
Abstract
In 2005, the high power thulium laser was introduced for the surgical treatment of benign prostatic obstruction. It has several properties that confer theoretical advantages over other lasers used for the same indication, such as technical versatility and a relatively small zone of thermal damage. Studies using the 70–150 W thulium laser systems demonstrate good efficacy of these procedures with low morbidity and few complications even in higher risk patients. Different techniques have been employed to treat the prostate with this technology, including enucleation, vapoenucleation, vaporization and resection. Comparative studies have been published comparing thulium laser prostatectomy to monopolar transurethral resection of prostate (TURP), bipolar TURP and holmium laser enucleation of prostate (HoLEP). In this review we discuss the current literature on the safety and efficacy of various thulium techniques for the treatment of benign prostatic hyperplasia and examine comparative studies.
Introduction
According to the Urologic Diseases in America project, benign prostatic hyperplasia (BPH) affects 70% of men in the US aged 60–69 and 80% of those aged 70 or older [Wei et al. 2005]. The Rancho Bernardo study, a longitudinal population-based study, found that 56% of men aged 50–79, 70% of men aged 80–89 and 90% of men aged 90 or older reported experiencing lower urinary tract symptoms (LUTS) [Parsons et al. 2008]. Multiple surgical options are available for the treatment of BPH and its associated symptoms, with transurethral resection of the prostate (TURP) remaining the gold standard surgical treatment with the longest follow-up data available. Although traditional TURP is both efficient and effective, it is associated with significant morbidity from bleeding and fluid shifts, including a 2–8% transfusion rate [Mebust et al. 1989; Rassweiler et al. 2006]. TURP rates have declined over the past two decades due to the significant benefits of medical therapy and the proliferation of alternative surgical techniques that include laser therapies for BPH. Yu and colleagues analyzed practice patterns and found that, by 2005, traditional TURP accounted for 39% of surgical interventions for BPH while laser procedures accounted for 57% [Yu et al. 2008]. There are several different types of minimally invasive laser procedures including enucleation, vaporization, vapoenucleation and resection.
The high power thulium laser was first introduced in 2005 for the treatment of BPH [Xia et al. 2005]. Similar to holmium technology, at 2010 nm, the wavelength of the thulium laser is very close to the peak for absorption in water, which is 1940 nm. However, unlike the pulsed wave holmium laser, this high density energy is delivered in a continuous wave. This theoretically translates to more efficient vaporization and shallower depth of penetration in tissue, which has been reported to be 0.2 mm as compared with 0.4 mm for holmium lasers [Fried and Murray, 2005]. This property likely also results in a smaller zone of thermal damage, which in turn may help to decrease postoperative dysuria, an adverse effect that is commonly associated with transurethral laser prostate surgery [Rieken et al. 2010]. The fiber is diode pumped which gives it the capability of operating in either a pulsed mode or a continuous wave mode. The continuous wave mode is more suitable for hemostasis and coagulation of tissue, whereas the pulsed mode for is more suited for lithotripsy [Hardy et al. 2014].
Studies using the 70–150 W thulium laser systems demonstrate good short-term efficacy with low morbidity and few complications [Gross et al. 2012]. This paper reviews the current evidence of safety and efficacy of the various thulium laser techniques for the treatment of BPH and the comparative studies.
Methods
A PubMed search for papers from 2005 to 2015 was conducted using the words ‘thulium laser prostate’. A total of 112 papers were obtained. After case reports, abstracts only and papers not in English were excluded, 98 articles remained. We reviewed all case series, review papers, cohort studies, and retrospective and prospective studies relevant to the topic covered in this review. We then scanned the references of the articles used to capture any additional relevant papers which would make this manuscript more comprehensive.
Surgical techniques
Several techniques using the thulium laser have been described for laser prostatectomy including thulium vapoenucleation (ThuVEP) and thulium laser resection of the prostate (TmLRP) (the ‘tangerine’ technique), thulium laser enucleation (ThuLEP) and thulium vaporization (ThuVP) (Table 1). In the authors’ opinion, for smaller prostates all techniques are similarly efficient and feasible. The end-fire fiber in combination with effective vaporization of the thulium laser system lends itself to both vaporization and enucleation. Hence, the choice of technique in smaller prostates is mostly driven by surgeon preference. For larger prostates (i.e. size >100 ml), enucleation techniques are more efficient and effective. ThuVEP and ThuLEP are almost identical techniques in description. There may be a greater proportion of mechanical, as opposed to laser, enucleation in the ThuLEP technique.
Thulium non-comparative observational studies.
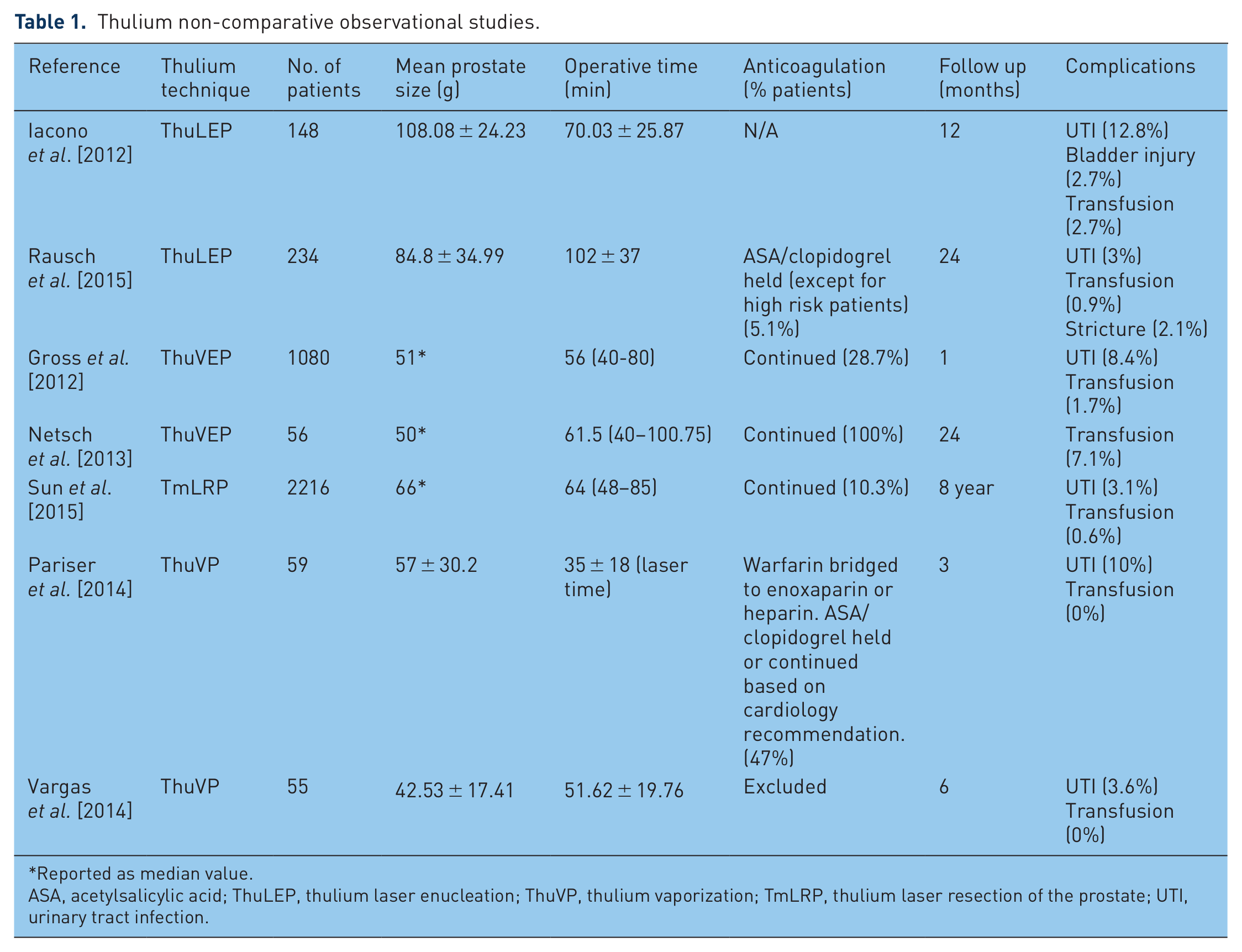
Reported as median value.
ASA, acetylsalicylic acid; ThuLEP, thulium laser enucleation; ThuVP, thulium vaporization; TmLRP, thulium laser resection of the prostate; UTI, urinary tract infection.
There are two main high power thulium laser systems: the CyberTM (Quanta System, Solbiate Olona, Italy; 150W, 200W) and the Revolix® (Lisa Laser, Katlenburg-Lindau, Germany; 30W, 70W, 120W and 200W systems). The authors have used both systems at the same power level and there does not appear to be a noticeable difference in vaporization efficiency.
Vapoenucleation (ThuVEP)
Vapoenucleation is the most commonly described technique and involves trilobar enucleation using a combination of laser and mechanical energy followed by intravesical morcellation, similar to holmium laser enucleation of prostate (HoLEP) [Bach et al. 2009a, 2009b]. The continuous wave of the thulium laser leads to a very different interaction with prostate tissue compared with the pulsed holmium laser, which is the reason the technique has been coined ‘vapoenucleation’. The majority of studies are short term and there is large heterogeneity in patient populations making the studies difficult to compare.
The first studies were performed in small prostates where the tissue chip size was small enough to avoid the need for morcellation. Bach and colleagues reported on a single surgeon feasibility series of 54 men with a mean prostate volume 30.3 (range 12–38) cm3 who underwent vaporesection of the prostate with the 70W RevoLix® (Lisa Laser Products, Katlenburg-Lindau, Germany) laser system with a wavelength of 2013 nm [Bach et al. 2007]. Improvements were seen in mean International Prostate Symptom Score (IPSS) (19.8 to 6.9), maximum flow rate (Qmax) (4.1–20.1 ml/s) and postvoid residual (PVR) (86–12 ml) compared with preoperative paramaters. No patients required transfusion or rehospitalization. A total of six (11%) patients developed a symptomatic urinary tract infection (UTI) requiring antibiotic therapy.
Following this feasibility study, this same group of authors investigated the feasibility and efficacy of thulium:YAG (Tm:YAG) laser vapoenucleation of the prostate in larger prostates [Bach et al. 2009b]. In this short-term study, with follow up to discharge, 88 patients with a prostate volume of 61.3 ± 24.0 cm3 underwent vapoenucleation of the prostate with the 70W RevoLix® Tm:YAG laser. In contrast to the previous study, morcellation was performed in all patients following enucleation. The complication rate was 16.6%, with 12 patients having complications: two (2.2%) patients required blood transfusions for postoperative bleeding; six (6.8%) patients developed symptomatic UTIs; three (3.4%) patients experienced intra- or postoperative bleeding; and two (2.2%) underwent a second-look procedure during the same hospital stay due to inability to void. Significant improvements were seen at discharge in Qmax (3.5 ± 4.7–19.8 ± 11.6 ml/s) and PVR (121 ± 340–22 ± 33 ml).
This same group reported on complications and early postoperative outcomes of ThuVEP performed by 11 surgeons at a single institution in an impressively large series of 1080 patients using various generations of the thulium laser between 70W and 200W [Gross et al. 2012]. This was a short-term analysis examining preoperative characteristics, surgical details and immediate outcomes.
Median age at surgery was 71 years and prostate size was 52 ml [interquartile range (IQR) 36–79] with a median operation time of 56 minutes. A total of 22% of patients were in retention prior to surgery. Median enucleation time was 33 minutes (IQR 22–50) and median resected tissue weight was 30 g (IQR 36–78). Significant changes were seen after surgery in median maximum flow rate (8.9 versus 18.4 ml/s, p < 0.001) and PVR (120 versus 20 ml, p < 0.001) compared with before surgery. Median catheterization time was 2 days (IQR 2–2) and median hospital stay was 4 days (IQR 3–5).
The overall immediate morbidity rate was 16.9%. Minor complications (Clavien class 1 and 2) occurred in 262 (24.6%) patients. Within 4 weeks, 71 (6.6%) patients required intervention (Clavien 3a: 0.6%; Clavien 3b: 6%). One patient had a Clavien 4a complication and had an acute myocardial infarction. No mortalities were seen.
The most frequently reported complications were urinary retention after catheter removal (9%), UTI without bacteremia (6.9%), clot retention without surgical revision (3.5%), residual prostate tissue requiring reoperation (2.7%), capsular perforation (2.1%), hemorrhage requiring reoperation (2%), bleeding requiring blood transfusion (1.7%), UTI with signs of bacteremia (1.5%), extraperitoneal fluid collection (1.5%), superficial bladder injury due to morcellation (1.4%), ureteral orifice injury (0.7%) and hydronephrosis due to ureteric orifice injury (0.6%). The overall reoperation rate was 4.7% and the readmission rate was 4.1%.
A subanalysis was performed and patients were stratified by prostate size. Group A had a prostate size <40 ml (28%), Group B had a prostate size 40–79 ml (47%) and Group C had a prostate size ⩾80 ml (25%). No differences were seen in complications rates between the groups.
The complication rate using the Clavien classification system (CCS) were then compared with those in published series of HoLEP, photoselective vaporization of the prostate (PVP), TURP and open prostatectomy. Overall in this large series, immediate outcomes and complication rates for ThuVEP were similar to those in large series of HoLEP and PVP and lower than in TURP and open prostatectomy. This large series confirmed that ThuVEP is a safe and effective procedure for the treatment of symptomatic BPH with low perioperative morbidity.
There are many strengths of this large series of patients including adequate power, multiple surgeons and use of standardized reporting methods for complications. However, the fact that it was a single center study and that various generations of the thulium laser were used may not make the results generalizable to some populations.
Studies support the use of ThuVEP in medically complex patients, such as high risk cardiopulmonary patients on oral anticoagulation, with few perioperative complications. Macchione and colleagues investigated the safety and efficacy of ThVEP using the 120-W Tm:YAG laser (Revolix Duo) in 76 patients who were taking oral antiplatelet or anticoagulation. In 41 patients (group A), the procedure was performed while patients continued oral anticoagulation and, in 35 patients (group B), oral anticoagulation was discontinued 10 days prior to surgery and patients were bridged with low molecular weight heparin (LMWH) for 2 weeks, with 3 (8%) patients from this group taking warfarin [Macchione et al. 2013].
In group A, 5 (12%) patients were taking warfarin, 20 (48%) acetylsalicylic acid (ASA), 12 (29%) ticlopidine, and 4 (10%) ASA and clopidogrel. In group B, 3 (8%) patients were taking warfarin, 15 (42%) ASA, 11 (31%) ticlopidine and 6 (17%) ASA and clopidogrel. All procedures were performed by a single surgeon. The decision to discontinue oral anticoagulation was made by the consultant cardiologist. In both groups, mean age was similar (69 ± 7 for both) as well as mean prostate size (65 ml for both). Median ASA for both groups was 3. Operative times (48 ± 8, 47 ± 5 minutes), catherization time (1.5 ± 6, 1.6 ± 6 days), hospital stay (2.3 ± 0.9 and 2.4 ± 9 days), mean drop in sodium (0.52 ± 2.0 and 1.34 ± 1.1 g/L) and mean hemoglobin drop (0.35 ± 0.2 and 0.85 ± 0.2 g/l) were similar between groups A and B. Only one patient in group A required a transfusion. A total of three (4%) patients overall required continuous bladder irrigation for postoperative hematuria. Significant improvements were seen compared to baseline in Qmax, IPSS, PVR and quality of life (QoL) at 3 and 6 months postoperative.
Thulium laser resection of prostate (TmLRP)
TmLRP was initially applied in 2004 by Xia and colleagues in the treatment of BPH [Xia et al. 2005]. Described as the ‘tangerine technique’, resection is carried out by dissection of whole prostatic lobes off the surgical capsule similar to that of peeling a tangerine. Tissue is vaporized sufficiently so that small pieces may be removed via a resectoscope without requiring use of a morcellator [Xia, 2009]. Several studies with short-term follow up have demonstrated excellent safety and efficacy of this technique [Xia et al. 2008; Fu et al. 2010].
In 2014, Sun and colleagues evaluated the long-term durability and complication rates after TmLRP through a large, prospective, multicenter study [Sun et al. 2015]. A total of 2016 patients were treated with TmLRP at four medical centers and were followed for up to 8 years (61.1% followed for 5 years, 24.4% followed for 8 years). A Tm:YAG laser was used with a laser power level at 50W, 70W or 120W in all patients.
IPSS, QoL, Qmax and PVR were all significantly improved at 3 months after surgery and remained significantly improved during the entire follow-up period. IPSS and QoL decreased by 72.3% and 75%, respectively; Qmax had increased by 178% and PVR had decreased by 81.8% by the end of follow up. At 3 months, 1 year and 8 years postoperatively, median IPSS was 7, 6 and 6, respectively; median QoL was 1, 1 and 1; median Qmax was 21.7, 22.3 and 19.2 ml/s, respectively; and PVR was 22, 18 and 20 ml. These results showed sustained long-term improvement in all urinary parameters post TmLRP. Short-term Clavien 1 and 2 complications occurred in 23.7% of the patients. A total of 9% patients had some type of temporary urinary incontinence and only 3% of patients were reported to have UTI. A total of 6% of patients went into urinary retention requiring catheterization and 3% had clot retention requiring bladder irrigation. Blood transfusion was required by 13 (0.6%) patients and eight (0.4%) developed deep vein thrombosis and pulmonary embolus. There was evidence of systemic infection in 29 (1.3%) patients. Clavien 3 complications, requiring re-intervention occurred in 2.2% of the patients. Resection of residual tissue was required in 11 (0.5%) patients and 37 (1.7%) patients underwent cystoscopy for bleeding. In the cohort of 556 patients with prostate size >80 g, there was no difference in overall, Clavien 1, 2 or 3 complications compared with the patients with prostate size <80 g.
One unique aspect of this study was the reporting of long-term complications. Urethral stricture and bladder neck contractures occurred in 2.6% and 1.6% of patient, respectively. Persistent stress incontinence was found in two patients (0.1%). Re-operation as a result of BPH recurrence was required in 1.2% of patients over the course of up to 8 years.
Of note, this study also included 228 patients who were taking oral anticoagulants (aspirin and/or clopidogrel) at the time of surgery. There was no difference in overall, Clavien 1, 2 or 3 complications between those taking anticoagulants and not. Additionally, there was no difference in perioperative bleeding between the two groups (1.3% risk on anticoagulation versus 0.7% risk off anticoagulation, p = 0.41) This study offers a particular robust analysis given its prospective, multi-centered design, long-term follow up and inclusion of a diverse patient profile including varied prostate size and patients at higher risk of cardiopulmonary or bleeding complications than those on anticoagulation.
Thulium laser vaporization of the prostate (ThuVP)
Although the thulium laser is well suited to vaporization, it is only recently that the safety and efficacy of ThuVP has been reported. Pariser and colleagues reported short-term outcomes of ThuVP using the 150W (Cyber™) thulium laser in the US, which was the first study to be published on outcomes on any technique for thulium laser prostatectomy in a North American patient population. A total of 59 patients with mean prostate volume of 57 ± 30.2 ml underwent ThuVP; 47% of the patients were taking oral anticoagulation at baseline with aspirin, clopidogrel, warfarin or enoxaparin. The majority (78%) of patients were discharged home the same day of surgery. Although there was a significant change in hemoglobin from baseline (13.1–12.4 g/dl), no patients received blood transfusions and the drop was similar to that seen in 532 nm laser studies [Pariser et al. 2014].
At 3 months, mean Qmax and PVR were significantly improved. Subjective measurements (IPSS and QoL) also demonstrated significant improvements from baseline at all follow-up intervals. At 3 months, IPSS was 8.7 ± 6.5 compared with 19.9 ± 8.0 at baseline and QoL was 2.1 ± 1.4 compared with 4.5 ± 1.1 at baseline (p < 0.05). All 15 patients who presented in retention were voiding spontaneously at the time of their last follow up. The overall 30-day complication rate was 20%, with all complications graded as Clavien 1 and 2. A total of 10% of patients needed catheterization for urinary retention (half of these were in retention prior to surgery) and 10% developed symptomatic culture-proven UTIs. There were no immediate higher grade complications. Between 30 and 90 days, 1 patient developed a urethral stricture and 1 a bladder neck contracture. Both were successfully managed endoscopically and represent the only Clavien grade 3 complications [Pariser et al. 2014].
Around the same time, Vargas and colleagues also published outcomes of 150W ThuVP with 6 months of follow up in 52 patients in Spain. Prostate size was comparatively smaller with median 51 ml (IQR 36–78.7 ml) and patients on anticoagulation were excluded. Patients were also discharged home the same day of surgery. Significant improvements were seen in Qmax (mean improvement 9.33 ml/s) and mean IPSS (reduction by 17 points). Immediate complications were recorded at 1 month follow up and included acute urinary retention (one patient), urinary tract infection (two patients) and gross hematuria (two patients). The only late complication observed (assessed at the 6 month mark) was bladder neck contracture, which was seen in one patient. Again within 30 days, no Clavien grade 3 or higher complications were seen [Vargas et al. 2014]. No comparative data are available for ThuVP, although this technique appears to have short-term complications similar to those described after vaporization with other laser systems as well as TURP [Reich et al. 2008; Pereira-Correia et al. 2012].
Thus far, early short-term studies on ThuVP appear promising and outcomes appear similar to those from 532 nm vaporization but further long-term and comparative studies are needed.
Thulium laser enucleation of the prostate (ThuLEP)
ThuLEP is extremely similar to ThuVEP except that enucleation of the adenoma is done mechanically without the use of energy. The initial cuts are still made with the laser [Kyriazis et al. 2012]. Due to the continuous pulse, vaporization occurs whenever the laser is employed. Indeed, in papers the description between the two techniques is often indistinguishable [Bach et al. 2009a, 2009b].
Iacono and colleagues described a series of 148 men who underwent ThuLEP with large prostate size (108 ± 24 ml) who underwent the procedure using the 120W RevoLix laser with 12 months of follow-up. Significant improvements were seen in IPSS, QoL, and PVR [Iacono et al. 2012]. Complications included UTI in 19 patients (12.8%), postoperative urgency incontinence in 10 (6.7%), early recatheterization with residual tissue at prostatic apex in four patients (2.7%), blood transfusion in four patients (2.7%) and bladder injury during morcellation in 2 patients (1.3%). There was significant increase in IIEF but the absolute difference in score was very small (19.3 ± 8.2–20.3 ± 8.2, p < 0.05).
In a recent series, Rausch and colleagues performed ThuLEP between 2008 and 2012 in 234 patients with a mean prostate size of 84.8 ± 34.9 ml using the RevoLix (power not specified). Overall the 30-day complication rate was 19.7%. In the perioperative period, only 3% of patients experienced a UTI, 6.8% required catheter replacement and 0.9% required a blood transfusion. In the postoperative period, 3% experienced urgency incontinence and 2.1% experienced bladder neck stricture [Rausch et al. 2015]. Complications occurring after 30 days included stress incontinence in one patient (0.5%) and inability to void requiring chronic catheterization in 19 (8.1%) patients. Predictors of complications in univariate and multivariate analysis were age >80 years and prostate size <50 ml.
Very few studies have addressed sexual outcomes in detail following any thulium laser prostatectomy. In 2015, Carmignani and colleagues evaluated sexual outcomes in 110 men undergoing ThuLEP with the Cyber 150™ W laser in a prospective study using validated instruments. Patients were evaluated before surgery and at 3 and 6 months after ThuLEP with IPSS, IIEF-5 and ICIQ-Male Sexual Matters associated with Lower Urinary Tract Symptoms (ICIQ-MLUTSsex) [Carmignani et al. 2015]. While a significant and sustained improvement in the scores evaluating urinary symptoms was observed, there were no significant differences in erectile function before and after surgery.
Comparative studies
Comparative studies to traditional TURP
Several comparative studies of thulium laser prostatectomy and other transurethral techniques are available (see Table 2), mostly originating in Asia. Several studies have been published comparing thulium laser prostatectomy with standard monopolar TURP [Xia et al. 2008]. Using a 50W continuous wave thulium laser (LISA Laser Products OHG, Germany), Xia and colleagues performed TmLRP and compared outcomes up to 12 months with standard TURP. Patients in urinary retention were excluded. A total of 52 patients were randomized to TmLRP and 48 to TURP. Operative time for both procedures were also similar for TmLRP and TURP (46 ± 16 and 50 ± 20 minutes, p = 0.28). There was a smaller decrease in hemoglobin in the TmLRP group versus TURP (0.92 ± 0.82 versus 1.46 ± 0.65 g/dl, p = 0.0004). Hospital stay (115 ± 24 versus 161 ± 34 hours, p < 0.0001) and catheterization time (46 ± 26 and 87 ± 34 hours, p < 0.0001) were also shorter in the TmLRP group compared with TURP. At 1, 6 and 12 months follow up, no significant differences were seen between groups in IPSS, QoL, Qmax or PVR. No significant changes in IIEF-5 scores were seen compared with preoperative in either group [Xia et al. 2008]. Regarding adverse effects, there were two (4%) transfusions required in the TURP group but none required in the TmLRP group. No significant differences were found with regard to rate of transfusion, TURP syndrome or UTI. No differences were seen in either the rate of de novo stress urinary incontinence or urethral strictures. Overall, this study suggested that subjective and objective improvements of this technique are similar to TURP but with lower morbidity.
Comparative studies.

BiTURP, bipolar transurethral resection of the prostrate; ThuLEP, thulium laser enucleation; ThuLRP, thulium laser resection of the prostate; ThuVEP, thulium vapoenucleation; TURP, transurethral resection of the prostate.
More recently, Cui and colleagues performed a randomized trial comparing the safety and efficacy of standard TURP compared with TmLRP with outcomes to 4 years. Patients were randomized to the TmLRP (49)and TURP (57) groups. The authors found that the degree of improvement in all micturition parameters including IPSS, QoL, PVR and Qmax were near comparable in both the TmLRP and the TURP patients at every time point of follow up to 48 months. Details of the short-term complications were not reported. Long-term re-operation rates for BPH recurrence and rate of bladder neck contracture were similar in the two groups, although the study may be underpowered to look at these parameters [Cui et al. 2014].
Chang and colleagues recently reported a study that compared a high-power 150W CyberTM ThuVEP with standard TURP with a 1-year follow up. A total of 29 patients were assigned to have ThuVEP and 30 to TURP. Voided volume, Qmax, PVR and mean flow rate all improved significantly in both groups and there were no differences in IPSS or QoL after 1 year of follow up. The transfusion rate in this study was 13.8% in the ThuVEP group and 26.7% in the TURP group, which is higher than that reported in other studies using the high power laser [Gross et al. 2012; Pariser et al. 2014]. This may be due to a lower threshold for transfusion in the older patient population of this study (mean age: ThuVEP 76; TURP 72). There was minimal change in hemoglobin level before and after the operation (ThuVEP: 0.5 ± 1.3 g/dl; TURP: 0.5 ± 1.1 g/dl) [Chang et al. 2015]. Because operative time was not reported and baseline patient characteristics are very different to those in the previous studies, it is difficult to make a conclusion in regard to the benefit of the higher power laser compared with the 50W laser used by Xia and colleagues in 2008.
A meta-analysis using nine trials to examine the performance of TmLRP versus TURP indicated TmLRP to be a safe, feasible and efficient alternative to TURP for treating patients with BPH with reliable perioperative safety, fewer complications, and comparable efficacy in relation to Qmax, PVP, QoL and IPSS. Patients undergoing TmLRP experienced smaller declines in serum sodium levels (p < 0.0001), hemoglobin levels (p < 0.0001), shorter durations of catheterization (p < 0.0001), shorter lengths of hospital stay (p < 0.0001) and fewer total complications (p < 0.0001) [Tang et al. 2014].
Comparative studies to bipolar transurethral plasmakinetic prostatectomy (BiTURP)
Yang and colleagues published a comparative study of 158 patients randomized to ThuLEP with a 100W thulium laser and BiTURP, with all patients returning for 18-month follow up. Preoperative parameters were similar in both groups. The authors found that ThuLEP required a significantly longer operative time (65.4 versus 47.4 minutes, p = 0.022) than BiTURP, but resulted in a significantly shorter hospital stay (2.4 versus 4.6 days, p = 0.026), shorter catheterization time (2.1 versus 3.5 days, p = 0.031) and lower drop in hemoglobin (0.15 versus 0.30 g/dl). Similar improvements were seen in IPSS, QoL, Qmax and PVR [Yang et al. 2013]. Short-term and perioperative complications were not mentioned. No patients in any group developed urethral strictures or bladder neck contractures.
Wei and colleagues compared the efficacy and safety of TmLRP using the 120W Tm:YAG laser to BiTURP in patients with prostate size >80 g. A total of 45 patients were randomized to each group and were evaluated at 1, 6, 12 and 18 months. The mean prostate sizes (112.86 ± 28.36 ml TmLRP, 115 ± 39.45 ml BiTURP group) as well as other perioperative parameters were similar in both groups. Compared with the BiTURP group, the TmLRP group had statistically lower hemoglobin drop, shorter catheterization time and shorter hospital stay. Both groups had significant postoperative improvements in IPSS, QoL, Qmax and PVR, with no differences observed between the two groups. Both techniques showed a low perioperative complication rate (TmLRP versus BiTURP: Clavien 1: 13.33 versus 20%; Clavien 2: 0 versus 2.22%; Clavien 3: 0 versus 0%). One patient in the BiTURP group required a blood transfusion perioperatively. Urethral stricture rate was equal (one patient in each group) and one patient in BiTURP group developed a bladder neck contracture. Additionally, there were no significant reduction in IIEF-5 scores during the follow-up period compared with preoperative data and no statistically significant difference was observed between the two groups [Wei et al. 2014].
Peng and colleagues also sought to compare the short-term efficacy and safety of TmLRP with a 100W thulium laser (LISA Laser products OHG, Germany) to BiTURP. A total of 100 patients were randomized to TmLRP or BiTURP. Operative time was significantly longer in the TmLRP group (61 ± 24 versus 30 ± 6 minutes, p < 0.05), while catheterization time (1.8 ± 0.4 versus 3.2 ± 0.6 days, p < 0.05) and hospital stay (3.3 ± 0.8 versus 4.1 ± 1.3 days, p < 0.05) were significantly shorter. No transfusions were required in either group. Significant improvements were seen in both groups in subjective and objective objectives at 1 and 3 months postoperative. Short-term and perioperative complications were not mentioned. Compared with BiTURP, TmLRP was superior in safety, blood loss and urethral stricture rate with similar improvements in IPSS, Qmax and PVR [Peng et al. 2013].
Comparative studies to HoLEP
Zhang and colleagues randomized 133 consecutive patients with BPH to either undergo ThuLEP or HoLEP in order to compare the two techniques. They used a 70W thulium laser system and a 100W holmium laser system and randomized 72 patients to the thulium group and 62 patients to the holmium group. For the ThuLEP and HoLEP groups, mean prostate volume was relatively small and similar (47 ± 25 and 44 ± 23 ml). Operative time was comparatively longer for the ThuLEP group versus the HoLEP group (72.4 versus 61.5 minutes), but resulted in less blood loss (130.0 ml versus 166.6 ml). However, catheterization time and decrease in hemoglobin postoperatively were similar in both groups. The authors concluded that the shorter operative time of the HoLEP may be secondary to the ease of finding the correct capsular plane with the holium:YAG laser. The physical characters of the pulsed holmium:YAG laser include a ‘scar-free’ feature on the prostatic surface with precise incision and dissection simultaneous with coagulation of small and medium-size vessels. Hence, as the incision reaches the surgical capsule, the transitional prostatic lobes burst from this plane to make the enucleation easier. In contrast, the thulium:YAG laser energy is emitted in a continuous wave and induces an ‘eschar-like’ effect on the surface of the incised tissue. Because of worse visualization, a longer time may have been spent to dissect in the correct plane. IPSS, QoL, PVR and PSA were similar in both groups at 1, 6, 12 and 18 months of follow up. No transfusions were required in either group, and no short or long term re-operations were mentioned [Zhang et al. 2012].
Learning curve
Although the outcomes of the Zhang series [Zhang et al. 2012] seem to be similar between the two laser technologies, HoLEP has been shown to demand a great learning curve, with 40–60 cases required to become proficient [Brunckhorst et al. 2015]. Gross and colleagues addressed the learning curve of ThuVEP [Gross et al. 2012] All the 1080 cases were divided into consecutive groups of 216 patients each and complication rates were analyzed in each subgroup. Overall, complication rates decreased significantly over time, with a 41.7% complication rate within the first 216 cases and 19.4% within the last 216 cases (p < 0.001). ThuVEP may have an easier learning curve than HoLEP because the thulium laser allows for instant conversion to vaporization with the same end-fire fiber, a technique that more urologists are comfortable with.
Cost
Currently no comparative cost studies have been performed specifically investigating thulium lasers. However, in 2001, a prospective, randomized trial investigating the cost effectiveness of holmium lasers versus traditional TURP found catheterization time, length of hospital stay, risk of bleeding and incidence of untoward events reduced while offering equivalent outcomes at 1 year postoperatively. In a cost effectiveness analysis, these improvements represented a 24.5% cost saving over TURP [Fraundorfer et al. 2001]. With regard to the thulium laser, acquisition costs are comparable with other laser modalities and the laser fibers cost about €450 each. In contrast to some other laser systems, however, the bare-ended quartz fibers of the thulium laser can be reused many times, which leads to almost negligible running costs [Szlauer et al. 2009].
Conclusion
With reports from around the world, the thulium laser prostatectomy represents a safe and efficacious procedure for benign prostatic obstruction. Multiple techniques including laser resection, vapoenucleation and vaporization have been described and appear to safe and effective with low morbidity. Overall, comparative studies with the traditional TURP, BiTURP, and HoLEP have demonstrated promising, noninferior data in terms of safety and efficacy. Thulium seems to provide better hemostasis, less overall morbidity, shorter catheterization time and a shorter hospital stay compared with the traditional TURP. Also, its option for efficient vaporization in addition to enucleation makes it an easier technology for the average urologist to learn to use than the holmium laser. Finally, due to the physical properties of the laser, thulium laser prostatectomy may theoretically be associated with lower rates of dysuria compared with PVP, although studies are lacking. Further comparative studies are needed to explore this promising and user-friendly technology.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.