
Abstract
Renal oncocytoma is a benign epithelial neoplasm typically composed of large cells with granular eosinophilic cytoplasm. Although rare, histologically worrisome features such as vascular and perinephric fat invasion have been reported. Of the 159 renal oncocytomas resected at our institution, 20 (12.6%) had vascular and/or perinephric fat invasion. Microscopically, 10 oncocytomas had perinephric fat invasion, 7 had vascular invasion and 3 had both vascular and perinephric fat invasion. Grossly, perinephric fat invasion was visible in three cases and tumour was identified within the branches of the renal vein in two cases. Tumours occurred in 14 men and 6 women (M:F = 2.3:1). The mean age at diagnosis was 64.5 years (range, 33–88 years). A total of 11 cases had radical nephrectomies while 9 cases had partial nephrectomies. There was no evidence of disease recurrence, metastasis or death due to tumour after a mean follow up of 25.6 months (range, 2–103 months). The presence of vascular and perinephric fat invasion in renal oncocytoma though worrisome, does not alter the benign course of the tumour.
Introduction
First described by Zippel in 1942 1 and later by Klein and Valensi in 1976, 2 oncocytoma accounts for approximately 5–9% of all renal epithelial neoplasms, 3 and comprises 10–15% of enhancing small renal masses (⩽ 4 cm). 4 Thought to arise from intercalated cells of renal collecting tubules, oncocytoma is a benign renal epithelial neoplasm typically composed of large cells with granular eosinophilic cytoplasm.5,6
Although rare, both vascular and perinephric fat invasion have been described. The reported incidence of perinephric fat invasion ranges from 2% to 20% 7 and vascular invasion occurs in up to 5.4% of cases. 8 The presence of vascular and perinephric fat invasion is particularly worrisome as invasion is considered a feature of malignancy in renal cell carcinoma (RCC) and would warrant pT3a disease staging.
Furthermore, in a survey of 17 urological pathologists regarding the diagnostic criteria for oncocytic renal neoplasms, 10 (59%) respondents indicated that perinephric fat invasion was unequivocally compatible with a diagnosis of oncocytoma. Six (35%) of those surveyed reported that vascular invasion was compatible with an oncocytoma diagnosis. 9 The survey emphasizes the persisting uncertainty in the diagnosis of oncocytoma, particularly in the presence of worrisome histological features, hence the need to further characterize this tumour.
We present the clinical and pathological features of renal oncocytoma with vascular and perinephric fat invasion including clinical follow up.
Methods
A total of 159 oncocytomas resected at Imperial College Healthcare NHS Trust, London from 2004 to 2018 were retrieved from the archives of the Department of Cellular Pathology. Biopsy specimens were excluded from this study.
Slides and surgical pathology reports of oncocytoma with vascular and/or perinephric fat invasion were reviewed by the authors. The cases were assessed for clinical and pathological data including specimen type, laterality, tumour size, morphology, perinephric fat invasion, vascular invasion, coexisting neoplasms, presence of necrosis, atypia and mitosis. Follow-up data were obtained from electronic medical records.
Results
Of the 159 renal oncocytomas resected at our institution, 20 had vascular and/or perinephric fat invasion. The demographic characteristics, clinical and pathological findings of the 20 cases are summarized in Table 1. A total of 10 had perinephric fat invasion, 7 had vascular invasion and 3 had both vascular and perinephric fat invasion. There were 14 men and 6 women (M:F = 2.3:1) and the mean age at diagnosis was 64.5 years (range, 33–88 years). A total of 11 cases had radical nephrectomies while 9 cases had partial nephrectomies. Of the 10 cases with vascular invasion, 3 were partial nephrectomies. The right kidney was involved in 11 cases and the left kidney in 9 cases. All cases were unifocal and no bilateral tumours were identified.
Clinical and pathological data of 20 patients with renal oncocytoma.
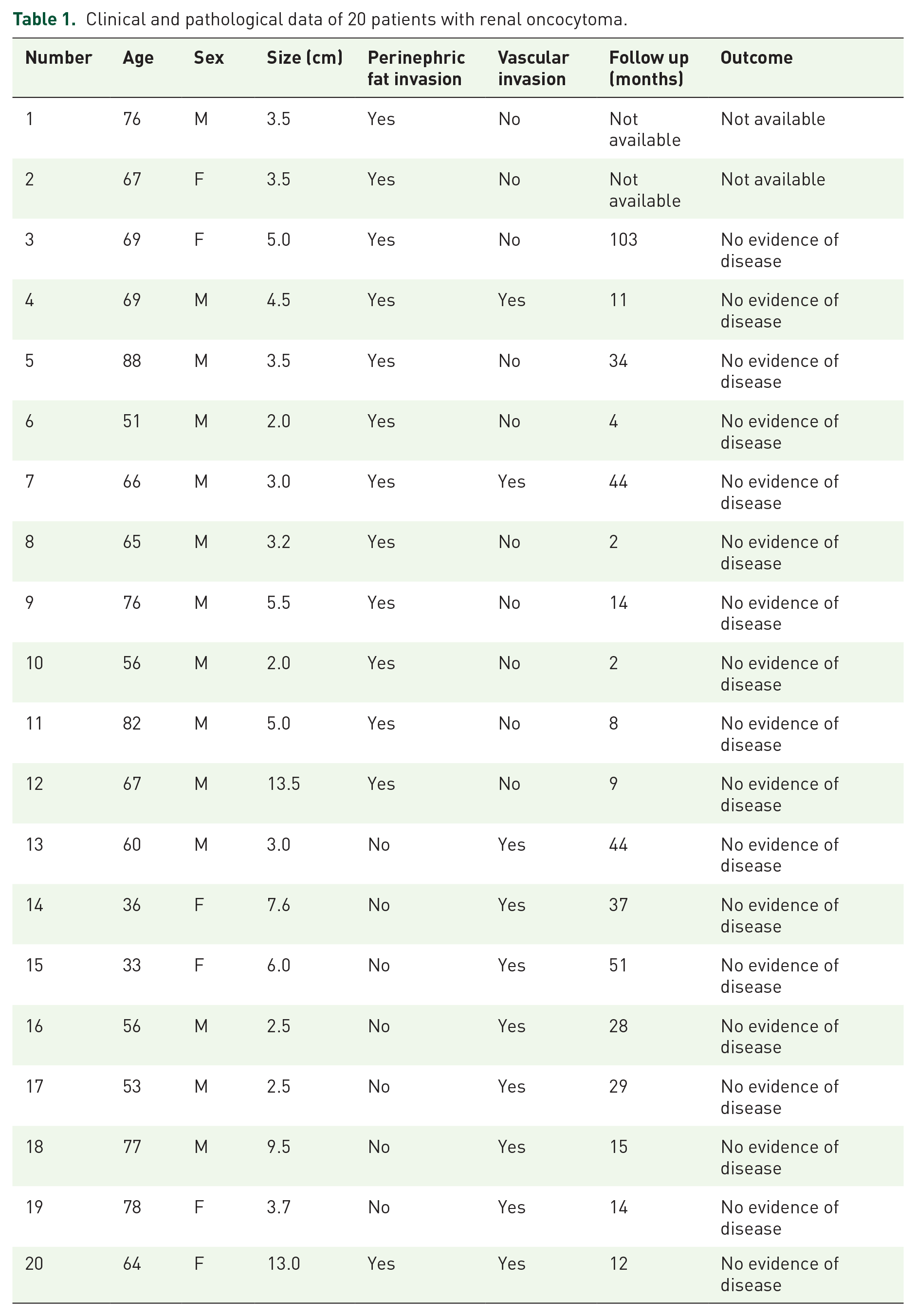
Grossly, the tumours were well circumscribed and unencapsulated with tan to mahogany-brown cut surfaces. Tumour size ranged from 2 cm to 13.5 cm (mean, 5 cm). Two oncocytomas had a central stellate scar. Two patients had coexisting neoplasms including papillary adenoma and chromophobe RCC (ChRCC). The main tumour mass in both patients was oncocytoma and vascular invasion was by oncocytoma only. Grossly, perinephric fat invasion by oncocytoma was seen in three cases and the three tumours ranged from 3.2 cm to 5.0 cm in diameter. The two cases with grossly visible vascular invasion were radical nephrectomies and tumour sizes were 3 cm and 9.5 cm. The vascular and surgical resection margins of all specimens were free of tumour.
Microscopically, the tumours were well circumscribed with a solid-nested growth pattern. One case had a mixed architecture including solid-nested and tubulocystic growth patterns. The tumours were composed of large round to polygonal cells with densely granular eosinophilic cytoplasm set within loose oedematous connective tissue stroma. The lesional cells had uniform nuclei with smooth nuclear membranes, evenly distributed chromatin and a small central nucleolus. There was no evidence of necrosis. No sarcomatoid or clear-cell change was seen. One case had one mitotic figure and upon meticulous search, two mitotic figures were identified in a second case. No abnormal mitoses were identified. Four cases showed focal dystrophic calcification and occasional haemosiderin-laden foamy macrophages were identified. Isolated foci of degenerative nuclear atypia were noted including hyperchromatic and smudged chromatin forms.
Perinephric fat invasion was focal with a well-defined interface between fat and tumour. No desmoplastic tissue reaction was seen (Figure 1).
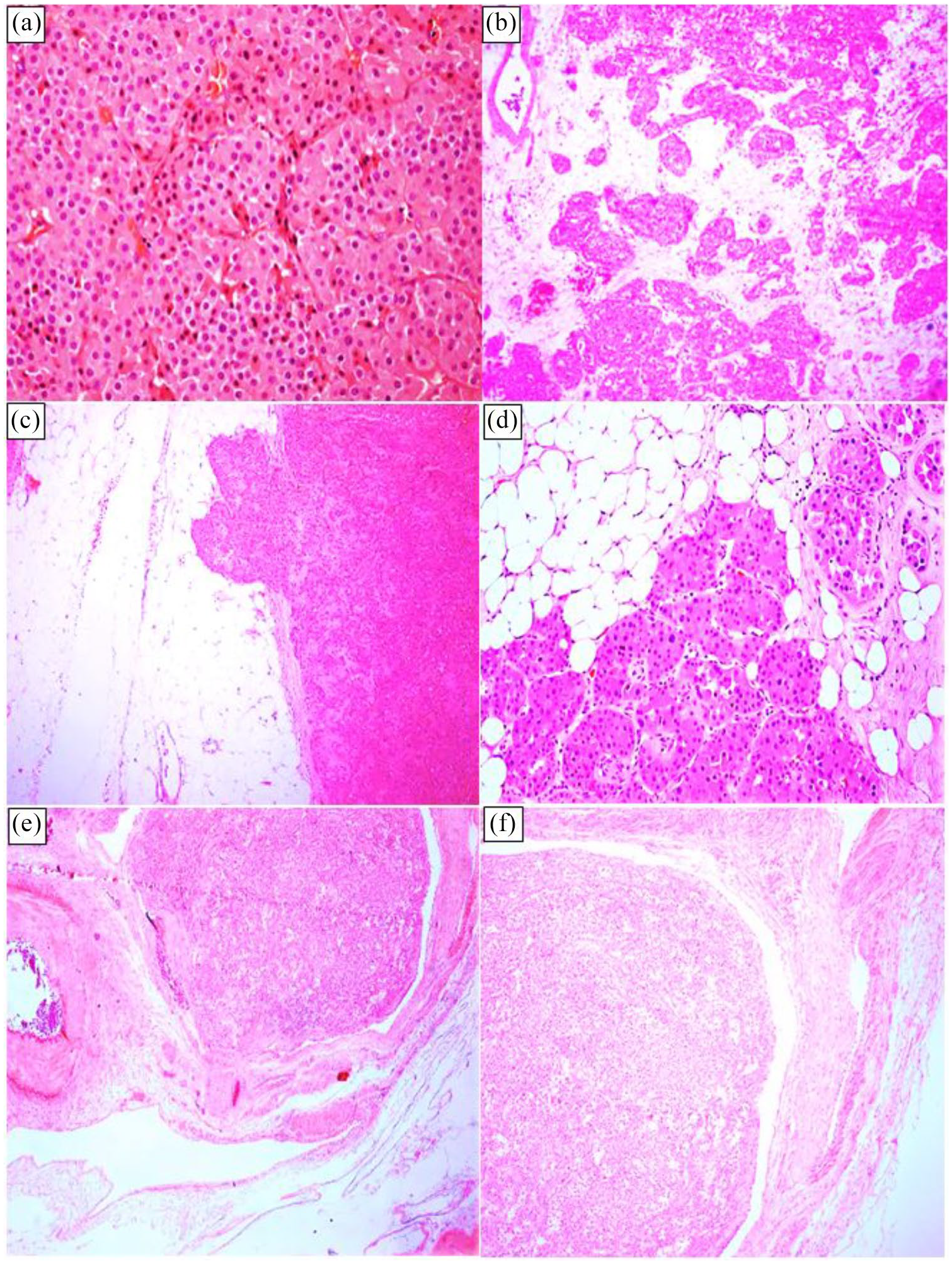
(a) Oncocytoma with a solid growth pattern and composed of polygonal cells with densely granular eosinophilic cytoplasm; (b) oncocytoma set within loose hypocellular connective tissue stroma; (c) and (d) oncocytoma with perinephric fat invasion; (e) and (f) oncocytoma with vascular invasion.
Tumour was identified within the branches of the renal vein. Plugs of tumour were also seen within variably sized vessels with focal adherence to the vessel wall in a few cases. Although few cases had scattered lesional cells which expressed CK7, the vast majority of tumours were negative.
Follow-up information was available for 18 patients. There was no evidence of disease recurrence, metastasis or death due to tumour after a mean follow up of 25.6 months (range, 2–103 months).
Discussion
Renal oncocytoma is a benign epithelial neoplasm composed predominantly of large, round to polygonal cells with granular eosinophilic cytoplasm. The nucleus is round with finely distributed chromatin and inconspicuous nucleoli. 3 Typically, tumour cells are arranged in a solid-nested pattern or small islands of eosinophilic cells within loose oedematous stroma. Other patterns including tubulocystic and mixed may be present. Although oncocytes are the predominant cell type, occasionally, small cells (oncoblasts) with scanty cytoplasm, hyperchromatic nuclei and a high nuclear: cytoplasmic ratio may be present. 3 A central stellate scar, though not unique to renal oncocytoma, may be seen in up to 32.1% of cases. 6
Renal oncocytoma has been associated with some atypical features including vascular invasion, perinephric fat infiltration, focal clear-cell changes typically within hyalinized areas, 6 and rarely, focal papillae within tubular and cystic areas. 3 Mitoses, though vanishingly rare in oncocytoma, have been reported in the literature.3,6,7,10 Features considered incompatible with the diagnosis of oncocytoma include extensive necrosis, significant mitotic activity including atypical forms, sarcomatoid areas, diffuse or conspicuous papillary growth pattern and prominent clear-cell change.3,10
Both vascular and perinephric fat invasion in renal oncocytomas have been described in the literature. Trpkov and colleagues in a study of 109 cases identified 17 (15.6%) oncocytomas with perinephric fat invasion and 4 cases (3.7%) with vascular invasion. 6 The median follow up was 52 months (range, 1–113 months). All patients were free of recurrent and metastatic disease. There was no death due to tumour. Trpkov and colleagues concluded that these features, though problematic, fall within a spectrum of morphological changes seen in renal oncocytoma. 6
Amin and colleagues in a study of 80 cases from 2 institutions identified 9 cases (11.3%) with perinephric fat invasion. No vascular invasion was reported in the study. There was no evidence of recurrent disease, metastasis or death as a result of tumour after a mean follow up of 91.5 months (range, 15–200 months). 10
Perez-Ordonez and colleagues studied 70 oncocytomas and reported perinephric fat invasion in 14 cases (20%). Three patients (4%) had vascular invasion: one had invasion of capillary-sized vessels whereas the other two had invasion of venous-type vessels. 7 The mean follow up was 58 months (range, 1–181 months). A total of 62 patients (89%) were alive with no evidence of disease, 6 (9%) died from unrelated causes, 1 was alive with stable metastatic disease in the liver and 1 died with metastatic disease to the liver and bone. 7 Of the three patients with vascular invasion, one remained free of tumour at 48.9 months of follow up. The second patient had liver metastasis, which was confirmed by needle biopsy at the time of nephrectomy. After 14 years of follow up, there was no change in size of the liver lesion and no evidence of tumour recurrence.7,11 The third patient reportedly developed liver and bone metastases. However, the metastases were not proven by tissue diagnosis. 7
In a series of 1474 renal oncocytomas from 3 institutions, the authors reported vascular invasion in 22 cases (1.5%). The mean follow up was 29.9 months (range, 7.5–94.5 months). 11 Of the cases with follow-up data, all but one patient was alive, and the cause of death for this patient was not known. The patients were free of recurrent or metastatic disease. 11
Another review of 324 renal oncocytomas identified 7 cases (2.2%) with vascular invasion. After a mean follow up of 3.6 years (range, 1–5 years), all patients were alive without disease recurrence and metastasis. The authors concluded that the tumour may have intravascular extension into branches of the renal vein. In addition, renal oncocytomas with vascular invasion share identical morphological, immunohistochemical and cytogenetic features with oncocytomas without vascular invasion. 12
Our study is comparable in many respects with other studies. The incidence of vascular and perinephric fat invasion in our series was 6% and 8%, respectively. Most of the tumours showed characteristic solid-nested architecture with tan to mahogany-brown cut surfaces. Perinephric fat invasion was focal and did not elicit desmoplastic reaction in surrounding tissue. In addition, our series showed invasion of variably sized vessels with gross involvement of branches of the renal vein. All patients with clinical follow-up data were alive and free of recurrent and metastatic disease.
Vascular invasion has also been described in other rare benign renal neoplasms including anastomosing haemangioma 13 and mixed epithelial and stroma tumour of the kidney. 14 The presence of vascular invasion does not appear to affect the excellent prognosis associated with these tumours.
The morphologies of most renal neoplasms are well characterized and often do not require ancillary tests. However, oncocytic renal neoplasms may be challenging. The differential diagnosis of oncocytic renal neoplasms include oncocytoma, oncocytic papillary RCC (PRCC), succinate dehydrogenase (SDH)-deficient RCC, eosinophilic, solid and cystic RCC (ESC RCC) and eosinophilic variant of ChRCC.
Oncocytic PRCC, a proposed variant of PRCC, is a rare neoplasm characterized by predominantly papillary or tubulopapillary architecture. The papillae are lined by neoplastic cells with granular eosinophilic cytoplasm and oncocytic PRCC does not require immunohistochemistry (IHC) for diagnosis. 15
SDH-deficient RCC is composed of neoplastic cells with distinctive cytoplasmic vacuoles or flocculent inclusions that contain eosinophilic material. The loss of IHC staining for SDH complex II, subunit B and iron sulphur protein, a marker of dysfunction of the mitochondrial complex II, is a requirement for the diagnosis of SDH-deficient RCC. Most patients have germline mutations in one of the SDH genes. 3
ESC RCC, while not included in the 2016 World Health Organization classification of tumours of the urinary system, is a newly described neoplasm predominantly occurring in women. ESC RCC is characterized by cells with abundant eosinophilic cytoplasm, typical fine or coarse basophilic stippling, solid and cystic growth patterns, frequent CK20+/CK7– immunophenotype and an indolent clinical course.16,17
A common diagnostic challenge is distinguishing the eosinophilic variant of ChRCC and oncocytoma. ChRCC is characterized by cells with prominent cell membranes described as plant cell-like, wrinkled ‘raisinoid’ nuclei with perinuclear haloes, finely granular eosinophilic cytoplasm and diffusely positive CK7 immunophenotype. 3 The distinctive nuclear features of ChRCC are key to distinguishing oncocytoma from the eosinophilic variant of ChRCC. 18 The International Society of Urological Pathology recommends paying close attention to nuclear cytology and cytoplasmic features supplemented by IHC staining for CK7. 15
On the basis of our experience and the findings of other studies, we believe that renal oncocytomas have characteristic morphological features that allow for accurate diagnosis. The cases in our series were diagnosed based on morphology and supported by IHC for CK7. Tumour cells were mostly negative for CK7 although occasional focally positive cells were seen. Furthermore, we are of the opinion that the presence of necrosis, sarcomatoid areas, prominent clear-cell changes, prominent papillary architecture and widespread mitotic figures including atypical forms are not compatible with the diagnosis of renal oncocytoma.
We conclude that the presence of vascular and perinephric fat invasion is consistent with the diagnosis of renal oncocytoma and does not alter its benign course.
Footnotes
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.
Ethical statement
Our study did not require an ethical board approval because it did not contain human or animal trials.