
Abstract
Transurethral resection of the prostate (TURP) has remained the procedure of choice for the surgical treatment of bladder outflow obstruction for almost five decades, but holmium laser enucleation of the prostate (HoLEP) is now emerging as a challenger as the gold standard procedure. This review summarizes the evidence base for HoLEP, with particular reference to randomized, controlled (level 1) evidence.
Transurethral resection of the prostate (TURP) has remained the procedure of choice for the surgical treatment of bladder outflow obstruction secondary to benign prostatic enlargement (BPE) for almost five decades [Madersbacher and Marberger, 1999]. However, morbidity after TURP is significant, with reported rates of blood transfusion of approximately 8% [AUA Practice Guidelines Committee, 2003], hyponatraemia in up to 3% [Rassweiler et al. 2006], and a reoperation rate of 1% per year [Madersbacher Prostate Study Group, 2005]. Numerous operations have been developed to improve the outcomes and reduce the morbidity of transurethral prostatic surgery, but most have not stood the test of time, either due to patient dissatisfaction or lack of durability [Gilling et al. 1996].
For a procedure to rival and surpass TURP, it needs to be acceptable both to surgeons and patients. It must have a low complication rate and a low reoperation rate. It should be effective in relieving bladder outflow obstruction and ideally it should be cheap [Chandhoke, 1998].
The holmium laser is a pulsed solid state laser, with a wavelength of 2140 nm. This wavelength is strongly absorbed by water, making it ideal for safe use in an aqueous environment. The tissue effects depend on the energy of the laser beam and its interaction with tissue. For holmium laser enucleation of the prostate (HoLEP), 80–100 W of power are used, and delivered to the prostate using an end-firing bare laser fibre. The effect is precise tissue cutting, with penetration of energy approximately 0.2 mm into prostatic tissue, simultaneous coagulation of blood vessels, and very little thermal spread.
HoLEP was originally developed in Tauranga, New Zealand by Peter Gilling and Mark Fraundorfer [Gilling et al. 1996]. The first prostate procedures performed using the holmium laser were ablation procedures, but the surgeons found the technique unacceptably slow. By replacing a side-firing fibre with an end-firing fibre, the surgeons discovered that it was possible to cut away chips of prostate, so the procedure of holmium laser resection of the prostate evolved. Better still, a whole lobe of prostate could be enucleated along the anatomical plane between the adenoma and the prostatic capsule, similar to the principles used in open Millin’s or transvesical prostatectomy. For this development, a morcellator was required to allow efficient and safe removal of the enucleated prostate from within the bladder [Fraundorfer and Gilling, 1998].
This review aims to evaluate the evidence base for HoLEP, with particular reference to randomized, controlled (level 1A) evidence.
Comparison with transurethral resection of the prostate
There have been five randomized controlled trials comparing HoLEP with conventional TURP (Table 1). The original trial, performed in Tauranga, New Zealand [Tan et al. 2003], involved 61 patients equally randomized into two groups. The study was powered to detect a 10% difference (approximately 5 hours) in hospital stay or catheterization time between the two groups. All patients had bladder outflow obstruction confirmed on preoperative urodynamics, and prostate sizes, measured by transrectal ultrasound, ranged from 40 to 200 ml. Perioperative parameters which were assessed included operative time, catheter time, irrigation requirements, transfusion rate, and resected prostate weight. Patients were followed 1, 3, 6, and 12 months postoperatively, with peak flow rates and American Urological Association (AUA) symptom scores, as well as urodynamics and transrectal ultrasound prostate volumes at 6 months. In summary, HoLEP was superior to TURP in terms of catheter time (mean 17.7 h for HoLEP and 44.9 h for TURP) and hospital stay (27.6 h for HoLEP versus 49.9 h for TURP), but operative times were longer (62.1 min for HoLEP and 33.1 min for TURP). More prostate tissue was removed during HoLEP (mean 40 g versus 24.7 g). Although both procedures were equally effective in improving flow rates and symptom scores with 1-year follow up, HoLEP was superior to TURP in relief of bladder outflow obstruction as proven by urodynamics. This was the first time a transurethral procedure had shown superior urodynamic outcomes compared with TURP (Table 3). Complications of the two procedures were similar (see Table 2), although numbers are small and it is difficult to draw conclusions.
Randomized controlled trials of holmium laser encleation of the prostate (HoLEP) versus transurethral resection of the prostate (TURP).
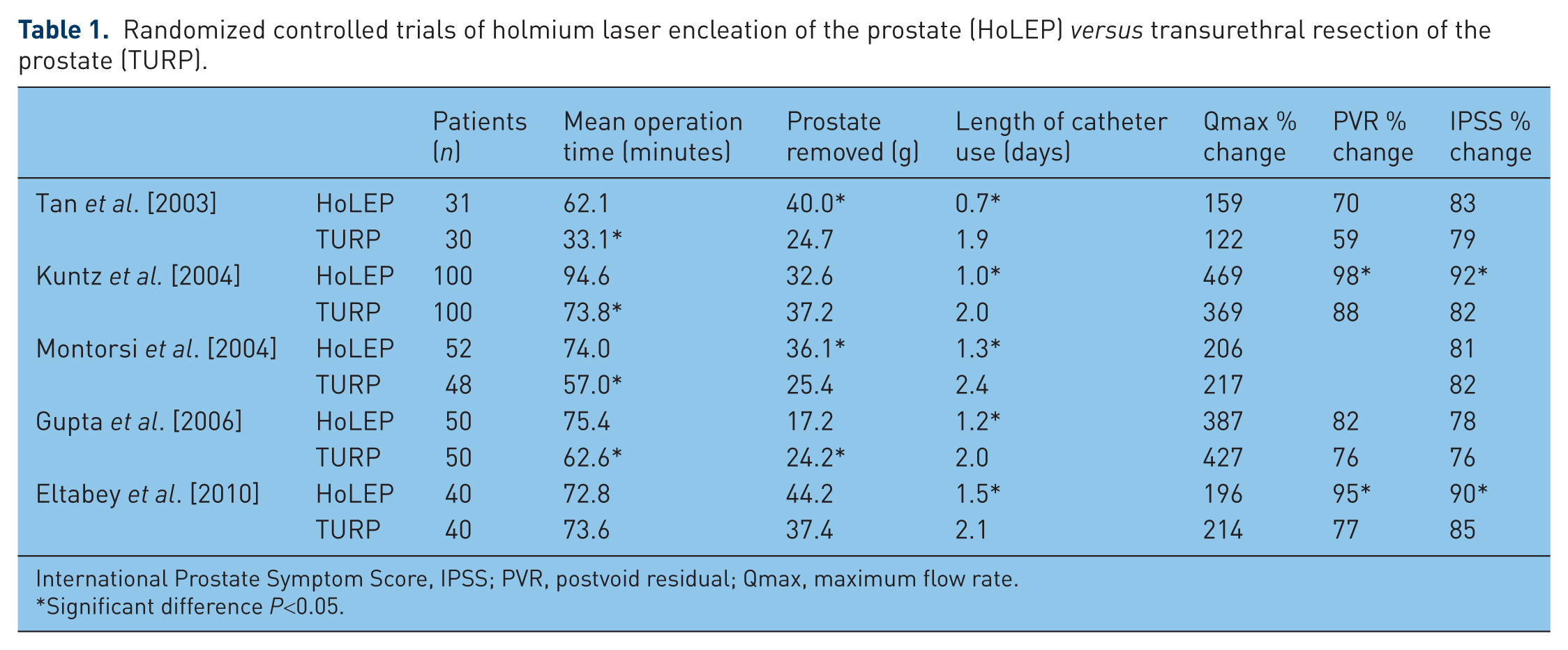
International Prostate Symptom Score, IPSS; PVR, postvoid residual; Qmax, maximum flow rate.
Significant difference P<0.05.
Complications of holmium laser encleation of the prostate (HoLEP) and transurethral resection of the prostate (TURP) [Tan et al. 2003].

Urodynamic findings for holmium laser encleation of the prostate (HoLEP) and transurethral resection of the prostate (TURP).

p < 0.001.
PdetQmax, detrusor pressure at maximal flow rate.
This landmark study was continued and the patients were reassessed at 2-year follow up [Wilson, 2006]. A total of 48 of the original 61 patients were available for assessment and both groups continued to show similar postoperative maximal flow rate (Qmax), AUA and quality of life (QoL) symptom scores. Adverse events were also presented. There was one urethral stricture in the HoLEP group and three in the TURP group. The conclusion from this study was that HoLEP was durable in the medium term.
Further updates were published in 2008 and 2012 [Gilling et al. 2008, 2012]. At 7-year follow up, only 31 patients were available (14 HoLEP and 17 TURP), with 12 deceased and 18 lost to follow up. This illustrates the difficulties in obtaining long-term data in older patients undergoing surgery, even in a location such as New Zealand with a relatively stable population. Nonetheless, of the evaluable patients, there were no differences in flow rates, AUA and QoL scores, benign prostate hyperplasia (BPH) impact scores, international index of erectile function, or International Continence Society Short Form questionnaire (ISC-SF) scores at any time points up to 92 months. There were no reoperations in the HoLEP group and three in the TURP group. The results of this randomized trial confirm that HoLEP is at least equivalent to TURP in the long term, but with a lower reoperation rate.
The medical literature contains many examples of an initial study reporting excellent results, which cannot subsequently be achieved or replicated in other centres. For HoLEP this is not the case. Montorsi and colleagues reported on the first multicentre randomized, controlled trial of HoLEP and TURP, from Bergamo and Milan in Italy [Montorsi et al. 2004]. A total of 100 patients with bladder outflow obstruction proven on urodynamics were randomized to HoLEP or TURP, with follow up continued for 1 year. Patients in the HoLEP group had shorter catheter times and hospital stay, but both procedures were equally effective in relieving obstruction and improving symptoms, with no difference in complications (see Table 3 for urodynamics findings and Table 4 for complications). Similarly, a further randomized, controlled trial of HoLEP and TURP from centres in Berlin, Germany and Cairo, Egypt replicated these findings in a further 200 patients [Kuntz et al. 2004]. A fourth randomized trial from Saudi Arabia [Eltabey et al. 2010] included 80 patients with prostate volumes up to 100 ml. There was no difference in operating times, but HoLEP was again associated with less blood loss, as well as shorter catheter time and hospital stay. HoLEP produced greater improvements in flow rates, AUA scores, and postvoid residual (PVR) volumes. At 1-year follow up, one patient in the HoLEP group developed a urethral stricture compared with two patients in the TURP group.
Early and late adverse events of holmium laser encleation of the prostate (HoLEP) and transurethral resection of the prostate (TURP) [Montorsi et al. 2004].

Gupta and coworkers reported on a randomized controlled trial of HoLEP, standard TURP, and transurethral vapour resection (TUVRP) of the prostate [Gupta et al. 2006]. Fifty patients were included in each group. Both HoLEP and TUVRP showed less blood loss than TURP, and HoLEP had the lowest postoperative irrigation requirements, nursing contact time, and catheter duration. There were no significant differences in IPSS, Qmax, or PVR volumes between the groups.
All of these randomized trials were well designed, with prostate volumes being measured by transrectal ultrasound (TRUS), and using postoperative urodynamics as the most stringent assessment of relief of bladder outflow obstruction. In most, the patient groups included would be similar to the broad case mix faced by practising urologists, although generally patients with prostate cancer and chronic retention were excluded. All contained power calculations to ensure statistical validity, although primary outcome variables selected mostly reflected perioperative variables such as catheter time or length of stay, which might be prone to bias unless the surgeons were blinded to which procedure had been carried out. A consistent finding was that operating time is longer for HoLEP than TURP. However, if the increased volume of tissue removed during HoLEP is taken into account, the procedures in these studies are equally time efficient (0.52 g/min for HoLEP versus 0.57 g/min for TURP) [Ahyai et al. 2010]. Overall, the studies were underpowered to assess for differences in complications between the two procedures, but taken together, very few complications were seen in a total of over 400 patients.
These randomized trials were included in a comprehensive meta-analysis of functional outcomes and complications following transurethral surgery for lower urinary tract symptoms which was published in 2010 [Ahyat et al. 2010]. Twenty-seven randomized, controlled trials of TURP, bipolar TURP, transurethral vaporization of the prostate, HoLEP and KTP laser vaporization were analyzed. The authors used a random effects statistical model and compared combined mean outcomes using forest plots. For HoLEP, four of the previously mentioned randomized trials versus TURP, and two trials versus open prostatectomy were included, with a total of 363 patients. In terms of functional outcomes, HoLEP was the only minimally invasive alternative which showed statistically significant superiority over TURP in both flow rate and IPSS improvements. There was no difference in QoL improvements and postoperative PVR volumes between any of the procedures. In terms of complications, HoLEP had the lowest rate of perioperative complications (5.9% acute retention and only 1.4% reoperation) and showed the lowest rate of postoperative complications.
Comparison with open prostatectomy
The first randomized, controlled trial of HoLEP and open prostatectomy was published in 2002 [Kuntz and Lehrich, 2002]. One hundred and twenty patients with bladder outflow obstruction on urodynamics and prostate volumes greater than 100 ml were randomized to HoLEP or open transvesical prostatectomy. Patients with chronic urinary retention, carcinoma of the prostate, and those with catheters were excluded. At the beginning of the study a morcellator for removal of the enucleated tissue from the bladder was not available, and the ‘mushroom’ technique of leaving the enucleated prostatic lobe attached at the bladder neck by a narrow pedicle and using a standard electrocautery loop to resect the adenoma small enough to be removed [Hochreiter et al. 2002]. This may have skewed the operative times, which were longer overall for HoLEP than open surgery (135.9 min for HoLEP and 90.6 min for open), with similar weight of tissue removed, but all other perioperative parameters favoured HoLEP. Haemoglobin loss, postoperative catheter time, and hospital stay were all significantly better in the HoLEP group. Eight patients in the open group required blood transfusions compared with none in the HoLEP group. There were no differences in AUA scores, peak urinary flow rates, and residual volumes, with 6-month postoperative follow up. Late complications were infrequent, with two bladder neck contractures in the open group, and one stricture in the HoLEP group.
The results of this study were later updated, initially with 18 months of follow up [Kuntz et al. 2004], then with 5-year follow up [Kuntz et al. 2008]. Seventy-four of the original 120 patients completed the 5-year follow-up period. Long-term results were similar in both groups, with mean Qmax of 24.3 ml/s for HoLEP and 24.4 ml/s for open prostatectomy, and mean IPSS scores of 3 in both groups. Both procedures were low in complications, with two urethral strictures for HoLEP compared with one for open, and three bladder neck strictures for open compared with one for HoLEP. The conclusions were that HoLEP was highly effective, suitable for all sizes of prostate, with results durable in the medium term. HoLEP had lower perioperative morbidity and the authors suggested that HoLEP should be considered the new gold standard for surgical treatment of large prostates.
These results were replicated by Naspro and colleagues in a randomized, controlled trial versus open transvesical prostatectomy involving 80 patients, with 2 years of follow up [Naspro et al. 2006]. Again, although operative time was longer for HoLEP (mean 72 min for HoLEP versus 58 min for open), blood transfusion rates, catheterization times, and hospital stay all favoured HoLEP. The transfusion rates in this series were high for open prostatectomy (17.9%) compared with the published literature (6.8–13.3%) [Moody and Lingeman, 2001]. Both groups showed equal urodynamic improvements at 12 months, and there were no differences between the two groups in Qmax or IPSS at any time points up to 2 years. Erectile function, as measured by the International Index of Erectile Function (IIEF) questionnaire, showed no change in baseline in either group. Both groups experienced dysuria (68% in HoLEP group and 41% in open group at 3 months) in the early postoperative period, but this resolved in all but one patient in each group by 2 years. Two patients in each group required reintervention for strictures or bladder neck contracture within the first year of follow up. The authors considered HoLEP to be a safe and minimally invasive alternative to open prostatectomy.
Comparison with bipolar transurethral resection of the prostate
Bipolar resection is emerging as a safer alternative to conventional TURP, avoiding the risks of dilutional hyponatraemia and reducing blood loss [Bhansali et al. 2009]. Proponents of prostate resection would argue that TURP has evolved [Rassweiler et al. 2006] and a more important comparison is with modern bipolar or plasmakinetic resection of the prostate.
Chen and colleagues performed a randomized controlled trial of plasmakinetic resection of the prostate and HoLEP in 280 patients who had previously failed to respond to medical treatment for bladder outflow obstruction [Chen et al. 2013]. Interestingly, the study was powered to show a difference in operating time, which is perhaps not an important outcome variable from a patient perspective. Patients in the HoLEP group had less blood loss, shorter bladder irrigation times, and a reduced hospital stay. There were no significant differences in IPSS, QoL, and Qmax with 2 years of follow up, and there were no differences in complications, erectile function, and retrograde ejaculation. The resection times were similar but operative times were longer for HoLEP, largely due to the additional time for morcellation. The authors commented that the modified enucleation technique described by Gong and colleagues, in which the adenoma is enucleated in an anterior to posterior direction rather than from apex to base, made the procedure easier [Gong et al. 2012], and that the modified morcellation technique of Hwang and colleagues was more efficient and operative times could be further reduced [Hwang et al. 2010]. They preferred the improved intraoperative vision during HoLEP. The authors concluded that HoLEP was superior and proposed that this should be considered the new gold standard operative procedure for BPE.
In contrast, in a second randomized controlled trial of bipolar TURP and HoLEP [Fayed et al. 2011], the conclusions were rather different. The authors randomized only 60 patients with short follow up of 6 months. Although the blood loss, complications, and outcomes were not statistically different between the two groups, they favoured bipolar resection due to the high costs of the holmium laser. They also considered that the resection technique was more familiar to urologists, was easier to master, and avoided the difficulties of the learning curve, and that the equipment for bipolar resection was readily available in most urological theatres.
Comparison with other laser techniques
In recent years, GreenlightTM photoselective vaporisation of the prostate (American Medical System Incorporation, Minnetonka, MN, USA) has gained popularity as an alternative to conventional TURP and it was estimated that in 2005 laser treatment accounted for 57% of total BPH operations in the USA [Yu et al. 2008]. The GreenlightTM laser produces a wavelength of 532 nm, which is fully transmitted through water, but is strongly absorbed by oxygenated haemoglobin. The original GreenlightTM produced 80 W of laser energy but was superseded by the lithium borate (LBO) 120 W Greenlight HPSTM system, which produces faster vaporization of prostate tissue [Wosnitzer and Rutman, 2009]. In 2010 the Greenlight XPSTM was introduced, to provide more power and better ablation efficiency [Malek et al. 2011]. Data are still accumulating, but early results appear promising.
In 2012, Elmansy and coworkers reported the results of the first randomized controlled clinical trial to compare HoLEP with high-performance Greenlight HPSTM in patients with prostates larger than 60 ml [Elmansy et al. 2012]. A total of 80 patients were recruited, with 43 being randomized to HoLEP and 37 to high power photoselective vaporisation (PVP/HPS). Follow up was for 12 months. No statistical differences were observed between the two groups at baseline, with 20% of each group being on anticoagulants or antiplatelet agents. Operative times and catheter times were similar, but 22% of the PVP group were converted intraoperatively to TURP or HoLEP due to failure to control bleeding resulting in poor vision and inadequate tissue removal. A further two PVP cases (5.4%) required retreatment within the study period due to residual adenoma. Overall, therefore, approaching 30% of the PVP cases were unsuccessful on an intention-to-treat basis. In the converted cases, a mean of 46 g of further prostate tissue was removed by HoLEP or TURP. When the converted cases were excluded from the analysis, the improvements in Qmax, PVR, and IPSS favoured HoLEP. Men treated with HoLEP had an 88% decrease in prostate-specific antigen (PSA) compared with only 60% in the PVP group, and postoperative TRUS volumes decreased by 78% for HoLEP and 52% for PVP, suggesting more complete removal of adenoma with HoLEP. Also in support of this assertion, retrograde ejaculation was seen in 88% of the HoLEP group and only 29% of the PVP group, questioning the adequacy of the PVP treatment.
The thulium laser has a similar wavelength of 2013nm, but operates in a continuous wave, and has been shown to be effective for resection, vaporization, and enucleation [Bach et al. 2010]. However, unlike the holmium laser, the thulium laser is ineffective for stone fragmentation, which limits its applications in urology. For prostatic surgery, although both the thulium and holmium lasers have excellent haemostatic properties, there are important differences between the two. The thulium laser produces a more powerful cutting action, but leaves more charring on the tissue surface. With the thulium laser, vision is made more difficult by a stream of bubbles from the fibre tip. One advantage of the thulium laser is that it is cheaper to manufacture.
Zhang and coworkers from Beijing, China published a randomized, controlled trial of thulium laser enucleation of the prostate versus HoLEP [Zhang et al. 2012]. A total of 133 patients were equally randomized to the two groups. Energy settings of 70 W for the thulium laser and 90 W for the holmium laser were used, and the mushroom technique was used for tissue removal. Operative times were significantly longer for the thulium laser (mean 72.4 min versus 61.5 min) but the blood loss was less (130.0 ml versus 166.6 ml). These differences were considered clinically insignificant. After 18 months of follow up there were no differences in QoL scores, IPSS, Qmax, postoperative PSA, or complications between the two groups. The authors concluded that both lasers were equally effective, but they did comment that the holmium laser provided a cleaner and easier plane of dissection between the adenoma and capsule, and the lack of charring made the plane easier to identify. They also concluded that the time for mushroom resection was 17 min, similar to that for morcellation, and the mushroom technique remained a satisfactory option for tissue removal. However, prostate volumes were relatively small in this study (range 34–79 ml).
There has yet to be published a cost comparison between the two lasers. At the current time, the literature evidence is more extensive for the holmium laser than the thulium laser, and so HoLEP should still be considered the gold standard for enucleation. However, as more data become available, this is an interesting area for future developments.
Holmium laser encleation for the large prostate
The randomized, controlled trial data of HoLEP versus open prostatectomy included enucleated prostate weights of up to 200 g [Kuntz and Lehrich, 2002], and suggested that there was no upper size limit for laser enucleation. In a large cases series of 554 patients with prostate volumes up to 350 ml from a single centre in Quebec, Canada [Elzayat et al. 2005], outcomes were found to be independent of prostate size. Similarly, Shah and coworkers stratified outcomes by prostate size in 354 patients undergoing HoLEP [Shah et al. 2008]. The largest prostate was 350 ml, and 42 of the patients had prostate volumes greater than 100 ml on TRUS. Overall, perioperative complications were equally distributed across the groups, and outcomes were independent of prostate size. Operative efficiency was found to increase from 0.36 to 0.58 g/min as prostate size increased. Similar results were obtained in a case series of 573 patients, divided into three groups based on prostate size [Humphreys et al. 2008].
From these studies it can be concluded that there is no upper size limit for HoLEP in experienced hands. This is in contrast to all other endoscopic treatment options for BPE. With the advent of α adrenoreceptor blocker therapy and 5α reductase inhibitor therapy as effective medical treatment of lower urinary tract symptoms, prostatic surgery is often delayed, and prostate sizes in operative series have increased over the last three decades [Rassweiller et al. 2006]. The suitability of HoLEP in all sizes of prostate may prove to be a most desirable advantage as life expectancy increases and prostatic surgery is performed at a later stage in the natural history of the disease.
Holmium laser encleation of the prostate for acute urinary retention
Acute urinary retention is the primary indication for surgery in up to 46% of cases [Pickard et al. 1998], so it is clearly important that a procedure is effective in this setting. These patients present a particular challenge, as outcomes for TURP have been shown to be inferior and complications rates greater than patients without retention. In the UK National Prostatectomy Audit [Pickard et al. 1998], rate of postoperative failure to void was 9.2% compared with 2.4% in those without retention. Perioperative morbidity, catheter times, and hospital stay were increased in the retention group, largely due to increased bleeding complications. In a large multicentre trial of 3885 patients undergoing TURP [Mebust et al. 2002] the urinary infection rate was three times greater in the acute retention group.
Peterson and coworkers from Indianapolis, Indiana, USA reported on a cohort of 164 consecutive patients who underwent HoLEP for acute urinary retention [Peterson et al. 2005]. Although the mean duration of preoperative catheterization was 29 days, some patients had a catheter for up to a year. Prostate volumes in this cohort were very large, mean preoperative prostate size being measured as 107 ml on transrectal ultrasound. All patients were catheter free within 10 days postoperatively, although two patients needed temporary recatheterization within 3 months for haematuria and clot retention. The complication rate was very low, with only seven patients requiring antibiotics for urinary infection and 12 patients having temporary stress incontinence requiring the use of pads at 1-month follow up. At 6 months, one further patient required temporary catheterization for haematuria, there were three further urinary infections, and one patient needed reoperation for urethral stricture. Stress incontinence had resolved in most patients, although five patients were still using pads at this time point. Unfortunately the dropout rate of patients lost to follow up then became significant, with only 38 of the patients being evaluated at 1 year. One patient required urethral dilatation, one developed epididymitis, and only one patient still required pads for stress incontinence.
Although this study is not randomized, these excellent results support the use of HoLEP in this high-risk patient group. Increased incidence of complications compared with the elective setting were not seen, perhaps due to the excellent haemostatic properties of the holmium laser, the avoidance of irrigant absorption and dilutional hyponatraemia, and the completeness of removal of the adenoma.
Analysis of the learning curve
It is often perceived that HoLEP is a difficult procedure, and this may have hampered its widespread acceptance. In the original paper by from Tan and colleagues, the authors commented that approximately 20 or 30 procedures were necessary to achieve consistent and reproducible results in medium sized (50 ml) prostates [Tan et al. 2003]. They considered this to be similar to that required for urological trainees to learn TURP, but the better visibility due to less bleeding in HoLEP was advantageous. The use of the morcellator has also been considered dangerous due to an incidence of bladder mucosal injury of up to 18% in early series [Montorsi et al. 2004]. However, this complication has now virtually been eliminated with a simple modification of the surgical technique, using double irrigation, which helps to keep the bladder full throughout and keeps the bladder mucosa well away from the morcellator blades.
The learning curve for HoLEP was critically examined by El Hakim and Elhilali [El Hakim and Elhilali, 2002]. In this study, 27 patients were treated using HoLEP performed by a senior resident, under the supervision of an experienced HoLEP surgeon. Each of the 27 procedures was recorded and reviewed, and compared with 118 patients who underwent HoLEP by the supervising urologist. For the first 15 patients, the resident performed on average 85% of the operation and the attending staff intervened whenever difficulty arose. The two most difficult technical steps identified were the initial apical enucleation, and the incision of the remaining anteroapical mucosal attachment of the lateral lobes. The last 12 patients were managed completely by the resident with no intervention from the staff urologist. There was no difference in operative time or other operative variables between the first 15 and next 12 patients, or any difference in postoperative outcomes or complications when compared with the patients treated by the experienced surgeon. The authors concluded that although HoLEP is technically more challenging than TURP, by using a modular operative technique, with close supervision and feedback from an experienced surgeon, the trainee can become confident with the procedure after 10–15 cases.
In a retrospective review of 70 patients who underwent HoLEP [Seki et al. 2003], the ratio of improvement in the preoperative to postoperative urinary flow rate, PVR urine, IPSS, and QoL index did not change significantly as experience increased, indicating that good results can be obtained early in the learning curve. However, the efficiency of enucleation increased significantly as experience increased. There were two morcellator bladder injuries in this series.
In conclusion, the published literature suggests that good clinical results can generally be achieved within 20 cases. In the UK there is a structured training and mentoring programme, which includes HoLEP courses and masterclasses, as well as HoLEP simulation on a realistic prostate model. This has led to more widespread uptake than in other countries and with support the learning curve has been shortened [Kastner et al. 2010]. Trainees often find HoLEP easier than TURP due to improved intraoperative vision from reduced bleeding, so the long learning curve for HoLEP appears to be largely a myth [Ahmed et al. 2010].
Costs analysis
The financial outlay required to set up HoLEP is potentially a barrier to increased uptake of the technique. Fraundorfer and colleagues assessed the costs associated with holmium laser resection of the prostate (HoLRP) and TURP [Fraundorfer et al. 2001]. They concluded that the operative time was longer for HoLRP than TURP, which incurred additional costs, but because HoLRP was superior with respect to catheterization time, nursing contact time, hospital stay, and blood transfusion rate, inpatient hospital costs were cheaper overall. Cost analysis showed HoLRP to be 24.5% cheaper per case, which would equate in this financial model to 93 cases per year being required to cover the costs of laser machine purchase and maintenance within 5 years.
However, it is management of complications which has the greatest impact on procedure cost, particularly if another surgical procedure is required. In the Fraundorfer study, eight HoLRP patients made 12 unscheduled clinic visits and 12 TURP patients made 16 unscheduled visits. Seven TURP patients required readmission during the first year for clot retention (n = 1), deep vein thrombosis (n = 1), bladder neck incision (n = 3), and repeat surgery (n = 2); three HoLRP patients were admitted with retention (n = 2) and for bladder neck incision (n = 1). The total costs of managing complications were 40% less for HoLRP than TURP.
In a comparison of the inpatient costs of HoLEP and open prostatectomy [Salonia et al. 2006], operative time was 16.1% of the total cost for open prostatectomy and 25.1% of the total for HoLEP; theatre disposables were 13.3% of the total for open compared with 29.3% for HoLEP; but hospital stay was the largest factor, with this contributing 53.3% of the total for open and 32% for HoLEP. Overall, HoLEP was 9.6% cheaper than open prostatectomy.
Lourenco and colleagues reported on a systematic review of the effectiveness and cost utility of surgical treatment for men with BPE [Lourenco et al. 2008]. They used a Markov model, which assesses total costs based on likely care pathways. They concluded that HoLEP was more cost effective than a single TURP, but less effective than a strategy involving repeat TURP if required. Overall TURP remained the most clinically effective and cost effective.
One of the problems with cost analysis is that the relevance to different healthcare systems can be limited, as hospital costs and reimbursement varies significantly in different countries. The true costs of theatre time and hospital stay are difficult to quantify, and the results of such studies depend heavily on the financial model used. None of these studies address the potential for increased income if operating time is saved, allowing an extra procedure to be performed and resulting in increased income. Also many of the postoperative costs are fixed and so shorter hospital stay does not necessarily result in financial savings to a hospital, unless availability of hospital beds is a limiting factor for operative activity.
In contrast to GreenlightTM photoselective vaporisation laser ablation of the prostate in which a single use side-firing fibre is used, the laser fibres for HoLEP are reusable, and each fibre can be used for upwards of 20 cases. Therefore, although the purchase cost of the holmium laser is high, the running costs are low.
Holmium laser encleation of the prostate combined with other procedures
The clinical efficacy of the holmium laser for fragmentation of urinary tract stones is well established and it is no surprise that HoLEP combined with laser cystolitholapaxy for bladder stones [Shah et al. 2007] or HoLEP combined with ureteroscopy and laser stone fragmentation is effective, feasible, and safe [Kim et al. 2004]. Other reported combinations in the literature include sequential HoLEP with laparoscopic bladder diverticulectomy [Shah et al. 2006], percutaneous nephrolithotomy and insertion and removal of ureteric stents [Kim et al. 2004]. Laparoscopic radical prostatectomy can also be readily performed after HoLEP [Suardi et al. 2008].
Other energy sources for enucleation
From a theoretical standpoint, the ideal energy source for enucleation of the prostate would be one producing a precise cutting effect, with simultaneous coagulation of blood vessels and no thermal spread to minimize the effects on adjacent structures, such as the erectile nerves which are closely related to the apex of the prostate. The holmium laser wavelength has all of these desirable properties, with the added advantage of the energy being strongly absorbed by water which provides inherent safety. However, several studies have investigated the potential for replicating the enucleation technique using other energy sources.
The technique of plasmakinetic enucleation of the prostate (PKEP) was described by Neill and coworkers, in which a bipolar electrode (Gyrus Plasmakinetic System, Gyrus Medical, Cardiff, UK) was used to enter the anatomical plane between the adenoma and capsule, then blunt dissection with bipolar haemostasis was used to complete the enucleation [Neill et al. 2006]. In this study the morcellator was then used. Twenty patients were randomized to each treatment, the primary outcome variable being selected as catheter time, as this reflects the degree of postoperative haemorrhage and is a parameter which is important to patients as is the main determinant of hospital stay. The study was powered to detect a 30% difference between the two procedures. In conclusion, plasmakinetic enucleation was shown to be safe and effective, but operation time (43.6 min for HoLEP versus 60.5 min for PKEP), recovery room time (47.1 min versus 65.5 min for PKEP) and irrigation use (5% for HoLEP, 35% for PKEP) all favoured HoLEP. Adverse events and functional outcomes were similar, with a year of follow up, although the study was designed to primarily examine the perioperative variables rather than longer-term outcomes. Despite the longer irrigation time, there were no differences in catheter time, hospital time, or blood transfusions, so the clinical significance of these differences is debatable. Although a cost comparison was not included, the implication was that the Gyrus enucleation was cheaper due to lower capital costs of the equipment, although clearly the Gyrus system is less versatile and cannot be used for stones. The surgeons in this study were experienced in prostate enucleation and they considered PKEP to be more difficult than HoLEP, partly due to inferior haemostatic properties but also partly because of bubbles at the point of activation of the Gyrus device obscuring vision and requiring more frequent stopping and checking of the position of the capsular plane. From this study the authors concluded that the best energy source for enucleation remained the holmium laser, although bipolar enucleation could be considered as a cheaper alternative for those skilled in the enucleation technique.
In a randomized, controlled trial comparing PKEP to TURP by Zhao and colleagues, the prostatic adenoma was separated from the sphincter using the bipolar loop, then enucleated in antegrade fashion largely by blunt dissection, then cut into chips, similar to the ‘mushroom’ technique [Zhao et al. 2010]. Prostate sizes of up to 150 ml were included and postoperative follow up continued for 3 years. There were no differences in operative time but significantly reduced blood loss, irrigation requirements, catheter time, and hospital stay in the PKEP group. At 36 months, PKEP patients had significantly better flow rates and lower voiding pressures on urodynamics than TURP patients, with no differences in sexual function between the groups. From this study, the conclusion was that PKEP outcomes compared favourably with TURP. This study provides further evidence that endoscopic enucleation techniques are superior to resection techniques and more complete removal of the prostatic adenoma leads to better outcomes.
There remains insufficient evidence to support plasmakinetic enucleation over holmium enucleation, although from a theoretical standpoint the precision of the tissue effect and no thermal spread from the holmium has advantages over electrocautery. It remains to be seen whether these advantages are important clinically.
Conclusion
There have been many procedures which have been proposed as alternatives to TURP for the surgical treatment of men with bladder outflow obstruction secondary to BPE. The ideal procedure is one which is minimally invasive, associated with low perioperative morbidity, effective in relieving obstruction and improving symptoms, has a low complication rate, and is durable in the long term. The evidence base in support of HoLEP is more extensive than that for any other minimally invasive alternative to TURP, with over 400 patients enrolled in published prospective randomized clinical trials. It is now well established that HoLEP is superior to TURP in the perioperative period and symptom improvement is at least as good as TURP. The complication and reoperation rates appear lower and durability has been confirmed over 10 years of follow up. It would appear therefore that HoLEP achieves all the goals of the ideal procedure.
The European Association of Urology published guidelines on laser surgery in 2012 [EAU Guidelines panel on Laser Technologies, Herrmann et al. 2012]. The recommendations were that HoLEP is an alternative to TURP and can be offered to any patient with bladder outflow obstruction secondary to benign prostatic enlargement (BPE), with the highest level of evidence (level 1a) and the highest grade of recommendation (grade A). They also concluded that HoLEP can be offered to patients with chronic urinary retention (level 2b, grade B), and in patients on anticoagulants or antiplatelet medication (level 2b, grade B).
The HoLEP procedure has now passed the tests of feasibility, safety, efficacy, and durability, and is a strong contender for the new reference standard for endoscopic BPH surgery. For HoLEP, the next challenge is its wider clinical application outside of experienced centres, ideally under the mentorship of established HoLEP surgeons to generally shorten the learning curve.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
Mark Cynk is a meeting participant for Lumenis, Inc.