
Abstract
Background:
Chronic prostatitis/chronic pelvic pain syndrome (IIIB CP/CPPS) is a condition of unclear aetiology. Many approaches have been used without satisfactory results. The aim of this study is to evaluate the efficacy of once-daily 5 mg tadalafil in pain control and improving quality of life in patients affected by CP/CPPS.
Methods:
Twenty patients affected by chronic prostatitis according EAU (European Association of Urology) guidelines were evaluated for once-daily 5 mg tadalafil; 14 patients were eligible for the study. The validated Italian version of the NIH Chronic Prostatitis Symptom Index (NIH-CPSI) and the International Prostatic Symptom Score (IPSS) questionnaires were submitted to all the patients. Every patient underwent uroflowmetry and ultrasound prostatic volume at the beginning and at the end of the study.
Results:
All 14 patients eligible for the study reported an improvement of symptoms during therapy: statistically significant differences were reported in terms of NIH-CPSI (p < 0.000002) and IPSS (p < 0.0001) during follow-up evaluations. No statistically significant improvement of uroflowmetry parameters was reported during the treatment.
Conclusions:
In our study the daily use of 5 mg tadalafil improves symptoms and quality of life in patients affected by CP/CPPS after 4 weeks of therapy. A larger population of patients is needed to confirm the efficacy of this therapy in CP/CPPS.
Introduction
Chronic prostatitis/chronic pelvic pain syndrome (IIIB CP/CPPS) is a chronic condition characterized by abdominal, pelvic and perineal pain frequently associated with obstructive and/or irritating low urinary tract symptoms. It is also characterized by the documented absence of urinary tract infection. 1 It represents a relatively common condition affecting about 8% of men aged 50 years and under. 2 Its aetiology is nowadays unclear and the therapeutic approach is still a matter of debate. Due to the strong impact on patients’ quality of life, many monotherapies have been proposed in the last decades (antibiotics, alpha-blockers, phytotherapeutics, anti-inflammatories); according to the literature, combinations of these therapies appear to achieve the greatest improvement. 3 A clinical phenotype system (UPOINT) is used to classify patients with CPPS and to guide therapy; a multimodal approach seems to be the best approach for these patients. 4 Grimsley and colleagues found that patients with erectile dysfunction treated with phosphodiesterase 5 inhibitors (PDE5) reported a concomitant improvement in their prostatitis symptoms; their paper advanced the hypothesis that the relaxation of prostatic duct smooth muscles, increasing wash-out of prostatic reflux products, could significantly reduce prostatic inflammation. 5
The aim of this study is to evaluate the efficacy of once-daily 5 mg tadalafil therapy in reducing pain and improving quality of life in patients affected by CP/CPPS.
Materials and methods
We evaluated all consecutive patients affected by CP/CPPS treated as outpatients between January and June 2016. All the patients included in the study gave their informed consent to participate.
Inclusion criteria were the presence of CP/CPPS symptoms for at least 3 months and negative Meares–Stamey test. Patients under 18 years old or over 50 years old with urinary infections or other urological diseases were excluded. All patients treated with antimicrobial drugs during the previous 3 months were excluded. A wash-out period of at least 2 weeks was requested in patients who underwent therapies with alpha-blockers, anti-inflammatory or phytotherapeutic drugs. All eligible patients during the first evaluation (V1) were administered the validated Italian version of the NIH Chronic Prostatitis Symptom Index (NIH-CPSI) and the International Prostatic Symptom Score (IPSS). Uroflowmetry and ultrasound prostatic volume were also performed. Follow-up visits were performed every 4 weeks (V2, V3, V4); every visit included NIH-CPSI and IPSS questionnaires. The uroflowmetry parameters were registered only at 12 weeks (V4). Only patients that completed the 12 weeks of treatment were considered for the study. Therefore, in addition to the descriptive statistic results (mean, standard deviation, range) one-way analysis of variance (ANOVA) and Student’s t test were used to evaluate the variables NIH-CPSI, IPSS and uroflowmetry. Statistical significance was considered if p value was <0.05.
Results
From a population of 20 patients with IIIB CP/CPPS symptoms, 5 patients were excluded for a positive 4 glasses Meares–Stamey test. Another patient had to stop taking the once-daily tadalafil therapy due to muscular pain during the first week of treatment. Fourteen patients were considered eligible for the study. Table 1 describes the population characteristics and the results of the first evaluation (V1). No adverse events were registered during the treatment. All patients reported an improvement in symptoms during the therapy: statistically significant differences were reported between the follow-up visits in terms of NIH-CPSI (p < 0.000002) and IPSS (p < 0.0001). The NIH-CPSI and IPSS results at 4, 8 and 12 weeks are reported in Tables 2 and 3 respectively; Figures 1 and 2 describe the trend of parameters during the follow-up period. No statistically significant alterations of uroflowmetry were reported during the treatment (Table 4, Figure 3).
Patient’s characteristics at enrolment (n = 14).
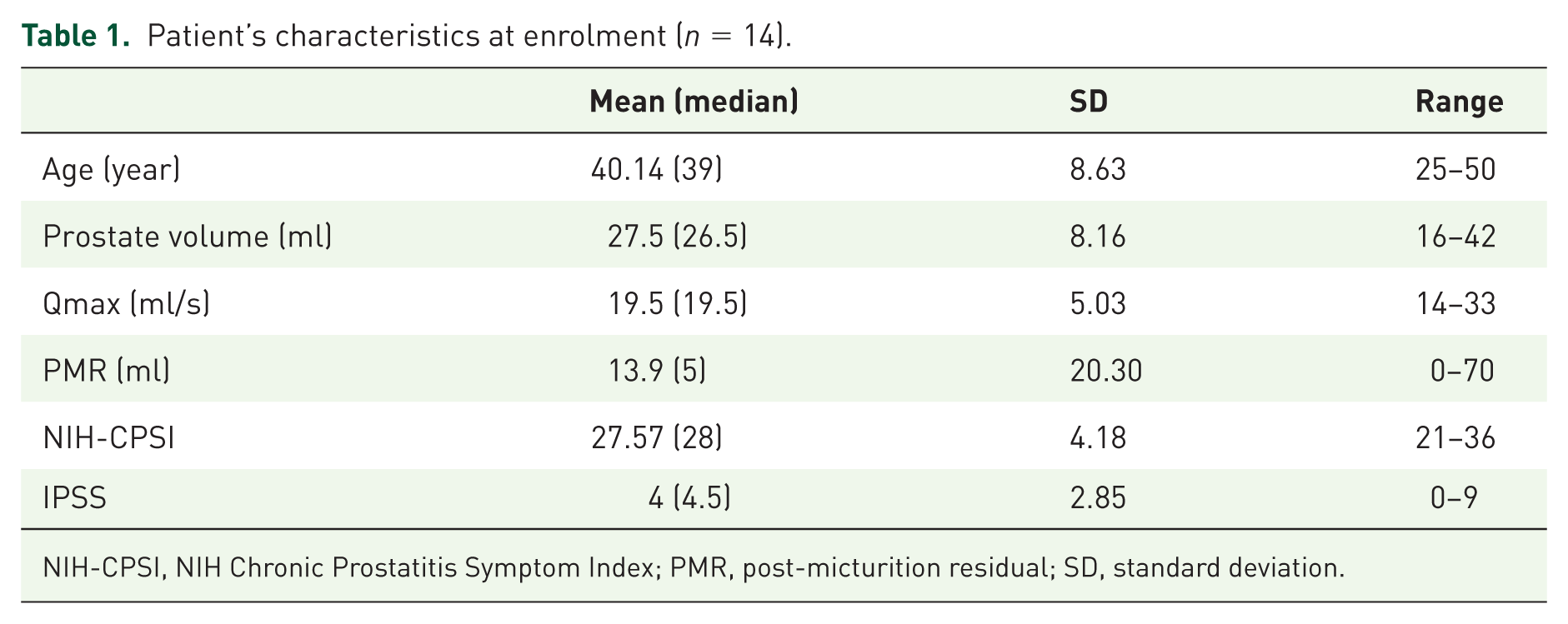
NIH-CPSI, NIH Chronic Prostatitis Symptom Index; PMR, post-micturition residual; SD, standard deviation.
NIH-CPSI during oral treatment with 5 mg daily tadalafil.

NIH-CPSI, NIH Chronic Prostatitis Symptom Index; SD, standard deviation.
ANOVA one-way test.
IPSS during oral treatment with 5 mg daily tadalafil.

IPSS, International Prostatic Symptom Score; SD, standard deviation.
ANOVA one-way test.

Symptoms progression.

Uroflowmetry parameters.
Qmax (ml/s) and post-micturition residual (PMR) after 12 weeks of oral treatment with 5 mg daily tadalafil.

Student’s t test.

International Prostatic Symptom Score.
Discussion
CP/CPPS is characterized by pelvic or perineal pain without evidence of urinary tract infection. Pain is described as arising from several area, including the perineum, rectum, prostate, penis, testicles and abdomen. It is frequently associated with urinary urgency, frequency, hesitancy and weak stream and often with painful ejaculation. 6 We evaluated the effects of once-daily 5 mg tadalafil for pain relief pain and to improve quality of life in patients affected by CP/CPPS. PDE5 inhibitors such as tadalafil work by blocking PDE5-mediated hydrolysis of cyclic GMP, leading to increased intracellular GMP levels. Cyclic GMP is a downstream mediator of nitric oxide (NO), which induces smooth muscle relaxation. Nitric oxide synthase, required for NO formation, has been localized biochemically and immunohistochemically in the transitional and peripheral zone of the prostate, 7 specifically in the nerve fibres and ganglia located in the prostatic smooth muscles. 8 PDE5, the target of PDE5 inhibitors, has been localized in the transitional zone. 9 Uckert and colleagues showed how PDE5 inhibitors reverse tension in prostatic smooth muscles, 10 suggesting that both NO and PDE5 mediate smooth muscle relaxation. Nevertheless, these studies did not explain how this muscular relaxation could improve prostatitis symptoms. Kirby and colleagues show a retrograde flow of urine into the prostatic ducts of transitional and peripheral zones in patients affected by prostatitis. 11 This study suggested that urinary reflux was the primum movens for both bacterial and abacterial prostatitis. In a recent study, Okamoto and colleagues investigated the effect of tadalafil on pelvic pain and prostatic inflammation in a rat model inducing experimental autoimmune prostatitis (EAP) in the animals. 12 Rats were treated with tadalafil 2 mg/kg or with the EAP vehicle only. The authors showed how the tactile allodynia was reduced after treatment with tadalafil. They also described a reduction in the severity of inflammatory lesions in prostatic tissues after the treatment; this suggests a role played by tadalafil in reducing inflammation and pain.
We hypothesized that the good results in terms of pain reduction and improvement in the quality of life were due to smooth muscle relaxation in prostatic ducts. This could guarantee a greater wash-out of oxidant elements from prostatic tissue, reducing irritant urinary elements and consequent prostatic inflammation.
This study has some limitations: the small number of enrolled patients and the lack of a control group. However, it represents the first paper to confirm the efficacy of 5 mg daily tadalafil in CP/CPPS. Certainly, controlled randomized clinical trials are need to confirm the results obtained in our study.
Conclusion
Though many drugs have been proposed for IIIB CP/CPPS, no effective treatment has been described. In our experience, a daily intake of 5 mg tadalafil guarantees a significant reduction in pain and improvement in quality of life for patients. Although only a small number of patients were enrolled in this study, our results are encouraging and we believe that this therapy should be given consideration when planning a multimodal approach. Certainly further studies with larger populations should be encouraged to achieve definitive results.
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.