
Abstract
Background:
Renal cell carcinoma (RCC) is one of the most common genitourinary malignancies. Programmed death ligand-1 (PDL1) is an immune checkpoint inhibitor, instrumental in ‘T cell escape’ of malignant cells. PDL1 has been shown to be associated with poor prognosis in multiple small studies. In this study, we want to study the role of PDL1 as a prognostic marker in RCC in an Indian population.
Methods:
A total of 30 patients who underwent radical or partial nephrectomy, with histopathological findings of RCC, were included in the study. PDL1 expression was studied in tumour tissue with immunohistochemistry. Patients were followed up for a period of 2 years for disease recurrence and cancer-specific mortality.
Results:
Expression of PDL1 was seen to be associated with higher grade and stage at presentation. PDL1 expression was also associated with statistically significant increased incidence of disease recurrence. Although cancer-specific mortality was higher in patients with positive PDL1 expression, it was seen to be statistically insignificant.
Conclusions:
PDL1 is a novel prognostic marker for RCC and is associated with poor prognosis. More studies with larger patient pool and multicentric studies will establish the role of PDL1 with certainty. This can be the torchbearer for the future management of RCC.
Keywords
Introduction
Renal cell carcinoma (RCC) is an adenocarcinoma accounting for 3% of all adult malignancies. 1 With increasing use of imaging, the rate of incidental discovery has increased manifold, and incidental discovery is now the most common presentation. The classical triad of gross haematuria, flank pain and palpable abdominal mass is now pigeon-holed as the ‘too late triad’.
Patient prognosis depends on multiple clinicopathological factors such as TNM stage, Fuhrman nuclear grade, tumour size and other haematological indices. 2 However, most of these factors correlate poorly with prognosis. Thus, there is need for new prognostication tools. 3
Investigation of the role of immunological pathways in tumour progression, as well as control, has been of interest in RCC, and has led, in turn, to the development of therapeutic agents with immunological intervention points such as interferon and IL-2. 4
Programmed death ligand-1 (PDL1) has been studied as a negative regulator of cytotoxic T cells, and potentiation of the antitumoural response has been observed after use of monoclonal antibodies directed against PDL1 in in vivo models. 5 These findings were the foundation of the search for the role of PDL1 as a prognostic marker and a possible therapeutic target. This has been studied in a few studies with small sample size; however, no such study has been carried out in the Indian population to date. In our study, we intended to study the role of PDL1 as a prognostic marker in RCC, in terms of stage at presentation, recurrence and cancer-specific mortality.
Materials and methods
Patients presenting with renal tumour to our institution were included in the study. Those who underwent palliative therapy and were not diagnosed with tissue diagnosis were excluded from the study. In total, 30 such patients who underwent either radical or partial nephrectomy and had RCC as the pathological finding were included in the study. Other pathological findings such as grade, resection margin, lymph nodes positivity and histopathological type were noted.
Expression of PDL1 was studied in the tissue samples of the resected specimen with immunohistochemistry. Abcam recombinant anti-PDL1 antibody (ab205921) was used for immunohistochemistry. PDL1 expression was graded semiquantitatively on a scale of 0–3+ as described by Choueiri and Figueroa and colleagues. 6
Patients were followed up at regular intervals with both in-clinic visits and over telephonic conversation over a minimum period of 2 years. Recurrence was documented with imaging and needle biopsy where needed. Both baseline and follow up data was assimilated. Data was analysed with the help of SPSS (24.0). Chi-squared test and Fischer exact test were used as appropriate.
Institutional ethical committee approval was obtained: approval no. IPGME&R/IEC/2017/337.
Results
The mean age of the study group was 55.3 years. The male:female ratio was 2:1; 73.3% of patients had a history of tobacco use and 16.6% had a history of addiction to alcohol. Out of 30 patients in our study group 2 were obese, with a body mass index (BMI) greater than 30; 20 (66.7%) were hypertensive; and 7 (23.3%) were diabetic.
The most common stage of presentation was stage I, with 17 (56.7%) cases. Eight cases (26.7%) presented with stage II and five cases (16.7%) presented with stage III. The most common histological grade was grade 1, with 16 cases (53.3%). Three cases were grade 2 and the remaining 11 cases were grade 3. There were nine cases of recurrence and five cases of cancer-specific mortality in the 2-year follow-up period. A total of 19 cases were operated with radical nephrectomy and, in 11 cases, partial nephrectomy was performed.
A total of 11 (36.7%) samples of tumour tested positive for PDL1 expression. A representative image showing PDL1 expression in RCC is shown in Figure 1. The other 9 samples had very low expression of PDL1 and were taken as negative for PDL1 expression; 10 tumour samples did not show any positive staining for PDL1.
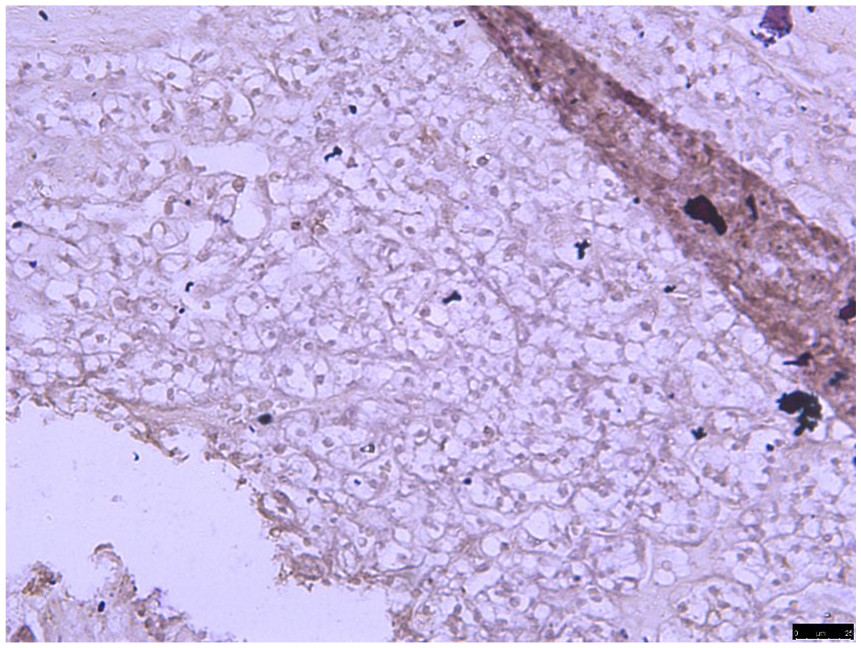
Programmed death ligand-1 (PDL1) expression seen in renal tumour cells in 20× magnification.
PDL1 was positive in 4 out of 17 (23.5%) cases of stage I tumours, 3 out of 8 (37.5%) cases of stage II, and 4 out of 5 (80%) cases of stage III. PDL1 was positive in 1 out of 16 (6.2%) cases of grade 1 tumours, 1 out of 3 (33.3%) grade 2 tumours, and 9 out of 11 (81.8%) grade 3 tumours, as shown in Figure 2.

Bar diagram showing association of programmed death ligand-1 (PDL1) with stage and grade.
The study shows that PDL1 positivity was associated with higher stage and grade at presentation; the association was statistically significant (p < 0.05).
In the study, seven out of nine (77.7%) patients who had recurrence in the 2-year follow up period had positive PDL1 expression (statistically significant, p < 0.05) as shown in Figure 3.

Bar diagram showing association of programmed death ligand-1 (PDL1) with recurrence.
Three out of five mortalities were associated with PDL1 expression but the association was not statistically significant.
Discussion
RCC has good prognosis in early stages of the disease, but the prognosis of advanced disease is dismal. 7
Stage alone has been found to be a reliable prognostic marker. However, it is ever-evolving, and multiple discrepancies have been found with stage-related prognosis. The need for new prognostication systems and markers in the past has been clear, and consequently new markers and nomograms have been developed. 3
We now have an abundance of evidence for the immunogenic nature of RCC. The most dramatic presentation of the immunogenic phenomenon is complete spontaneous regression of tumour, which has an incidence of around 0.4–4%. 8 Needless to say, this has attracted more research into the immunological basis of RCC. Findings of CA-IX as a diagnostic and prognostic marker of clear cell carcinoma is a notable example. 9
Cytotoxic T-lymphocyte antigen-4 (CTLA-4) expression on activated T cells has been shown to impair the antitumour response of T cells. On the basis of this, iplimumab, a CTLA-4 antibody, has been used in the clinical setting; however, the good antitumour response comes at a cost of intolerable toxicity at times. 10
PDL1, when bound to PD1, leads to downregulation of activated T cells. It has been shown that PDL1 expression is associated with aggressive disease in a variety of malignancies. 11 PDL1 expression in RCC has been shown to be associated with poor prognosis, aggressive disease and increased cancer-specific mortality. 12
In our study, expression of PDL1 in tumour cells was associated with higher stage and grade at presentation and with higher incidence of recurrence, all of which qualifies it as a valid poor prognostic marker. It was also associated with increased cancer-specific mortality but the association was not statistically significant, probably due to small sample size and short duration of follow up.
Similar findings have been noted in other studies. A study by Thompson and colleagues reported that elevated PDL1 expression in RCC tumours of the kidney is significantly associated with aggressive tumours and enhanced risk of RCC-specific death (threefold increased risk of RCC-specific death). 12
In another study by Thompson, Gillett and colleagues, patients with high expression of PDL1 on primary tumour cells and lymphocytes were significantly more likely to die of RCC compared with patients with low PDL1 expression (risk ratio (RR) = 4.17; 95% confidence interval (95% CI), 1.97– 8.84; p = 0.001). 13
A similar study by Thompson and Kuntz showed that the 5-year cancer-specific survival rates were 41.9% and 82.9% for patients with and without tumour PDL1, respectively. 14
With an understanding of the PDL1 axis in evasion of cancer cells from the immune system has come effort into development of targeted therapy against PDL1.
Pembrolizumab, a humanized monoclonal IgG4 antibody against PD1 inhibitor, was approved in 2014 for the treatment of melanoma. 15 Nivolumab, which has a similar action, was also approved in the same year for melanoma.
For RCC, Nivolumab in combination with Iplimumab has now achieved the status of a first-line therapy for treatment of stage IV and relapse. 16
In urothelial cancer, apart from Pembrolizumab and Nivolumab, three other PDL1 inhibitors including Durvalumab, Atezolizumab and Avelumab, have been approved.
PDL1 inhibitors are now also used in nonsquamous cell cancer of lung, head and neck cancers, gastric cancer, colorectal cancer and merkel cell carcinoma. 15
Conclusion
PDL1 is a novel prognostic marker for RCC that is associated with increased chances of cancer-specific recurrence and increased cancer-specific mortality as evident by the current studies. It is associated with higher stage and higher grade at initial presentation and represents more aggressive tumours. Its role as an independent prognostic marker is under trial and clearer results are expected in future.
As more and more research is being directed towards finding a reliable drug that specifically targets the PDL1 receptor, its use will not only prognosticate a patient but also will guide us towards expected efficacy of this drug in a particular patient.
A multicentric study with a larger patient pool will reinforce the role of PDL1 as a prognostic marker that may become the torch-bearer in the future management of RCC.
Footnotes
Acknowledgements
Kaustav Ghosh has helped in performing immunohistochemistry in the lab.
Funding
The author(s) received no financial support for the research, authorship, and publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.