
Abstract
Following new scientific insights, initial management for patients with high-risk nonmetastatic prostate cancer has changed considerably and rapidly over the last few years. Several clinical and pathologic variables should be taken into account when deciding the best treatment choice for those patients. These variables are summarized and discussed in detail. High radiation doses to the prostate are essential to achieve good local control in patients with high-risk nonmetastatic disease. Addition of androgen deprivation therapy (ADT) to radiation therapy has significantly improved overall survival and cancer-specific survival compared with radiation therapy alone without significantly increasing toxicity. Long-term neo(adjuvant) ADT (2–3 years) to radiation therapy significantly improved cancer-specific survival compared with short-term ADT (4–6 months). Radical prostatectomy with extended pelvic lymph node dissection is considered a reasonable option in experienced hands. ADT alone is an inappropriate treatment option for patients with high-risk nonmetastatic disease. Management decisions for these patients should be discussed by a multidisciplinary team.
Introduction
Prostate cancer is the most commonly diagnosed nonskin cancer and is the second leading cause of cancer-related death among older men. 1 The majority of prostate cancer related deaths are due to locally advanced or metastatic disease. 2 In contemporary literature, the exact definition of locally advanced nonmetastatic prostate cancer is a matter of debate. For example, a clinical stage T3 is needed to define locally advanced disease in the National Comprehensive Cancer Network guidelines, whereas in the European Association of Urology (EAU) and European Society for Medical Oncology (ESMO) guidelines, as well as for D’Amico risk classification, a clinical stage of T2 combined with a prostatic specific antigen (PSA) level greater than 20 ng/ml or a Gleason score of 8–10 are sufficient to classify patients as having advanced disease (Table 1).3–6 To avoid confusion, the term high-risk nonmetastatic prostate cancer is preferably used to describe patients with nonmetastatic disease with high risk of progression and death based on their clinical and pathologic features. 5 Patients with an initial PSA level greater than 20 ng/ml, or a Gleason biopsy sum over 7, or a T3 lesion on digital rectal examination or imaging, or a clinical M0 stage are considered to have high-risk non-metastatic disease. 5 Around 10–20% of newly diagnosed prostate cancer cases involve locally advanced disease. Nonetheless, in the PSA era, this eventuality is less common since up to 82% of prostate cancers are diagnosed when the tumor is still localized to the prostate gland. 7 However, around 20% of these cases are at high risk of disease progression. 8 Approaching patients with high-risk nonmetastatic prostate cancer with the optimal management plan would have the most tremendous effect on prostate cancer mortality rates. However, the management of this group is highly heterogeneous worldwide. Several treatment choices are available, including watchful waiting, radiation therapy, radical prostatectomy (RP) with or without lymph node dissection, androgen deprivation therapy (ADT), and any combination of these. Following new scientific insights, initial management for these patients with high-risk nonmetastatic prostate cancer has changed considerably and rapidly over the last few years. The aim of our report is to summarize the evidence of clinical studies on treatment choice in patients with high-risk nonmetastatic prostate cancer and to translate this knowledge into individualized patient care. The role of ADT in treating patients with high-risk nonmetastatic cancer is analyzed in detail.
Definitions for locally advanced prostate cancer according to different scientific societies.

EAU, European Association of Urology; ESMO, European Society for Medical Oncology; NCCN, National Comprehensive Cancer Network; tPSA, total prostate specific antigen.
Management of non-metastatic high risk patients
Several clinical and pathologic variables are considered to guide the optimal treatment choice for patients with high risk nonmetastatic prostate cancer and include accurate staging of the disease, the patient’s life expectancy, and the Gleason score (Table 2). First, ruling out the presence of metastatic spread at the moment of diagnosis is of paramount importance in patients with high-risk features. All scientific societies are in line for mandating imaging in high-risk patients.3–5 Bone scan and pelvic tomography are the recommended imaging modalities despite their inherent limitations. New technological advances in metabolic imaging and nano magnetic resonance imaging have led to more sensitive tests that detect prostate cancer spread at an earlier stage. 9 A substantial number of patients classified as having nonmetastatic disease on conventional imaging would be reclassified as having metastatic disease if a more sensitive imaging technique were used.10,11 Second, life expectancy based on age and comorbidities should also be taken into account when managing patients with high-risk nonmetastatic disease. 12 Third, biopsy Gleason sum, PSA level, extracapsular extension, positive surgical margin upon resection, seminal vesicle invasion and lymph node status are the most important adverse prognostic factors that would dictate the choice of therapy. 13
Clinical and pathologic variables affecting the optimal treatment choice for patients with high-risk nonmetastatic prostate disease.

PSA, prostate-specific antigen.
Primary control for patients with a high-risk nonmetastatic prostate cancer profile
Both the combination of ADT and external beam radiation therapy (EBRT) or RP with extended pelvic lymph node dissection are appropriate treatment modalities for patients with high-risk nonmetastatic disease if the life expectancy is over 5 years. 5 The appropriateness of these treatment modalities according to the life expectancy is not yet clear but cancer-specific mortality should always be balanced against other-cause mortality.14,15
EBRT and neo(adjuvant) ADT
The evidence in favor of radiation therapy and ADT is based on several randomized clinical trials (Table 3). Compared with radiation therapy alone, the combination of radiation therapy and ADT significantly decreased the risk of biochemical failure, clinical progression, local relapse, and distant metastases by 24%, 19%, 36%, and 28%, respectively, without increasing the risk of toxicity [relative risk (RR) 0.92; 95% confidence interval (CI) 0.87–1.11], genitourinary toxicity (RR 0.66; 95% CI 0.36–1.22), gastrointestinal toxicity (RR 0.69; 95% CI 0.46–1.03), and cardiac death (RR 0.87; 95% CI 0.70–1.09). 22 Overall, the addition of ADT to conventional-dose radiation therapy improved overall survival and cancer-specific survival without significantly increasing toxicity.22–25 In a meta-analysis, adding ADT to radiation therapy decreased risk of death from prostate cancer by 24% and risk of death by any cause by 14%. 22 It is noteworthy that all these trials were performed in the era of suboptimal radiation therapy doses, with the highest dose administered 66 Gy, while at present the recommended dose is 76–78 Gy.4,19 Subsequently, it would be of interest to reconsider these results in the era of new radiation therapy recommendations and technologies. At present, there is no evidence to avoid ADT with high-dose radiation therapy in the treatment of patients with high-risk nonmetastatic disease. In a retrospective analysis, Stenmark and colleagues demonstrated that the benefit of combining ADT and radiation therapy depends on the number of adverse risk factors. 26 Compared with those receiving ADT and radiotherapy, the risk of dying from prostate cancer in patients receiving radiation therapy alone was 4.8, 6.7, and 22.8 times higher if there were one, two, or three adverse risk factors, respectively. In this study, a Gleason score above 8 was the most adverse factor when considering the benefit of adding ADT to radiation therapy. In patients with high-risk prostate cancer, the combination of long-term adjuvant ADT and radiation therapy was shown to significantly improve overall survival compared with short-term ADT.27,28 In the European Organisation for Research and treatment of Cancer (EORTC) 22961 noninferiority trial and the Radiation Therapy Oncology Group (RTOG) 9202, the combination of long-term adjuvant ADT to RT significantly improved overall survival, cancer-specific survival, and distant metastasis free survival compared with short-term ADT. In this specific study, 62% of patients received triptorelin, 30% received goserelin, and 8% received other Gonadotrophin releasing hormone (GnRH) agonists. 27 These results require validation in new randomized controlled trials to reinvestigate the benefit of the combination of high doses of radiation therapy and ADT. In the actual state of knowledge, the combination of short-term ADT and radiotherapy did not show any benefit in low-risk patients while it decreased disease-specific mortality and increased overall survival in intermediate-risk patients. As for high-risk patients, the combination of long-term ADT and radiation therapy remains the standard of care.19,29
Benefits of adding neo(adjuvant) ADT to radiation therapy.
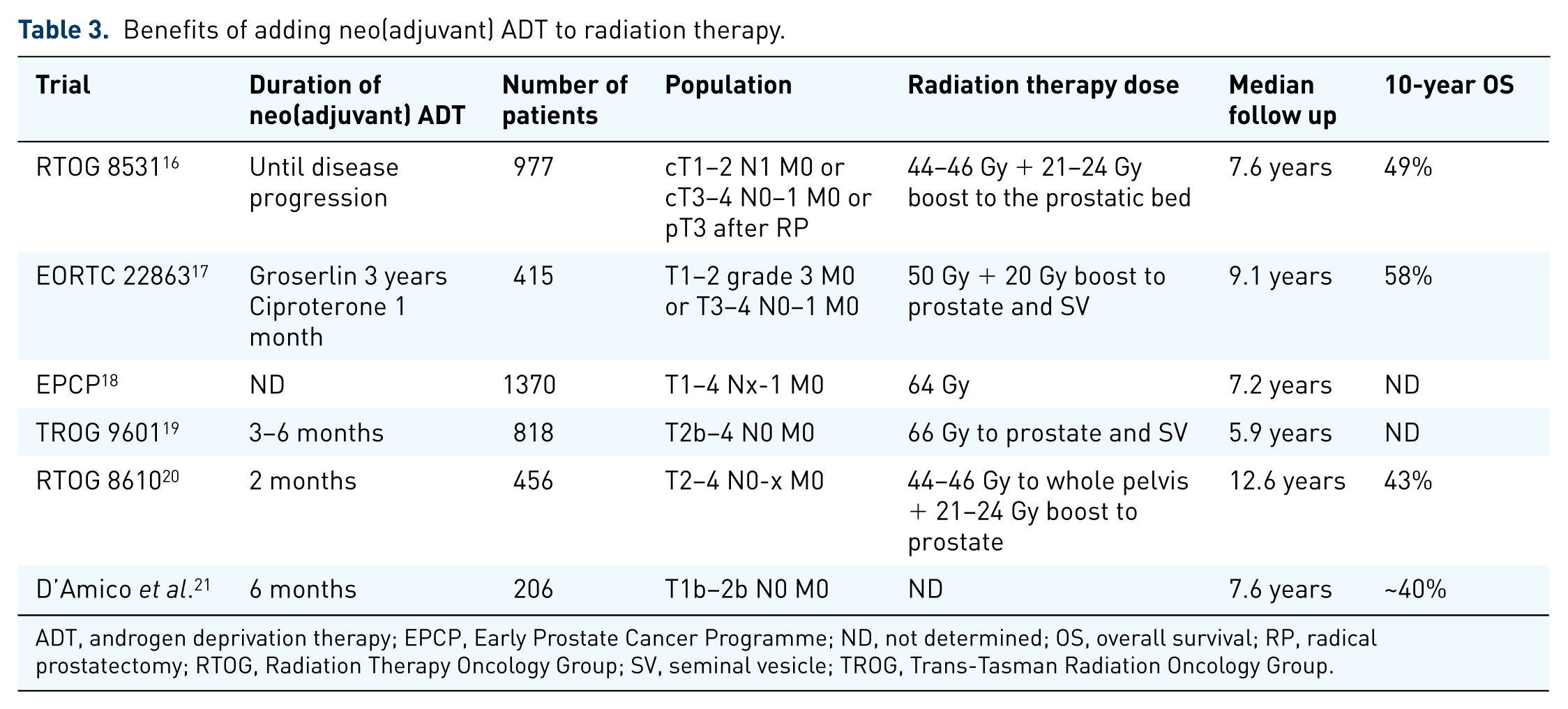
ADT, androgen deprivation therapy; EPCP, Early Prostate Cancer Programme; ND, not determined; OS, overall survival; RP, radical prostatectomy; RTOG, Radiation Therapy Oncology Group; SV, seminal vesicle; TROG, Trans-Tasman Radiation Oncology Group.
RP and extended pelvic lymph node dissection
The evidence in favor of surgery is based on large retrospective series from high-volume centers. The potential advantages of surgery as a monotherapy or as a first step in a multimodal approach is to accurately stage the tumor burden and arguably to better select patients needing adjuvant treatment. An extended pelvic lymph node dissection, a complete resection of the seminal vesicles, a clean apical dissection, a neurovascular bundle resection at the tumor bearing site, and a resection of the bladder neck when the tumor is located at the base are mandatory steps to achieve adequate local control. 30 Retrospective data have shown good oncologic outcomes, with 10-year cancer-specific survival varying between 60% and 92% in men with high-risk nonmetastatic prostate cancer.19,30–32 In these studies, cancer-specific survival rates were shown to decrease with the number of primary adverse risk factors at diagnosis, such as PSA level above 20 ng/ml, biopsy Gleason sum at least 8, clinical stage T3 or higher, and the presence of seminal vesicle invasion. In a retrospective multiexpert center cohort study, the authors divided 1360 patients into three groups according to adverse risk factors. 33 Based on their results, patients within the good prognosis group (PSA levels above 20 ng/ml, or cT3–4, or Gleason score above 7) might be treated with RP and extended pelvic lymph node dissection as a monotherapy, while patients within the poor prognosis group might need adjuvant therapy. The long-term results of the EORTC 229111 randomized controlled trial on postoperative radiotherapy following RP demonstrated increased biochemical recurrence-free survival rates in patients with positive surgical margins and in those younger than 70 years. In patients older than 70 years, postoperative adjuvant radiation therapy accounted for higher genitourinary toxicities. 34 A biochemical recurrence-free survival advantage was also observed in patients with RP for pT3 and positive surgical margins with early radiation therapy compared with observation in the ARO 96-02 trial (56% versus 35%; p < 0.001).35,36 Consequently, the role of adjuvant radiotherapy was criticized in view of the lack of benefit in overall survival. The update of the SWOG 8794 trial revealed increased overall survival (median 15.2 years versus 13.5 years; p = 0.031) with increased metastatic-free survival (p = 0.021), indicating an unequivocal benefit for adjuvant radiotherapy compared with observation. 37 A systematic review and meta-analysis of these three randomized clinical trials demonstrated a progression-free survival benefit in favor of adjuvant radiation therapy compared with observation [hazard ratio (HR) 0.48; 95% CI 0.42–0.55] without excess severe late toxicity. 38 Nevertheless, in day-to-day practice, clinicians often offer salvage radiation therapy to patients experiencing biochemical failure rather than adjuvant radiation therapy. New retrospective data with the longest follow up demonstrated distant metastasis-free survival rates at 5 years as high as 94% for all patients treated with salvage radiation therapy. 39 However, in the absence of randomized prospective clinical trials comparing adjuvant radiotherapy and salvage radiation therapy, one must seriously consider the advantages and disadvantages of each approach and modulate decisions by taking into account the pathology of the disease and the comorbidity of the patient. Early salvage radiation therapy after RP might not compromise oncologic control compared with adjuvant radiation therapy but it is currently under investigation in an ongoing multicenter phase III trial [ClinicalTrials.gov identifier: NCT00860652]. Recently, the eagerly awaited results of the RTOG 9601 trial were released. The results supported adding bicalutamide 150 mg to radiation therapy for salvage treatment following RP. Adding 24 months of such salvage treatment for patients with pT2N0 and pT3N0 reduced the risk of death by 23% compared with radiation therapy alone without causing undue toxicity (only gynecomastia). The number needed to treat to avoid one death was only 12. In a subgroup analysis, patients who benefitted the most were those with a Gleason score of 7–10, positive surgical margin, or those having a PSA level between 0.7 and 4.0 ng/ml. 19 Interestingly, the newly released results of a multi-institution validation study of the Decipher Prostate Cancer Classifier (Clinical Laboratory Improvement Amendments [CLIA] Laboratory, San Diego, CA), a genomic test for prostate cancer, might be used in the near future to improve clinical decisionmaking following RP. In this trial, patients who received RP and had an undetectable PSA in the postoperative setting were randomized into four arms. The first group received no postoperative treatment prior to developing metastasis. The three other groups were divided according to PSA levels. Patients with PSA levels less than 0.2 ng/ml were treated with adjuvant radiation therapy. Patients with minimal residual disease (PSA levels between 0.2 and 0.49 ng/ml) were offered salvage radiotherapy, while patients with PSA levels at least 0.5 ng/ml were considered for salvage radiotherapy. Based on the Decipher genomic test, patients with adverse pathological features and high genomic risk benefit from an aggressive approach of adjuvant radiation therapy or early salvage radiation therapy to avoid developing metastases. In contrast, men with lower genomic risk and good pathological features might be offered observation after RP. 40
Systemic therapy for patients with a high risk nonmetastatic prostate cancer profile
ADT monotherapy is an inappropriate treatment option in patients with high-risk nonmetastatic prostate cancer. There is currently no conclusive evidence that immediate primary ADT prolongs survival compared with conservative management in patients with high-risk prostate cancer.18,41 Immediate ADT was demonstrated to prolong cancer-specific survival compared with deferred ADT only in patients with a PSA level above 50 ng/ml or a PSA doubling time less than 12 months who were unsuitable for treatment with curative intent. 42 This survival benefit is modest and should be weighed against the side effects of prolonged ADT in this setting. A Scandinavian multicenter randomized controlled trial (SPCG-7/SFUO-3) examined the benefit of adding neo(adjuvant) three-dimensional conformational radiation therapy to ADT in patients with T3N0M0 prostate cancer. The authors demonstrated an improved overall survival and cancer-specific survival with an increase in genitourinary toxicity. 43 A more recent multicenter randomized controlled trial (PR/PR07) using modern radiation technology showed similar late-grade gastrointestinal toxicity when adding radiation therapy (65–69 Gy to prostate and seminal vesicle with or without 45 Gy to pelvic lymph nodes) to ADT compared with ADT alone. 44 In this trial, overall survival and cancer-specific survival were significantly improved in the group receiving radiation therapy and ADT compared with those receiving ADT alone. 44 A systematic review of 10 randomized controlled trials investigating neo(adjuvant) ADT prior to RP compared with RP alone demonstrated similar overall survival or disease-free survival. The only difference is that the neo(adjuvant) ADT allowed more organ confinement. In a subanalysis, patients with positive surgical margins or lymph node invasion did benefit from neo(adjuvant)ADT but the survival benefit was modest. 23 According to the EAU guidelines, adjuvant ADT is the standard of care in patients with lymph node invasion while there is no evidence for adding ADT to RP in patients with seminal vesicle invasion. 4 Patients with high-risk prostate cancer receiving adjuvant ADT showed minor benefits, with a 5-year overall survival of 95.9% (95% CI 93.9–97.9). 45 Adjuvant radiation therapy with ADT may still have a role. In a retrospective match controlled study of pT2–4 pN1 patients who underwent RP with extended pelvic lymph node dissection, adjuvant ADT and radiation therapy improved overall survival compared with adjuvant ADT monotherapy but randomized controlled trials are needed to confirm these findings. 46 In patients with a life expectancy of less than 5 years, neither surgery nor ADT are appropriate treatment options. The appropriateness of a therapy combining EBRT and ADT is uncertain in contemporary literature. However, in the presence of a Gleason score of 8 or higher and a combination of clinical stage T3 and a PSA level above 20 ng/ml that can cause detrimental prognosis within 1–2 years, the use of EBRT and long-term ADT is recommended. If EBRT cannot be used in this setting, ADT monotherapy can be offered. 5 Furthermore, there is no current role for adjuvant chemotherapy after RP. In the first survival results from STAMPEDE that were recently released, newly diagnosed patients with metastatic disease, node-positive disease, or at least two of the following criteria: stage T3–4, PSA at least 40 ng/ml and Gleason score 8–10, were randomized into two arms. In the first arm, standard of care was given while in the second arm immediate chemotherapy was administered. In patients with nonmetastatic disease, adjuvant chemotherapy did not add any survival benefit. 47 In addition, the results of the SPCG12 trial, a randomized open-label phase III trial of adjuvant docetaxel and surveillance after RP for high-risk prostate cancer, were recently published. 48 On multivariate analysis, the treatment arm was not a risk factor for progression and more deaths occurred in the adjuvant docetaxel arm compared with the surveillance group.
Conclusion
The management options for patients with high-risk nonmetastatic prostate cancer should always be discussed in a multidisciplinary team setting. The discussion with the patient in the light of his clinical and pathologic characteristics is paramount in order to offer him the best treatment strategy and to avoid unnecessary harm. Clinicians should be aware that ADT alone is an inappropriate treatment option for patients with high-risk non-metastatic disease. An accurate workup to rule out metastatic spread is mandatory before offering aggressive local control modalities.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.