
Abstract
Urolithiasis is the most common nonobstetric complication in the gravid patient. The experience can provoke undue stress for the mother, fetus, and management team. The physiologic changes of pregnancy render the physical exam and imaging studies less reliable than in the typical patient. Diagnosis is further complicated by the need for careful selection of imaging modality in order to maximize diagnostic utility and minimize obstetric risk to the mother and ionizing radiation exposure to the fetus. Ultrasound remains the first-line diagnostic imaging modality in this group, but other options are available if results are inconclusive. A trial of conservative management is uniformly recommended. In patients who fail spontaneous stone passage, treatment may be temporizing or definitive. While temporizing treatments have classically been deemed the gold standard, ureteroscopic stone removal is now acknowledged as a safe and highly effective definitive treatment approach. Ultimately, a multidisciplinary, team-based approach involving the patient, her obstetrician, urologist, radiologist, and anesthesiologist is needed to devise a maximally beneficial management plan.
Introduction
Management of urolithiasis in the pregnant patient requires clinical finesse and thoughtful analysis of the risks and benefits to both the mother and child with each decision. During her pregnancy, the mother undergoes physiologic changes which introduce additional complexities in stone management; similarly, the fetus is especially vulnerable to harm secondary to the disease process, diagnostic measures, and standard therapies. Given that the prevalence of kidney stones has been reported to be as high as 1:200 pregnancies, 1 it is critical that urologists be informed of the best treatment practices in order to provide exceptional care to both the mother and her child.
Diagnosis of urolithiasis in the gravid patient with suspected renal colic is complex. Maternal physiologic changes, such as hydronephrosis, make it difficult for the urologist to rely on traditional clinical signs and symptoms of urolithiasis for diagnosis.2–4 Furthermore, utilization of diagnostic imaging can only be done after careful consideration of risks and benefits; the ideal technique maximizes diagnostic yield while minimizing harm to the fetus and the mother by contrast methods and ionizing radiation. Accurate diagnosis is paramount as it guides appropriate management. 5
Many complexities also underlie the difficulty of treatment of urolithiasis in the pregnant patient. Optimal management requires careful consideration of benefits and risks to both mother and fetus with each decision. All methods of active management, with the exception of extracorporeal shock wave lithotripsy (SWL) and percutaneous nephrolithotomy (PCNL), are appropriate options for the gravid patient.6–9 Selection of a management plan for the pregnant patient must consider the need for anesthesia or contrast as well as radiation exposure, pain management, and possibility of obstetric complications. Conservative treatment therefore remains an attractive option to minimize medical and surgical interventions; however, as will be discussed, its success rate is often overestimated in the pregnant population.10,11 Often times, the appropriate approach to management of urolithiasis in the gravid patient requires a multidisciplinary team approach.8,12
Stone formation in pregnancy
As noted, the prevalence of kidney stones has been reported in as many as 1:200, and may range to 1:1500 pregnancies. 1 Furthermore, renal colic secondary to urolithiasis is the leading nonobstetric cause of hospitalization in the gravid patient. 13 Although the incidence of stones has previously been shown to be equal in pregnant and nonpregnant women of childbearing age, 14 the pathophysiologic forces driving the formation of these stones is influenced and complicated by a myriad of pregnancy-related changes in the mother.
Physiologic hydronephrosis of pregnancy
The incidence of physiologic hydronephrosis is as high as 90% on the right side and 67% on the left side during pregnancy. Though this typically resolves within 4–6 weeks postpartum, its laterality throughout pregnancy has shown no association with factors such as urinary tract problems or prior pregnancies. 4 Given this unpredictable nature, it may be difficult for a clinician to distinguish between physiologic and pathologic hydronephrosis.
The underlying pathophysiology of hydronephrosis in pregnancy is secondary to both mechanical and hormonal factors. The primary cause is ureteral obstruction secondary to compression from the gravid uterus at the pelvic brim. The anatomic relations of the ureters at the pelvic brim explain the susceptibility for development of right hydronephrosis; specifically, the right ureter crosses the iliac artery at the pelvic brim, whereas the left ureter does so more proximally and laterally, resulting in lower probability of compressing of the left ureter. 3 Other contributory mechanical factors such as the dextrorotation of the uterus and the cushioning of the left ureter by the sigmoid colon also help explain the predisposition of hydronephrosis for the right kidney.2,15
Hormonally, increased levels of progesterone during pregnancy decrease ureteral peristalsis, causing ureteral dilation above the pelvic brim.2,15 This physiologic hydronephrosis may result in stagnation of urine, potentially predisposing to stone formation 16 and complicating diagnosis, as will be subsequently discussed.
Urinary changes in pregnancy
With the increased metabolic demand of pregnancy, there is a concurrent physiologic increase of glomerular filtration rate by up to 50% throughout pregnancy. 17 Urinary excretion of sodium, calcium, and uric acid is subsequently increased. 18
Hypercalciuria in pregnancy arises partly secondary to the increased glomerular filtration rate, as well as to the placental production of 1,25-dihydroxycholecalciferol induced by fetal demand.2,19 One study of 15 healthy pregnant women taking only prenatal supplements identified hypercalciuria in all three trimesters; 7/15 (46.6%) of the women had hypercalciuria in the first trimester, 9/15 (60%) in the second trimester, and 8/15 (53.4%) in the third trimester. Additionally, 8/15 (53.4%) women had hypercalciuria in the 3-month postpartum period. Urine calcium levels in the second and third trimesters were significantly higher than those in the postpartum period; however, increased urine oxalate levels were not identified in any of the pregnant patients, except in the postpartum period. 18 In fact, hypercalciuria alone has been found to promote calcium oxalate supersaturation, thus potentially promoting calcium oxalate stone formation.20,21
Another notable change during pregnancy is the rise in urine pH. 6 Interestingly, hypercalciuria in alkaline urine favors the crystallization of calcium phosphate (rather than calcium oxalate) stones. 22 Therefore, one would expect a penchant for calcium phosphate stone formation in the pregnant woman. Indeed, although calcium oxalate calculi account for up to 65% of all stones in the general population, calcium phosphate stones predominate in pregnancy. In one study of 27 gravid patients with nephrolithiasis, calcium phosphate (hydroxyapatite) stones were far more prevalent than calcium oxalate stones during pregnancy. Stone analysis confirmed that in 74%, stone composition was predominantly calcium phosphate, whereas only 26% of cases had stones composed predominantly of calcium oxalate. 23
The rates of calcium phosphate stones in pregnant women are high even when compared with nonpregnant women of similar ages. For example, one study of over 2453 renal calculi produced during 1988–2004 reported that calcium oxalate stones comprised 42% of all studied renal calculi in women aged 10–35, whereas calcium phosphate stones comprised only 22%. 24 These findings suggest that the physiologic changes of pregnancy do in fact favor calcium phosphate stone formation.
Countering the increase in urinary promoters of stone formation during pregnancy is a concurrent rise in the excretion of crystallization inhibitors, such as citrate, magnesium, and glycosaminoglycans.1,2,18 Gestational hyperthiosulfaturia has also been proposed to reduce the risk of urolithiasis. 25 The increase in purported inhibitors has been postulated to explain why, despite physiologic hydronephrosis and an increase in urinary concentration of lithogenic factors, the overall prevalence of nephrolithiasis does not appear to increase in pregnancy. 18 Nevertheless, recent epidemiologic evidence noted an association between increasing number of pregnancies and lifetime stone prevalence, suggesting possibility of cumulative stone formation, regardless of actual stone presentation, during pregnancy. 26
Diagnosis
The correct and prompt diagnosis of urolithiasis in pregnancy is critical, as renal colic has been associated with an increased risk of preterm premature rupture of membranes and up to an 80% increase in odds of preterm delivery.27,28 As discussed previously, accurate diagnosis is muddled by the physiologic changes of pregnancy, and is limited by the need to use imaging with ionizing radiation as sparingly as possible, with careful regard to risks and benefits.
Testament to this difficulty is the fact that in a recent study of 82 pregnant women hospitalized for suspected acute renal colic, a stone was confirmed in only 29%. In this same study, the only factor predictive of urolithiasis was left hydronephrosis >10 mm. 29 The most common presenting symptom of urolithiasis in gravid patients is flank pain, reported in one study in 96.5% of 144 confirmed cases. 30 However, traditional clinical signs and symptoms of urolithiasis become less reliable for diagnosis in the pregnant woman, as flank pain and microscopic hematuria may occur as part of the normal course of pregnancy.30,31 While the physical exam undeniably remains an important part of the work up of urolithiasis in the gravid patient, adjunctive diagnostic measures are necessary to confirm the diagnosis.
Ultrasound
Renal ultrasound remains the first-line imaging modality in the gravid patient as its use protects the fetus from the risks of teratogenic radiation exposure of computed tomography (CT) or magnetic resonance imaging (MRI).1,32 It is quick, readily available, noninvasive, and cost effective. Importantly, there are no documented adverse effects on the fetus from diagnostic ultrasound studies. 33 Ultrasound is especially useful for visualizing stones calculi in the renal pelvis and ureteropelvic junction, and may also detect stones in the distal ureter when visualizing the bladder. 30 When a distal ureteral stone is identified on ultrasound, it is typically visualized as an echogenic, posteriorly shadowing focus at the distal end of a dilated ureter. 34 However, in the absence of a definitively visualized stone, differentiating between physiologic hydronephrosis of pregnancy and ureteric obstruction can be limited.2,35 Renal ultrasound has a 34% sensitivity and 86% specificity for urolithiasis, but reported sensitivities have ranged considerably, and there may be even more variability in sensitivity depending on the extent of physiologic changes in pregnancy.30,36 If renal ultrasound is ultimately inconclusive in aiding a diagnosis, the clinician may need to explore alternative diagnostic modalities.
In comparison to renal ultrasound, transvaginal ultrasound has been shown to have improved sensitivity in the identification of distal ureteral stones, as well as in the differentiation between obstruction and physiologic hydronephrosis; however, lack of availability and expertise may limit its use.1,34,37,38
Andreoui and MacMahon reported that ultrasound accuracy in predicting ureteral stones improved from 56.2% to 71.9% when the absence of a ureteric jet and an elevated renal resistive index (RI) were noted. RI was defined as the peak diastolic velocity subtracted from the peak systolic velocity, divided by the peak systolic velocity; an abnormally elevated RI was defined as ⩾0.70 and a significant ΔRI (inter-renal difference in RI) as ⩾0.08. 30 The utility of renal RI in identifying ureteral obstruction was confirmed in a study of 19 pregnant patients with unilateral symptomatic persistent hydronephrosis. 35 Shokeir and colleagues concluded that the ΔRI is a 77% sensitive and 83% specific test for diagnosis of acute unilateral ureteral obstruction in pregnant women. 39 Although there have been no documented adverse fetal effects from duplex Doppler imaging, its safety has not been proven at young fetal age.40,41
Computed tomography
With over 98% sensitivity and specificity, noncontrast CT is considered the gold standard for diagnosis of nephrolithiasis in the general population. 1 In the pregnant patient, CT has been generally avoided due to concerns about fetal radiation exposure; this is especially true during the first trimester. Nevertheless, use of diagnostic CT during pregnancy increased by 25% per year from 1997 to 2006. 42
Effects of radiation exposure can be classified as stochastic or deterministic; the latter are dose-dependent above a baseline threshold dose, whereas the former are possible at any level of radiation exposure. 43 According to the American College of Obstetricians and Gynecologists, there is no association between radiation doses of <50 mGy (<5 rad) and fetal anomalies or pregnancy loss. Potential, but unproven, subtle effects may be seen with early radiation exposure between 50 mGy and 100 mGy (5–10 rad). Spontaneous abortion risk, and risk of diminished IQ is associated with doses >100 mGy (>10 rad) at gestational age > 3 weeks. In general, however, the use of CT should not be withheld if clinically indicated, as long as the risks and benefits have been thoroughly considered.1,40,44,45
Ultra-low-dose CT is an option which reduces the radiation dose below teratogenic threshold levels. Noncontrast CT of the abdomen and pelvis delivers an estimated effective radiation dose of 8–10 mSv,45,46 though values up to 66% higher have been reported. 47 One recent systematic review of all prospective studies on adult patients undergoing various CT imaging modalities for renal colic or urolithiasis from 1995 to 2015 sought to define effective low-dose and ultra-low-dose CT radiation doses. After review of seven studies (1104 patients), they concluded that low-dose CT can be defined as <3.5 mSv, and ultra-low dose as <1.9 mSv. 48 Theoretically, this should make it safe for diagnostic use in pregnancy from the deterministic, teratogenic standpoint, although some theoretical concerns regarding stochastic effects including delayed hematologic malignancy remain.32,37 Studies have shown >96% sensitivity and specificity, and up to 99% positive predictive value of low-dose CT for diagnosis of stones in the nonpregnant population. 49 Studies of pregnant women evaluated with low-dose CT for urolithiasis have found >95% specificity and positive predictive value.12,50
Magnetic resonance imaging/urography
MRI is a useful alternative to CT in the pregnant patient. MRI utilizes nonionizing radiation, and provides similar or greater sensitivity and specificity than CT without the need for contrast. 51 Magnetic resonance urography (MRU) using T2-weighted images has been proposed to be useful for distinguishing physiologic hydronephrosis of pregnancy from obstructive hydronephrosis. 52 In one study, half-Fourier acquisition single shot turbo spin-echo (HASTE) MRU was able to distinguish physiologic hydronephrosis from obstructive lithiasis in eight of nine patients. 51 Alternatively, thin-slice, high-resolution, T2-weighted fast spin echo (FSE) sequences have been reported to be valuable in the identification of smaller stones.52,53 As such, MRU is now touted as a second-line imaging modality during pregnancy, when ultrasound results are unrevealing or inconclusive.52,53
While the positive predictive value of MRI for detection of urolithiasis in pregnancy is higher than that of ultrasound (80% versus 77%), CT remains superior in that regard (95.8%). 50 However, one study of 64 nonpregnant patients with possible obstructive stones found that although actually identifying the stone itself in only 72%, the combination of perirenal fluid and ureteric dilation on HASTE MRU combined with plain film radiography provided similar overall accuracy in clinical diagnosis compared with CT. HASTE MRU also offers the added benefit of decreased observer variability than CT in detecting secondary signs of obstruction. 54 Therefore, there may be a role for HASTE MRU in the gravid patient with acute urolithiasis when other diagnostic modalities have proved inconclusive.
According to the 2013 ACR guidelines, there have been no conclusively documented deleterious effects of MR imaging on the developing fetus. 55 Various studies of pregnancies with a history of MRI exposure in either the first or third trimester have found no evidence of increased risk to the unborn fetuses.56,57 Accordingly, pregnant patients can receive MRI at any stage of pregnancy if indicated. Though administration of contrast agents is not an absolute contraindication in pregnancy, it should be considered on a case-by-case basis only if absolutely necessary, as gadolinium-enhanced MRI has been associated with extensive adverse effects, including neonatal death. 56
Intravenous urography
Intravenous urography (IVU), also known as intravenous pyelography (IVP), uses serial plain film imaging after intravenous administration of iodinated contrast in order to dynamically visualize the collecting system. More commonly used in the past, recent consensus considers alternative imaging modalities, including ultrasound, CT, and MRI, to be superior for the diagnosis of urolithiasis.58–61 In general, the routine use of IVP has been called into question and correspondingly declined in recent years. 62 The relatively low utility of IVP is especially prominent in pregnancy when one considers the radiation dose exposure secondary to serial radiographic imaging in IVU as well as the need for intravenous contrast.
Management of stones in the pregnant patient
Guided by the judicious use of imaging studies as outlined above, several courses of management may be considered. An overview of such strategies is presented in algorithm form (Figure 1), with summary of management consideration reviewed below.
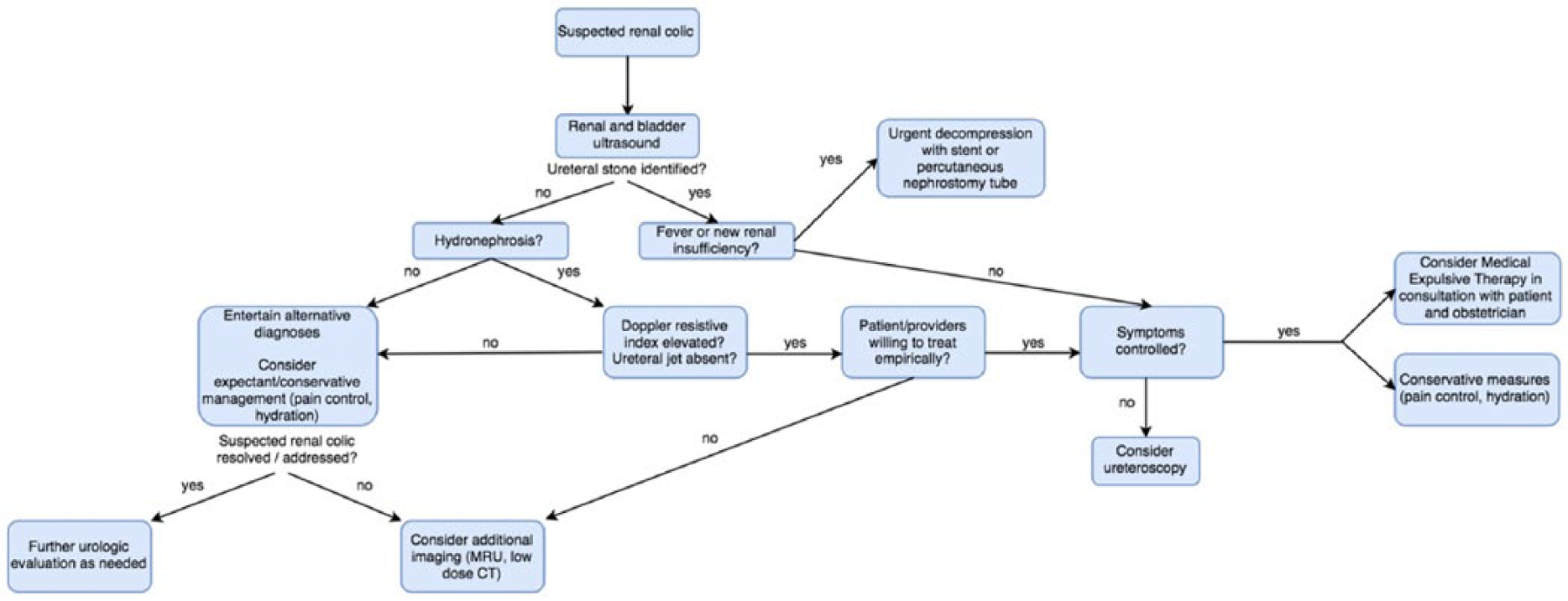
Algorithm for management of suspected renal colic in a gravid patient.
Conservative management
A majority of calculi are thought to pass spontaneously with conservative, expectant treatment of intravenous fluids and analgesia. Therefore, a trial of conservative therapy is always indicated in the gravid patient with urolithiasis.5,32 Rates of spontaneous stone passage have been reported as high as 70–80%, but this number may be overestimated in pregnancy due to misdiagnosis and poor follow up. 63 One study of 144 pregnant patients with confirmed nephrolithiasis found that 63% of stones passed spontaneously; 42.3% of renal pelvis or calyceal stones and 44.1% of distal ureteric stones passed spontaneously, whereas only 27.3% of ureteropelvic junction and proximal ureteric stones passed spontaneously. 30 While conservative management is considered a first-line therapy, it is important to recognize that it may be better-suited for stones in specific locations and more aggressive treatment is likely required if the patient does not feel adequate relief.
Conservative management remains the first-line treatment for uncomplicated cases of urolithiasis in pregnancy. The American Urological Association (AUA) guidelines endorse an initial management with conservative treatment, awaiting spontaneous stone passage in clinically fit patients. 5 Indications for conservative management include small solitary stones (<1 cm in size) in an otherwise stable patient with no signs of severe distress or infection. 1 Care should be taken to avoid nonsteroidal anti-inflammatories in these patients as they have been linked to fetal pulmonary hypertension, as well as premature closure of the ductus arteriosus if given in the third trimester. The preferred analgesic regime has been frequent, small doses of morphine.8,64,65 However, pain management strategies for stone disease continue to evolve, and in the pregnant population must also take fetal exposure into account, in addition to addressing the mother’s pain control. As per the American Urological Association (AUA)’s guidelines for the surgical management of stones, pharmacologic interventions should be coordinated with obstetric consultation. 5
Given the increased risk of premature labor and morbidity in the gravid patient with urolithiasis,6,64,65 it is critical that urologists understand when conservative management is insufficient. Indications for more aggressive treatment include pain refractory to analgesia, complete renal obstruction, and sepsis; this could occur in up to 20–30% of cases. 65
Medical expulsive therapy
When conservative management fails to control pain, or if the stone is unable to pass spontaneously, medical expulsive therapy may be considered in attempt to facilitate passage of calculi, although specific concerns have been raised.1,6 Alpha blockers and calcium channel blockers may cause relaxation of ureteric smooth muscle and facilitate the spontaneous passage of calculi. 11 However, evidence both supporting and opposing the use of medical expulsive therapy (MET) has been reported, and as of now the consensus remains inconclusive. Expulsive therapies such as tamsulosin and nifedipine are in fact used off label for treatment of stone disease, but are not US Food and Drug Administration (FDA) approved for use in pregnancy. 10 The SUSPEND trial is a multicenter, double-blind, randomized controlled trial which reported no difference in rates of spontaneous stone passage in groups of nonpregnant patients treated with tamsulosin, nifedipine, or placebo. 11 In a more recent meta-analysis of 55 randomized controlled trials of alpha blockers compared with placebo, Hollingsworth and colleagues found ‘moderate quality evidence’ that nonpregnant patients with larger stones may benefit from treatment with alpha-blockers, as they had a 57% higher overall rate of stone passage (95% confidence interval 1.17–2.27). 66 Clearly, further study is warranted.
The smooth muscle relaxation benefit provided by these therapies may prove less useful in pregnancy, as the ureters are already physiologically dilated. 10 In addition to possibly reduced efficacy, tamsulosin is classified as a category B medication by the FDA (defined as no demonstrated risk in animal reproduction studies, but lacking adequate studies in pregnant women 67 ), and reports on safety and outcomes of alpha blockers in pregnancy have been limited. A recent retrospective study of 27 patients receiving tamsulosin as MET matched 2:1 to untreated pregnant women with symptomatic urolithiasis found no significant differences in a host of perinatal outcomes, including mean gestational age, birthweights, lengths, Apgar scores, and NICU admissions. The study did identify a nonstatistically significant, but potentially concerning, increase in the incidence of sudden infant death syndrome (SIDS) in the tamsulosin cohort (p = 0.11). All possible SIDS risk factors were not assessed in their retrospective review, raising the possibility of confounding; however, this warrants further study. 68 Despite continuing conflicting evidence regarding spontaneous passage rates of stones with MET, a recent email survey study with 565 respondents found that worldwide MET usage was 97.6%, and usage in pregnancy was 44.3%. 10 Given the prevalence of off-label use and the lack of definitive evidence for or against the use of MET, further study of its use in pregnancy is clearly indicated. Until a conclusion is reached, ultimate decisions regarding medical and surgical management should be based on discussion with the patient and her obstetrician, as recommended by the AUA guidelines. 8
Temporizing options (ureteral stents, percutaneous nephrostomy drainage)
Active management options for urolithiasis can be subdivided into temporization strategies and definitive stone management. Temporization strategies include either ureteral stent placement or percutaneous nephrostomy (PCN) drainage. Historically, temporizing treatments have been considered the gold standard surgical management option for urolithiasis in pregnancy because they are less invasive and can potentially be performed under local anesthesia. These methods are highly effective in relieving obstruction, thus alleviating pain and helping to protect renal function.8,69 Reasons to consider temporary drainage include failure of conservative treatment, excessive stone burden, complex anatomy, obstetric concerns or complications, presentation very early or very late in the pregnancy, and other absolute contraindications to definitive surgical management, including active urinary tract infection.1,5,8
Ureteral stents and PCN drainage are considered equally safe and effective in pregnancy. Indwelling stents may be poorly tolerated, causing pain more severe than acute renal colic and reducing quality of life. One study of 26 women with urolithiasis found that 7 out of 15 women with stents required early induction secondary to stent intolerance. 70 Alpha blockers and antimuscarinics may be offered to nonpregnant patients to reduce stent discomfort, but their efficacy and appropriateness in the pregnant patient is unclear. 71 Furthermore, stents may be subject to bacterial colonization (increasing the risk of ascending urinary tract infection) as well as to migration and encrustation. In the pregnant patient specifically, the risk of encrustation is greater due to the altered urinary environment. If severe, this may prevent drainage and cause re-obstruction, further complicating surgical management. As such, stents require device exchange every 4–6 weeks in the gravid patient.1,6,9,64,69,72–74
PCN drainage is associated with many of the same complications as ureteral stents, including encrustation and bacterial colonization. The tubes are also subject to inadvertent dislodgement, causing more pain symptoms and the need for reintervention. While PCN tubes tout a decreased risk of ascending urinary tract infection, they have been associated with an increased risk of septic complications and pose the additional burden of an external drain to the patient; stents are therefore generally preferred.9,74
Overview of definitive stone management
Definitive stone management modalities include ureteroscopy, SWL, and PCNL. The latter two are not typically employed in the gravid patient. 1 Definitive stone management eliminates the need for recurrent procedures such as device exchange that are required with temporizing procedures. Indeed, as with any surgical intervention in the gravid patient, definitive stone management requires collaboration between several teams, including urology, obstetrics, neonatology, and anesthesia. 12
Ureteroscopic stone removal
Ureteroscopic stone removal (URS) has long been known to be safe and highly effective in pregnancy. 75 In addition to boasting high stone clearance rates, URS also offers low complication rates. A recent systematic review by Semins and colleagues identified 14 reports encompassing 108 pregnant patients who underwent URS. They reported an overall urologic complication rate of 8.3%, with no significant difference in the rates of ureteral injury or urinary tract infection complication rates when compared with outcomes in nonpregnant women. 9 A retrospective study specifically assessing postureteroscopy obstetric outcomes identified two complications out of 46 gravid patients undergoing ureteroscopic procedures at five institutions for an overall obstetric complication rate of 4.3%. 12 Despite similar complications rates, the acuity of a complication in the pregnant patient is higher than in the nonpregnant patient given the risk to the fetus, underscoring the need for a team-based approach. The ACOG guidelines recommend that any nonurgent surgeries, such as URS, be performed in the second trimester of pregnancy to minimize the risk of preterm contractions and spontaneous abortion. 76
Although typically, ureteroscopy is performed with fluoroscopic guidance, concerns regarding maternal/fetal radiation exposure have prompted development of strategies to reduce or eliminate intraoperative fluoroscopy in this population. Use of low dosed and pulsed fluoroscopy combined with lead shielding of the patient’s pelvis can reduce total radiation exposure, whereas direct, endoscopically visualized passage of the ureteroscope or ultrasound-guided ureteroscopy may allow a completely radiation-free method of ureteroscopy in the gravid patient. 77
Another consideration favoring URS is reduced cost; Wymer and colleagues created decision analytic models for a theoretical cohort of pregnant women diagnosed with symptomatic urolithiasis.
Treatment courses with serial stenting every 4 weeks were compared with URS in regard to cost and effectiveness. Ureteroscopy was ultimately found to be less costly and more effective, especially if the diagnosis of urolithiasis was made during early pregnancy. Costs analysis considered the possibility of complications related to each procedure, and effectiveness was measured as quality-adjusted life-years. 78 The AUA guidelines endorse ureteroscopic stone treatment in those failing trial of observation for ureteral stones, with alternative options of stent or nephrostomy placement recognizing the aforementioned limitations inherent in these temporizing alternatives. 8
Shock wave lithotripsy
Shock wave lithotripsy (SWL) harnesses shock wave to fragment stones. In nonpregnant patients, it is an excellent option for management of urinary stones, as it is noninvasive and efficacious.72,79 However, it is absolutely contraindicated in pregnancy due to the potential for fetal death from shock wave injury. One study of pregnant mice at different gestational stages found a direct association between number of shock waves received and fetal loss. The authors report extensive hemorrhage and necrosis in the fetuses upon histological analysis. Given the many alternative treatment options for symptomatic urolithiasis, pregnant women with stones should never be exposed to the risks associated with SWL. 7 In light of this risk, all women of child-bearing age should receive a pregnancy test prior to treatment with SWL.
Pneumatic and laser lithotripsy
Studies of safety and efficacy of pneumatic lithotripsy and laser lithotripsy in pregnancy are sparse. In one study of 27 pregnant patients with diagnosed ureteral calculi, eight underwent pneumatic lithotripsy, 17 underwent Holmium laser lithotripsy, and the two remaining patients were found to have lower ureteral stones <7 mm that were extracted with forceps. There were no reported intraoperative complications, and no observed abnormalities in the newborns. As such, the authors concluded that intracorporeal pneumatic and Holmium laser lithotripsy are appropriate treatment options in pregnancy. 80 Another, more recent retrospective study of 15 pregnant women treated for ureteral stones with Holmium laser lithotripsy reported no major complications and concluded that the modality is a reasonable alternative in the gravid patient. However, the authors did note limitations to their study, such as the retrospective nature and the small sample size. 81 While informative, these studies do not offer definitive evidence supporting the safety of these interventions in pregnancy. Indeed, lack of fluoroscopic control in the pregnant patient to avoid injurious radiation exposure demands advanced surgical technique and experience. Additionally, the risks of perioperative anesthesia to both the fetus and pregnant patient must still be considered. 82
Percutaneous nephrolithotomy
Percutaneous nephrolithotomy (PCNL) involves the creation of a percutaneous tract into the renal collecting system. 72 Given its invasive nature, it is typically reserved for larger or more complex calculi (>1.5–2 cm). 72 Unlike SWL, PCNL is not absolutely contraindicated in pregnancy; several successful PCNLs have been reported at 11, 14, and 22 weeks’ gestation.83–85 Nevertheless, it is avoided in pregnancy due to the more common utilization of prone position and the potential demand for significant fluoroscopy exposure with standard techniques. Modified PCNL in the supine position with ultrasound guidance and limited fluoroscopic use may be considered in the gravid patient in the presence of an experienced, multidisciplinary team. 83
Conclusion
The occurrence of nephrolithiasis during pregnancy can be a significant, anxiety-provoking experience for all involved. An understanding of the relevant pathophysiology may lead to new insights into future preventative and therapeutic options. Ultrasound remains a mainstay of diagnostic imaging in this group. Conservative management with a trial of passage should be an initial management option, with ureteroscopy having emerged as a preferred treatment option for those failing conservative measures. While other options for treatment exist, these should be considered with a careful assessment of the risks and benefits. Ultimately, a multidisciplinary approach involving urologists, obstetricians, and radiologists and anesthesiologists as needed is critical to maximizing safe outcomes for mother and child.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.