
Abstract
Lower urinary tract dysfunction (LUTD) is common and causes a spectrum of morbidity and decreased quality of life (QoL) for patients. LUTD can range from urinary retention to urge incontinence, and includes a variety of syndromes, with the most common and widely recognized being overactive bladder (OAB). The classic treatments of LUTD and OAB comprise different strategies including behavioral therapies, medications and minimally invasive or invasive surgical procedures. Generally, once patients have tried behavioral modifications and oral medical therapy, and have not experienced adequate relief of their symptoms, the next step is to consider minimally invasive therapies. In the last two decades since FDA approval, sacral nerve stimulation (SNS) has become an accepted intervention, with increasing use and evidence of effectiveness for LUTD, specifically OAB and non-obstructive urinary retention. SNS has shown both objective and subjective improvement in voiding symptoms in several randomized controlled trials (RCTs) when compared to sham or standard medical therapy. The main limitations for more extensive use include relatively high cost, implantation of a device and possibly reoperation secondary to adverse events (AE). Percutaneous tibial nerve stimulation (PTNS) is a less invasive, less direct and less expensive method for neuromodulation, which has also shown effectiveness in several randomized and non-randomized trials, including comparable improvement rates to anticholinergics in OAB management. However, the efficacy of PTNS is only maintained for a short period after the stimulation is delivered. This technique has a much lower rate of AE compared to SNS, but with the inconvenience of weekly visits for stimulation, although implantable devices are on the horizon. In this article we review the mechanism of action, indications, effectiveness and complications related to SNS and PTNS therapy for LUTD.
Keywords
Introduction
Although treatment with electrical impulses has been attempted for over a thousand years, the modern use of electricity for treatment of urinary symptoms started in the early 1960s. In 1963, Caldwell performed one of the first clinical studies of electric stimulation to control urinary symptoms. Years later, Moore replicated the intervention, applying electrical currents in female patients with stress urinary incontinence and showing improvements in 10 out of 18 patients. 1 Then, in 1989, Tanagho and colleagues reported a study testing electrical modulation through an implanted electrode on the ventral components of S3 and S4 in patients with neuropathic voiding disorders. They reported complete success in decreasing symptoms in 42% of their patients, and partial success in 52% of them. 2 These positive results and several other reports led to multicenter clinical trials sponsored by Medtronic Inc. (MDT-103) and final FDA approval of sacral nerve stimulation (SNS) (InterStim™, Medtronic Inc., MN, USA) in 1997 for the treatment of urinary urge incontinence and in 1999 for urinary urgency/frequency and urinary retention.3–5 The same device also received the CE mark in the European Community in 1994 for the management of chronic intractable disorders of the pelvis and lower urinary or intestinal tract, and was later approved for the same indications in Australia and Canada. For percutaneous tibial nerve stimulation (PTNS), McGuire reported in 1983 the use of percutaneous electrical stimulation through acupuncture on the tibial nerve, producing inhibition of detrusor activity and improving voiding symptoms. 6 Years later, Stoller at the University of California, San Francisco, created a device to apply electrical stimulation through an electrode located near the medial malleolus. 7 Subsequent clinical trials led to PTNS FDA approval (the Urgent® PC Neuromodulation System, Cogentix Medical Inc., MN, USA) in 2005 for treating urinary urgency/frequency and urge incontinence. This device received the CE mark during the same year for similar indications and an additional indication for fecal incontinence. More recently, Medtronic Inc. developed the NURO™ system and received approval for marketing.
Overactive bladder (OAB) is defined by the International Continence Society as ‘urinary urgency, usually accompanied by frequency and nocturia, with or without urgency urinary incontinence, in the absence of urinary tract infection or other obvious pathology’. 8 Guidelines for initial management of OAB include behavioral therapy and oral medications with antimuscarinics or B3 adrenoreceptor agonists. However, it is not uncommon for a subset of patients to not have significant improvement in symptoms and for another subset to have bothersome side effects from medications. 9 In this refractory set of patients, neuromodulation represents a minimally invasive and reversible alternative with relatively few side effects. 10 While SNS and PTNS are considered third-line treatments in the American Urological Association/Society of Urodynamics, Female Pelvic Medicine and Urologic reconstruction guidelines update with a grade C recommendation and careful patient selection, 11 the International Consortium of Incontinence assigns neuromodulation as grade A for the treatment of urge incontinence and grade B for idiopathic detrusor overactivity. 12 Furthermore, the European Association of Urology guidelines recommend SNS as grade A and PTNS as grade B for patients with urgency urinary incontinence refractory to medical therapy. 13
Principles and mechanism of action
The exact mechanism of how neuromodulation works remains unclear. It is hypothesized that the low-amplitude stimulation that is delivered has effects on spinal afferents, preganglionic sympathetic and parasympathetic efferents. The S3 nerve root is especially relevant as it contains sensory fibers from the pelvic floor and parasympathetic fibers effecting the detrusor. 14 The connections and synapses travel to the CNS through spinal descending and ascending pathways reaching the brain stem and cerebral centers for bladder control, including the pontine micturition centers, with the final effect in modulating reflex pathways.15,16 In OAB, for example, previous reports have shown an augmentation of somatic inhibitory afferences. 10
SNS directly stimulates these afferent and efferent pathways through the S3 root, while PTNS indirectly stimulates similar areas through direct stimulation of the posterior tibial nerve, which is a mixed nerve containing L4–S3 fibers. 14
Patient selection, trial periods and surgical techniques
Appropriate patient selection is extremely important and a trial period before definitive placement of an implantable pulse generator (IPG) is highly recommended or required by most authorities and insurances. A trial period is the best way to determine how a patient perceives the stimulation and to see both subjective and objective improvement prior to placement of a high-cost IPG. 17 The percutaneous nerve evaluation (PNE) or trial stimulation is performed in the office and consists of insulated wire placement in the S3 and/or S4 foramen, generally under local anesthesia with the wire or wires taped and attached to an external stimulator. A successful or positive trial is defined as >50% improvement in voiding diary parameters and patient tolerance of the stimulation for at least 3 days. After appropriate counseling, the lead and IPG are then placed in an operating room (OR) setting, generally under monitored anesthesia care (MAC) on an outpatient basis. Alternatively, many surgeons prefer a staged approach in which the permanent quadripolar tined lead is implanted in the OR under sedation, and if the trial is successful, a second-stage OR procedure is done for lead tunneling and placement of the IPG. If the trial is unsuccessful, the lead can be removed under local anesthesia or under sedation. Longer trial periods up to 2 weeks can be carried out more easily if the tined quadripolar lead is implanted in the first phase as it has a much lower probability of lead migration. Although longer trial periods may decrease the rate of false-negatives, they may lead to higher rates of infection; the Medtronic product brochure specifies trial periods of no longer than 2 weeks with the tined permanent quadripolar lead. 18 Amend and colleagues evaluated 21 patients with the PNE/trial stimulation approach who had trial periods >1 month with a mean evaluation period of 52.3 days. The group found that 76% of these patients underwent definitive implantation with a success rate of 94% and no infections, infection-related explantations or wound-healing disorders during a mean follow up of 33.9 months. 19 Similarly, Kessler and colleagues found a positive testing in 73% of patients who had trial periods >14 days with temporary leads. Migration occurred in only one patient and the group did not report infection episodes. 20 Everaert and colleagues randomized 42 patients to PNE/stimulation and implant or two-stage implant, with higher rates of failed therapy in the PNE/stimulation group but lower associated costs. 21 In a separate review in patients with interstitial cystitis, the two-stage test approach consequently led to superior implantation rates compared with the more traditional PNE/stimulation group (94% versus 52%). 22 Faris and colleagues recently reported a success rate of 82% for PNE and 89% for a staged approach with higher trial success for females versus males and for urge incontinence versus urgency/frequency. These investigators found that elderly did as well as younger patients. 23
The most common technique for SNS is started with percutaneous access of the S3 foramen using landmarks such as the sacral notches and fluoroscopy. An insulated needle is first placed in the foramen and electrical stimulation is gently applied. Ideally, both sensory and motor responses are achieved. The sensory response is a pulling or vibration sensation in the vaginal and rectal areas in women and in the genital and rectal areas in men, while the motor response is a bellows like movement of the levator musculature and dorsiflexion of the big toe. If there is significant movement of all the toes at S3 and appropriate sensation is obtained at S4 with a good levator response, S4 placement should be considered. The IPG is placed in the lateral upper buttock area 4–6 cm below the posterior superior iliac crest. The lead is tunneled to the IPG with a tunneling device and connected with a screwdriver provided in the kit. Broad-spectrum antibiotics should be given prior, and appropriate precautions observed as for any prosthetic case.
PTNS does not require a strict trial period as the device is not implanted. This procedure is performed using a 34-gauge needle electrode that is inserted approximately 5 cm cephalad to the medial malleolus and slightly posterior to the tibia. The needle is inserted at a 60° angle and a surface electrode is placed on the calcaneus of the ipsilateral foot. The electrode and needle are connected to the stimulator, and after proper motor and sensory response confirmation, appropriate stimulation is carried out. The patient usually undergoes stimulation for 30 min on a weekly basis.
Effectiveness and adverse events of SNS
Table 1 presents the efficacy and adverse events (AE) of SNS in prospective trials.
Efficacy and AE of SNS in prospective trials.
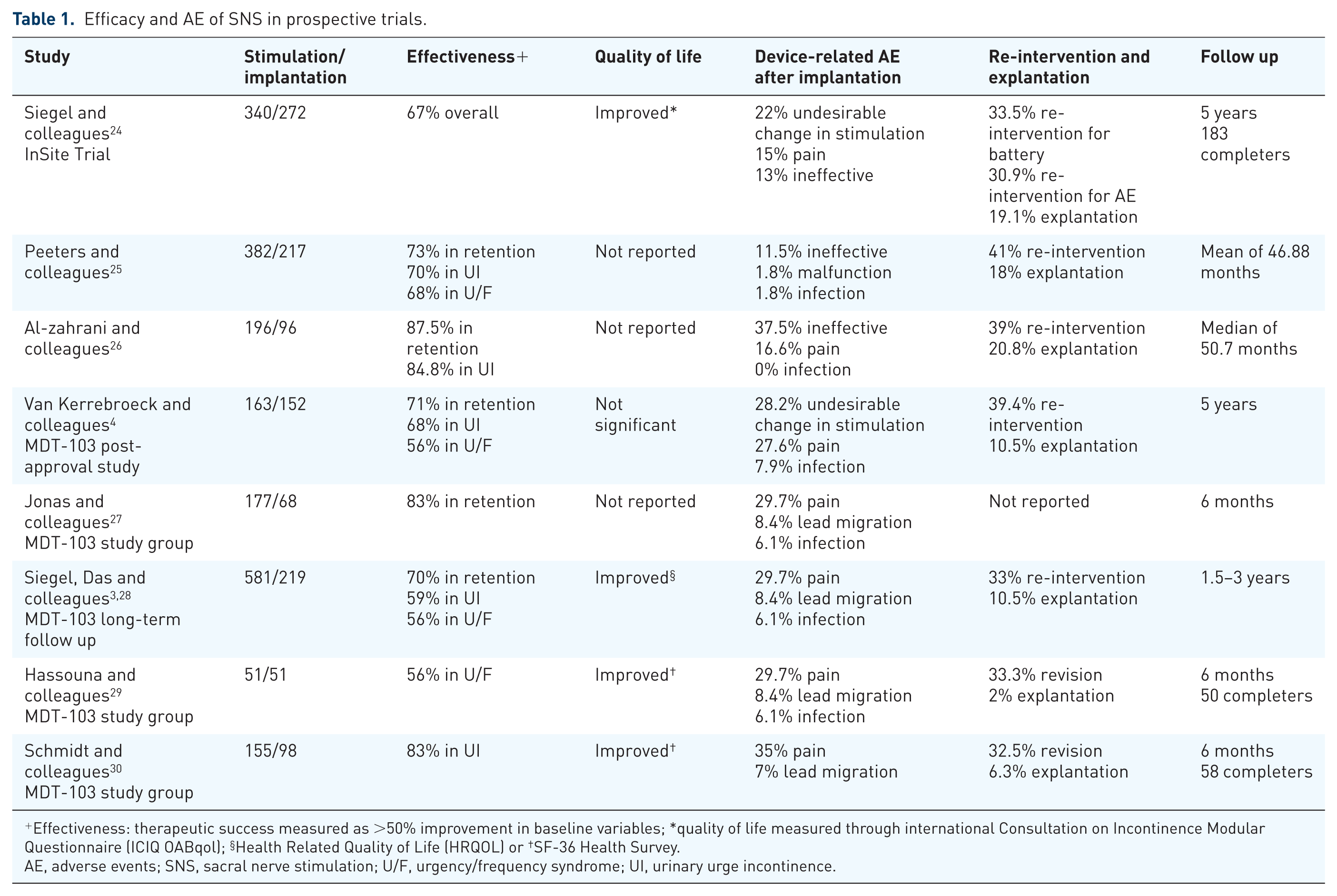
Effectiveness: therapeutic success measured as >50% improvement in baseline variables; *quality of life measured through international Consultation on Incontinence Modular Questionnaire (ICIQ OABqol); §Health Related Quality of Life (HRQOL) or †SF-36 Health Survey.
AE, adverse events; SNS, sacral nerve stimulation; U/F, urgency/frequency syndrome; UI, urinary urge incontinence.
Efficacy and AE of SNS and PTNS in reviews and RCTs
SNS
A Cochrane review in 2012 comparing anticholinergics versus non-drug therapies reported a tendency for higher subjective improvement rates in the electrical stimulation group, with a statistically significant difference only for the PTNS group. 31 For SNS only, a systematic review performed by Mirbagheri and colleagues found ‘perfect’ continence in 13–88% of patients. 32 This is consistent with another systematic review of 4 RCTs and 30 case series in urge incontinence in which 80% of the patients achieved continence or >50% improvement in their main incontinence symptoms after SNS. The reoperation rate for this particular review was 33% and explantation rate was 9%. Common reported side effects were pain at the implant or lead site in 25%, lead migration in 16%, replacement and repositioning of the implanted pulse generator in 15%, wound problems in 7% and infections in 5%. 33 There have been multiple reported RCTs with different designs. However, the main limitation for RCTs in neuromodulation is the absence of a proper placebo control, which can bias the results. The Rosetta trial was a multicenter open-label randomized trial comparing SNS versus botulinum toxin A (BotA) 200 units in refractory urgency incontinence after failed behavioral/medical therapy. This study reported greater improvement in decreasing symptom bother, and higher treatment satisfaction in the BotA group compared to SNS. However, BotA was also associated with higher incidence of urinary tract infections and a higher need for self-catheterization. Within the SNS group, the revision and removal rate was quite low at 3% of the patients. 34 A prospective, randomized, multicenter trial evaluating the 6-month success of SNS versus standard medical therapy in patients with mild OAB found significant improvement in quality of life (QoL) in the SNS group only and improvement rates in urinary symptoms of 86% compared to 44% for the medical therapy group. The AE rate was similar in both groups. 35 Finally, Scheepens and colleagues studied bilateral versus unilateral stimulation in a crossover trial of patients that had bilateral SNS implantation. At the conclusion of the study, no statistically significant improvement was achieved between unilateral versus bilateral stimulation. 36
PTNS
The effectiveness of PTNS has been compared against sham procedures, placebo or medical therapy. Finazzi-Agro and colleagues randomized 35 women with detrusor overactivity and urge incontinence unresponsive to medical therapy with antimuscarinics to PTNS or placebo. In the latter group, patients received stimulation through a needle placed in the medial part of the gastrocnemius muscle with the same frequency as the PTNS group. At the end of the study, 71% in the intervention group were considered responders with statistically significant improvement in the number of incontinence episodes, number of voids, voided volume and QoL. For the placebo group, 0% of the patients responded to therapy. 37 Similarly, in the SUmiT trial, 220 OAB patients were randomized to receive PTNS or sham in which they felt the needle but without any stimulation. The study reported statistically significant improvement in bladder symptoms, improvement in voiding diary parameters and no serious AEs for the PTNS group, with 54.5% of the patients reporting moderately or markedly improved responses compared to only 20.9% in the sham group. 38 In the ORBIT trial, PTNS intervention was compared to tolterodine 4 mg extended release, showing higher rates of subjective cure or improvement in the neurostimulation group (79.5% versus 54.8%) with similar rates of objective improvement and no serious AEs or device malfunctions. 39
Quality of life
One sub-study on patients from the original MDT-103 trial demonstrated notable depression and reduced QoL based on the SFA-36 questionnaire at baseline, with significant improvements in health-related QoL and depression scores after SNS. The results were maintained for 6 months. 28 Other authors have reported similar findings.40,41
Costs
Martinson and colleagues built an economic model comparing PTNS versus SNS in patients who remain on therapy for 2 years. The model reported lower costs for PTNS, with a difference of nearly 10,000 USD between them after a successful trial period. 42 In a Canadian study, a Markov model was developed over a 10-year horizon and deemed SNS the most cost-effective therapy to treat OAB when compared to BotA and medical therapy. 43 In another cost-effectiveness study, SNS was found to be cost-effective after 4 years of treatment when compared to BotA. These findings were no longer applicable if BotA injection were performed under local anesthesia or if bilateral SNS testing were performed. 44
Limitations and future prospects
MRI
The need for future MRI testing is now considered a partial contraindication for SNS placement. Recently, a study by Elkeleni and Hassouna in eight patients with implanted SNS before and after 1.5 Tesla MRI showed no change in perception of the stimulation, no device malfunction and no change in bladder function. 45 Similarly, Chermansky and colleagues reported an IPG malfunction in one patient that underwent 1.5 Tesla MRI with the IPG on. In contrast, eight patients that had the same test with the device off did not have any device malfunction after MRI. 46 Following these reports, Medtronic has developed guidelines for the conditional use of 1.5 Tesla MRI for head examination only and received FDA approval for 1.5 tesla MRI head scans in patients with the InterStimTM II model 3058. 47 New devices are already available for spinal cord stimulation that are safer for MRI.
Rechargeable IPG
Since battery life remains a significant limitation and also increases costs, a rechargeable IPG would be a welcome addition. Again, the technology for externally rechargeable devices that may need to be charged every 2–3 weeks, but which may not require replacement for up to 10 years, already exists and it is only a matter of time before it becomes available.
Implantable tibial nerve stimulator
A few trials have reported outcomes of implantable tibial nerve stimulators. The Urgent SQ™, developed by Uroplasty, is surgically implanted near the posterior tibial nerve and activated by an external stimulator. Preliminary open-label studies in a limited number of refractory OAB patients have shown relatively good effectiveness, minor AEs and no significant problems with device migration.48,49 Another battery-free device developed in Israel showed significant decreases in episodes of urgency, frequency and incontinence after 3 months, but reported some pain-related events in three patients and one explantation secondary to signs of infection. 50 An implantable device for tibial nerve stimulation clearly decreases the need for frequent office visits, and future studies are needed to better understand the long-term effectiveness and complications of these devices.
Other uses and other devices
While SNS has also been evaluated for neurogenic voiding dysfunction in disorders like Parkinson’s disease, stroke or multiple sclerosis, and some trials have shown similar efficacy and safety profile compared to non-neurogenic patients, these have been quite limited in scope and quality.51,52 Furthermore, the actual FDA approval in the USA is for non-neurogenic use only, as the original MDT-103 study specifically excluded all neurogenic patients. 3 The SNS has also received FDA approval for the treatment of fecal incontinence, but that is a separate topic. Other limited trials have been reported, showing effectiveness in treating interstitial cystitis and chronic pelvic pain syndromes. 53 Further research and rigorous studies are needed to better understand the effectiveness and safety of SNS and PTNS in neurogenic voiding dysfunction and pelvic disorders. Finally, there are descriptions of other non-implantable methods for external neuromodulation in the treatment of urge incontinence and OAB. Pelvic floor electrical stimulation using vaginal, anal and surface electrodes; magnetic stimulation delivered through a chair device, and inferential therapies are under-researched and less popular, with mixed results. 54
Conclusion
Both SNS and PTNS are useful modalities in the treatment of OAB, and SNS is also useful in the treatment of non-obstructive retention. PTNS is very minimally invasive but requires weekly visits and may lose therapeutic effect once treatment is completed although implantable devices are on the horizon. SNS does require a minimally invasive surgical procedure to place the IPG once a PNE/test stimulation or stage 1 lead placement shows adequate subjective and objective symptom improvement. For patients with refractory OAB, these modalities represent acceptable treatment options if behavioral therapies are unsuccessful and pharmaceutical management is suboptimal or leads to intolerable side effects. The vast majority of data support the use of SNS for patients with idiopathic OAB and non-obstructive retention, although there are limited reports for the use of this entity in neurogenic OAB and entities such as interstitial cystitis/chronic pelvic pain syndrome. Finally, revisions of SNS due to lead migration, pain and battery depletion (expected after 2–4 years) are common but well-tolerated minimally invasive procedures that are generally performed under MAC.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.