluated, we found that in the same model, the increase in caliber of the IUC was related to an increased drainage flow, but not to an increased irrigation flow.
Conclusion:
Precise measurements of the internal architecture of the three-way catheter, rather than relying on the caliber itself, could assist surgeons in choosing the best product for each specific patient, while minimizing complications.
Background
Continuous bladder irrigation (CBI) is the cornerstone for the clinical treatment of patients with macroscopic hematuria. Three-way indwelling urinary catheters (IUCs) with CBI are used to prevent or manage blood clots and consequent urinary retention. 1
CBI is based on a gravity-driven principle, in which saline flows from a hanging bag to the IUC. Thus, knowledge of the properties of the different equipment materials used is extremely important because it can influence irrigation and drainage processes.
The caliber of an IUC, measured in French (Fr), refers not to the lumen size, but to the overall external circumference. A three-way IUC allows for an irrigation system as well as a drainage port; however, it has a smaller internal drainage lumen than an equivalent size two-way catheter. 1
Inappropriate IUC selection, resulting in inadequate infusion or drainage rates, may cause severe adverse effects, such as bladder spasm, hemorrhage and clot retention. 1
Currently, the choice of IUC is mainly based on cost, availability and specific hospital stocking preferences. The surgeon’s opinion will only be taken into account if objective data support one product over another.
Given the myriad of available devices, there is a lack of comparative data on their effectiveness. Our objective was to systematically compare the mechanical properties and fluid dynamics of different models of latex and silicone three-way IUCs, as well as the variables that can worsen or enhance their performance, in an in vitro setting that resembles clinical use.
Materials and methods
Overall, three different three-way IUCs, each in three different sizes, were evaluated. The catheter model selection was based on the market share in our institution (Hospital Israelita Albert Einstein).
A 20-Fr, 22-Fr and 24-Fr Gold Silicone-Coated Rusch® (Model A); 20-Fr, 22-Fr and 24-Fr 100% Silicone Rusch® (Model B) and 20-Fr, 22-Fr and 24-Fr X-Flow Coloplast® (Model C) were studied.
Three different IUCs of each specific model and size were tested to diminish eventual biases.
Physical properties
To analyze the uniformity of the opening area of each channel, a perpendicular cross-sectional cut of the catheter was performed with a scalpel in three different portions: proximal (at the end of the connection head), middle-section (in the exact mid portion of the catheter) and distal (just before the cuff of the catheter; Figure 1).

(a) Formula used to calculate the area of the catheter; (b) Different portions of the IUC where the cross-sectional area was calculated; (c) IUC cross-section with total external diameter, internal irrigation port diameter, internal drainage port diameter and internal cuff port diameter.
After preparation, the samples were conditioned at 23 ± 2°C and 50 ± 5% relative humidity for a period of 40 h, because polymeric materials have great dimensional variation with changes in temperature and humidity.
In each portion, the following characteristics were evaluated: the total external diameter, internal irrigation port diameter, internal drainage port diameter and internal cuff port diameter.
To evaluate the diameters, the samples were positioned in the base of the profile projector (Mitutoyo®, Optical Comparator Type PJ-250C with a resolution of 0.005 mm and ×10 magnification), using the diagonal projection, so that all the outside diameters were perfectly displayed. Because the channel of the probes and their respective apertures are not perfectly circular, the ellipse area formula (A [ellipse area] = a [larger radius] × b [smaller radius]) was adopted as a method of calculating the area of the apertures (Figure 1).
After performing the measurements of three different catheters in each specification, the mean values were calculated and adopted for further comparisons.
In the most distal section of each catheter (section 3), the number of external orifices, the area of each isolated orifice, and the sum of the areas of all orifices were also measured. All irrigations orifices were lateral (Figure 2).

Number of distal orifices and irrigation of each catheter: (a) Gold Silicone-Coated Rusch®, (b) Silicone Rusch®, (c) Coloplast®.
Irrigation
Continuous irrigation was evaluated in 16 common clinical scenarios, all with maximum irrigation flow. A 500 ml Baxter® saline irrigation bag was suspended either 180 or 198 cm above the floor and a 4-mm diameter Hartmann® irrigation line was attached to the irrigation port of each catheter. The IUC was held in a horizontally position and kept either at 65 or 90 cm above the floor (Figure 3).

Irrigation flow analysis scheme.
Respecting the height variations between the bag and the catheter, the distance variation was determined in all the different situations: bag 190 cm/IUC 65 cm (⊗1 = 125 cm); bag 180 cm/IUC 65 cm (⊗2 = 115 cm); bag 190 cm/IUC 90 cm (⊗3 = 100 cm); bag 180 cm/IUC 90 cm (⊗4 = 90 cm).
Additionally, the IUC cuff was tested empty or inflated with 10, 20 or 40 ml of air. A picture of the inflated balloon configuration and its relationship with the drainage orifices is shown in Figure 4.

All catheters were inflated with 20 ml of air. (a) Gold Silicone-Coated Rusch®, (b) Silicone Rusch®, (c) Coloplast®.
A SF-TP Urozamm® collecting bag was attached to the drainage port. The infusion flow was measured when placing the IUC tip facing a urodynamic collecting funnel, and its precision weight balance was recorded. The sequence of adjustments for the urodynamic device (Dynamed®) was: press the ‘Play’ key, select ‘Acquisition’, ‘Adjust’ and then ‘Zero’. After such sequence, recording was started by selecting the ‘Rec’ option.
The experimental procedure of this study consisted of opening the equipment in maximum flow, interrupting the flow when the desired volume of study was reached (500 ml), which was indicated by the software itself. At this point, the option ‘Stop’ was pressed, then ‘Report’, ‘Analyze Exam’ and ‘View Report’. The procedure was repeated three times for each catheter.
A total of three probes of each model were used. As there was no difference in flow between the probes of the same model and size, we used the second test performed in each model and size as the reference value for the analyses.
Drainage
To analyze drainage, we created a model in which the proximal end was coupled to the collection bag at a predetermined height, while the other end was coupled and sealed to a container containing 1 l of saline. During the test, the cuff was filled with 0, 10 ml, 20 ml or 40 ml of air. The test was completed when 500 ml of liquid was drained.
Drainage flow was measured using the same apparatus used in the infusion analysis.
All models and sizes were tested with the combinations of 198 cm/65 cm, 198 cm/90 cm, 180 cm/65 cm and 180 cm/90 cm of the saline bag support and the IUC height, respectively.
The flow was evaluated using the Dynamed® urodynamic apparatus (model Dynapack) and each study was repeated three times.
For this study, the friction loss due to the length of the probes was negligible in view of its relatively small length.
Statistical analysis
Data sets were grouped for each catheter and then compared using analysis of variances.
Results
Physical properties
Different models of a same caliber IUC have different internal irrigation port diameters, internal drainage port diameters and internal cuff port diameters (Table 1).
Average of the internal lumen’s area based on the three section divisions.

The irrigation port external orifice area is similar among the different calibers of the same IUC model. However, it varies significantly among the different models (Table 1).
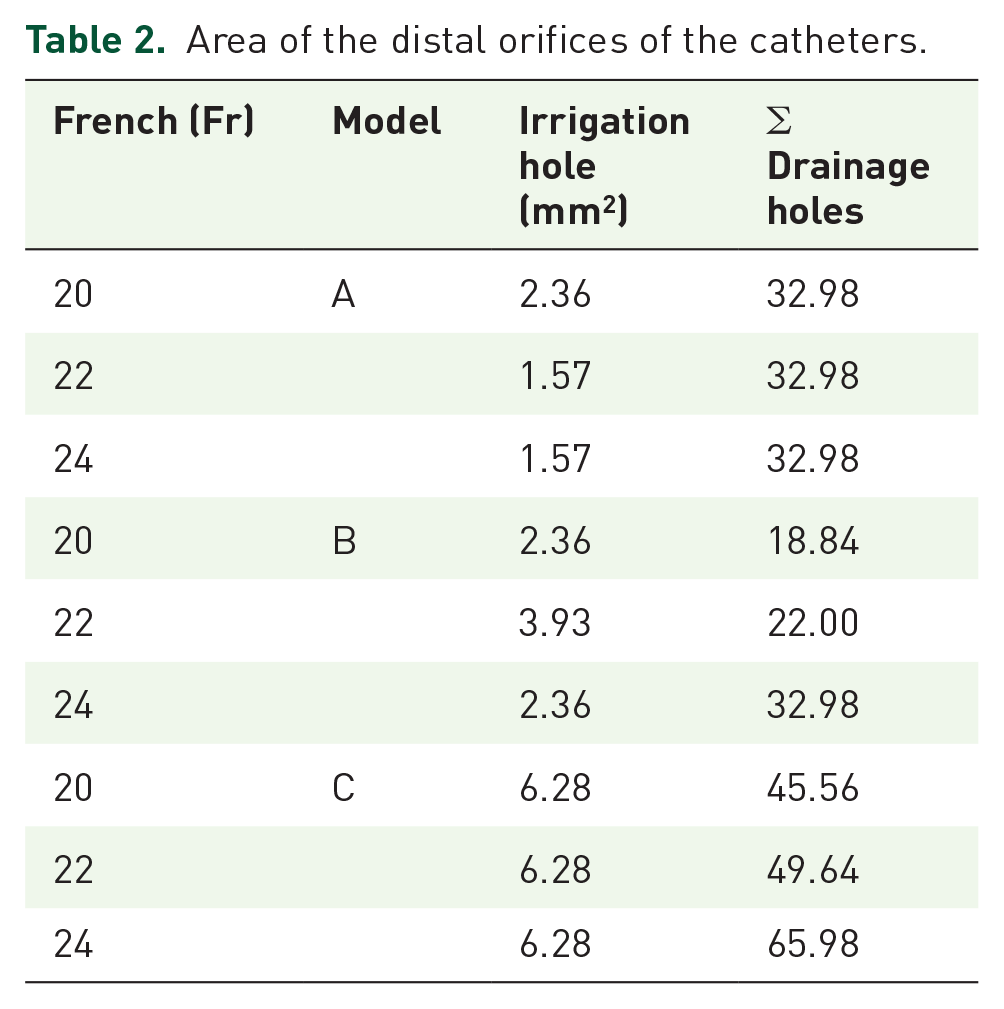
The total area of the external drain holes was obtained by summing the areas of all orifices. Regardless of the caliber of the IUC, the external drainage hole remained the same in Model A, but increased in Models B and C, as the caliber (French) increased (Table 2).
Area of the distal orifices of the catheters.
Wall thickness was calculated by subtracting the areas corresponding to irrigation, drainage and cuff channel from the total area of the catheter (Table 3).
Wall thickness was calculated by subtracting the areas corresponding to irrigation, drainage and cuff from the total area of the catheter.

Irrigation and drainage flow
When flows were evaluated, we found that in the same IUC model, the increase in caliber was related to an increased drainage flow, but not to an increased irrigation flow. However, when comparing different IUC models, both irrigation and drainage flows in Model C IUC were greater than their equivalent caliber of Models A and B IUCs (Tables 4 and 5).
Drainage flow study (500 ml × time in min).

IUC, indwelling urinary catheter.
Irrigation study. 500 ml × time in min. Δ1: 125 cm (bag irrigation 190 cm/IUC 65 cm); Δ2: 100 cm (irrigation 190 cm/IUC 90 cm); Δ3: 115 cm (irrigation 180 cm/IUC 65 cm); Δ4: 90 cm (irrigation 180 cm/IUC 90 cm).

IUC, indwelling urinary catheter.
The volume injected into the cuff did not interfere with infusion and drainage flows in all models (Tables 4 and 5).
Discussion
This study shows that there are significant differences among three-way IUCs and provide a scientific basis for appropriate selection within the clinical practice. The irrigation flow correlates better to the IUC model than to the IUC caliber. On the other hand, the drainage flow, besides varying from one IUC model to the other, also increases proportionally with the IUC caliber.
Every clinical situation leads to a particular kind of hematuria, which can be managed with a greater or lesser irrigation flow in order to prevent complications. 2 Some patients presenting with lower urinary tract bleeding must undergo efficient and effective catheter irrigation. 3 In addition, clot retention is a serious situation encountered after transurethral procedures, and a significant challenge for the patient and urologist. Several studies comparing surgical techniques for transurethral prostate or bladder resection have reported complications related to hematuria; however, without an understanding of the IUC model and caliber used in the patient population it is difficult to attribute these complications to the surgical technique or postoperative care.4,5
Our literature search could not find studies that determined the main risk factors responsible for bladder clot formation. However, one may hypothesize that both irrigation and drainage flows are important aspects. Intuitively, during a hemorrhagic emergency, the greater-caliber IUC tends to be chosen. 6 However, our study clearly demonstrates that knowing the available IUC properties in detail is paramount, because a greater-caliber IUC does not directly correlate with a better irrigation flow.
The 20-Fr Model C IUC has a larger internal irrigation port diameter than the calibers of Model A and Model B IUCs. It is 48% larger than Model A and 66% larger than the Model B 20-Fr IUC. In the 22-Fr catheters, Model C has a diameter 45% larger than Model A and 39% larger than Model B. In the 24-Fr probes, Model C has a 47% larger diameter than Model A and 64% larger than Model B.
Additionally, the Model C irrigation port external orifice presents a greater total orifice area, which is 2.5 times greater than Model B and four times greater than Model A. In the 20-Fr catheters, Model C presents a diameter 11% greater than Model B and 52% greater than Model A. In the 22-Fr catheters, Model B and C have similar diameters, both being 41% greater than Model A. In the 24-Fr catheters, Model C and B are similar and 29% greater than Model A.
When flows were evaluated, we found that in the same model, the increase in caliber of the IUC is related to an increased drainage flow, but not to an increased irrigation flow. However, the 20-Fr Model C IUC presented an irrigation flow that was 45% greater than the 24-Fr Model A IUC and 56% greater than the 24-Fr Model B IUC. Therefore, in cases of gross hematuria, if the doctor requires a more abundant infusion flow, it is necessary to change the model and not the size of the catheter.
Another important finding of this study is that there is no alteration of flow related to the volume of the cuff. Although there is a maximum volume accepted by each specific IUC, which is determined by the manufacturer, the amount of saline used to insufflate the cuff varies from a surgeon to the other. Thus, one may over-inflate the cuff and temporarily place traction into the IUC in order to squeeze the bladder neck and diminish the prostatic bleeding without worsening the irrigation flow.
Braasch and colleagues also noted variations in bladder irrigation and drainage when using catheters from different manufacturers. 1 The size of the catheter, measured in Fr, refers to the external circumference and not to the lumen. As with our study, they found that different IUC models with the same external circumference may present different cross-sectional areas (CSAs). 1
Davis also noted that Fr values and the catheter CSA did not predict flow-rate characteristics, but the irrigation channel CSA and the drainage channel CSA were predictive. He proposed a catheter labelling system to include the overall CSA, irrigation channel CSA, and drainage channel CSA values to provide more accurate and transparent data relevant to anticipated drainage and irrigation flow rates. 7 Similarly, our study also shows that the size of the catheter does not provide the success of the drainage or of the irrigation. Our study is the first to critically analyze the functional properties of the new Coloplast catheter.
In addition to the catheter external size, its port calibers and the total orifice area, there may be other factors that influence their selection for clinical use. It is known that most of the catheters are made of latex, silicone, polyvinyl chloride or latex coated with hydrogel. Although there are no randomized clinical trials looking at patient comfort, it is known that all these materials may cause urethral discomfort and can influence the hospital cost.8,9 Additionally, each material has an inherent peculiarity due to its composition: the latex absorbs water, which causes the catheter to swell, which in turn reduces the internal diameter and increases the external diameter. The polyvinyl chloride catheters are more rigid than the other catheters and might cause pain in some patients. The silicone hydrogel coated coloplast urethral catheter is made of a more inert material compared with the urethral mucosa, which could eventually make the catheter more comfortable to use, easier to insert, and more resistant to bacterial colonization. 10
It is believed that bladder compliance may also play an important role. Under a low-resistance pressure system, the flow of irrigation is facilitated, which should increase the efficiency of the inflow. Unfortunately, this comparison was not made in this study. Another factor that was not analyzed was the negative pressure required to collapse each type of catheter studied. We imagine that the more resistant to this factor the catheter is, the better the drainage, especially when there are multiple bladder clots. In addition, a catheter that does not collapse would be more amenable to forceful hand irrigation. Finally, the number of catheter models analyzed was limited to three and only one specimen of each catheter size was tested.
Conclusion
Different IUC models with the same external caliber have significantly disparate irrigation and drainage lumen calibers, that consequently yield different irrigation and drainage flows.
Understanding the properties of each IUC available facilitates the selection of the appropriate device that should be used in each clinical setting.
Future in vivo experiments must be performed to validate these in vitro findings.
Footnotes
Acknowledgements
Arie Carneiro, Marcelo Wroclawski and Alides Maria Mendes Rasabone Garcia drafted the manuscript and worked on the article’s concept.
Guilherme Andrade Peixoto, Jonathan Doyun Cha, Natasha Kouvaleski Saviano Moran, Felipe Ko Chen performed the lab experiments supervised by Arie Carneiro.
Arie Carneiro, Marcelo Wroclawski, Henrique Nelson Satkunas and José Roberto Augusto Campos designed and interpreted the data.
Arie Carneiro, Marcelo Wroclawski, Manoj Monga and Gustavo Caserta Lemos were involved in the interpretation and discussion of the results and critically revised the final paper for important intellectual content.
Maria Beatriz Lemos was the research team coordinator.
All authors approved the final version of the systematic review.
Arie Carneiro and Marcelo Langer Wroclawski are first authors for this paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.