
Abstract
The increased use of abdominal imaging has led to identification of more patients with incidental renal masses, and renal mass biopsy (RMB) has become a popular method to evaluate unknown renal masses prior to definitive treatment. Pathologic data obtained from biopsy may be used to guide decisions for treatment and may include the presence or absence of malignant tumor, renal cell cancer subtype, tumor grade and the presence of other aggressive pathologic features. However, prior to using RMB for risk stratification, it is important to understand whether RMB findings are equivalent to pathologic analysis of surgical specimens and to identify any potential limitations of this approach. This review outlines the advantages and limitations of the current studies that evaluate RMB as a guide for treatment decision in patients with unknown renal masses.
In multiple series, RMB has demonstrated low morbidity and a theoretical reduction in cost, if patients with benign tumors are identified from biopsy and can avoid subsequent treatment. However, when considering the routine use of RMB for risk stratification, it is important to note that biopsy may underestimate risk in some patients by undergrading, understaging or failing to identify aggressive tumor features. Future studies should focus on developing treatment algorithms that integrate RMB to identify the optimal use in risk stratification of patients with unknown renal masses.
Introduction
The incidence and detection of renal cell carcinoma (RCC) has increased significantly over the past 50 years [Pantuck et al. 2001]. Improvements in cross-sectional imaging techniques have facilitated detection of asymptomatic small renal masses (SRMs) while causing a stage migration in RCC [Hollingsworth et al. 2006] with masses up to 4 cm constituting 48–66% of new diagnoses [Nguyen et al. 2006]. The etiology of unknown renal masses falls into three categories: aggressive cancers, slow-growing cancers and benign tumors [Frank et al. 2003] and treatment of renal tumors may include surgery, ablation or active surveillance. However, deciding among treatments is not always straightforward, especially for patients with major comorbidities or advanced age [Patel et al. 2012]. Many small RCCs are indolent with less than 5% of patients with nonmetastatic SRMs progressing to metastatic RCCs (mRCCs) within the first 5 years after treatment [Abel et al. 2010b; Umbreit et al. 2012]. However, while the probability of developing mRCC is small, the consequences are significant because the prognosis for patients with RCC with metastases is dismal despite treatment with newer systemic agents [Heng et al. 2009]. Therefore, identifying aggressive tumors is critical to proper treatment, while the identification of more indolent tumors is also useful for selecting patients who may benefit from alternative approaches to treatment such as surveillance regimens.
Renal mass biopsy (RMB) has become a popular diagnostic tool to evaluate renal masses and may provide important information prior to treatment [Volpe et al. 2007]. However, RMB should be compared with the gold standard for risk assessment in patients with nonmetastatic disease, which is based on pathologic evaluation of renal tumor specimens after surgery. Multiple pathologic predictors for metastatic recurrence and cancer-specific survival have been described and validated, including nuclear grade, T stage and the presence of poor prognostic features such as sarcomatoid differentiation [Zisman et al. 2002; Sorbellini et al. 2005; Thompson et al. 2007; Abel et al. 2010b]. While percutaneous biopsy and three-dimensional imaging provide predictive data, it is unclear if information gained prior to surgery is equivalent to the pathologic assessment after surgery. The purpose of this review is to outline the data supporting and limiting the use of RMB for risk stratification in patients with renal masses.
Rationale for renal mass biopsy
Historically, patients diagnosed with renal masses would be treated with surgery and pathologic diagnosis would be made afterward from nephrectomy specimens. The rationale for surgery was the presumptive diagnosis of RCC since it is found in the majority of patients with incidental renal masses in surgical series [Frank et al. 2003]. However, the increased use of imaging has led to more frequent diagnosis of small incidental renal masses in patients who are often being treated for other cancers or serious medical comorbidities [Umbreit et al. 2012]. Deciding the best treatment for patients with renal masses can be especially difficult when considering possible competing causes of mortality for many patients [Kutikov et al. 2010]. In addition, alternatives to surgery such as thermal ablation [Choueiri et al. 2011] and active surveillance protocols [Smaldone et al. 2013] have been developed and may be more appropriate treatments for patients with serious comorbidities. As a result, RMB has become popular method for identifying renal malignancies prior to treatment [Leppert et al. 2014].
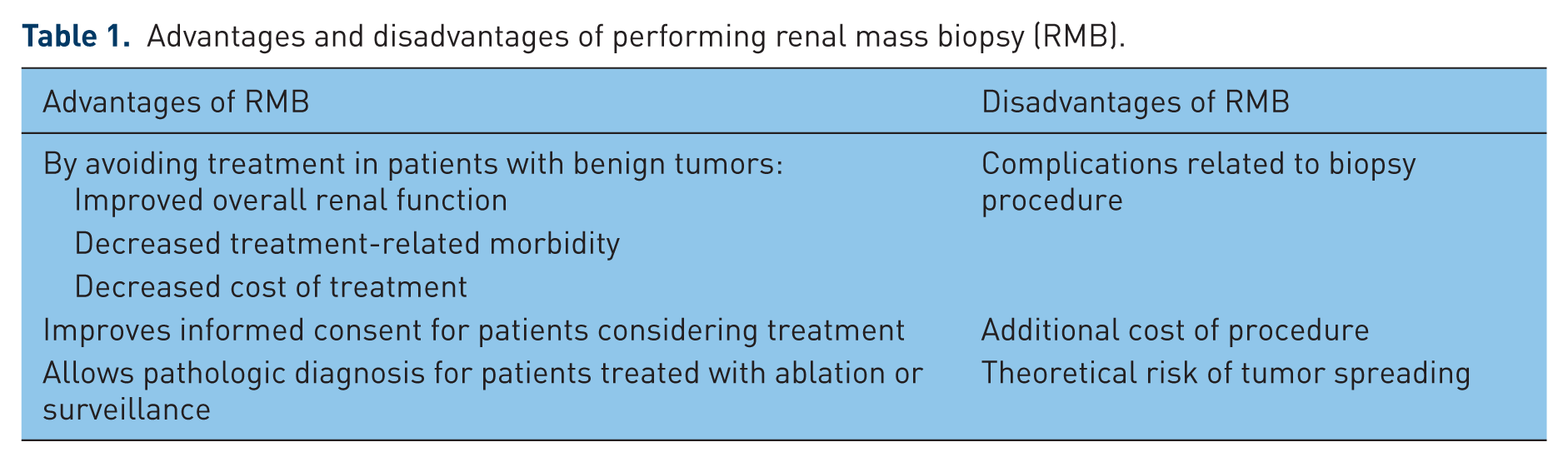
The optimal use of RMB for patients with incidental renal masses is debated and the proper role of biopsy for the evaluation of patients with typical renal mass remains unclear. Although there are theoretical advantages and disadvantages with the use of RMB (Table 1), the choice to obtain a biopsy should be made individually based on the perceived risks and benefits for each patient. Similar to any diagnostic test, a thorough understanding of the ability and limitations of RMB is essential for physicians treating patients with renal masses. Risk stratification for treatment planning should be comprehensive considering patient comorbidities, data from RMB and imaging, as well the potential for inaccuracy when using these techniques. Depending on the institutional practice, pathological information reported from biopsy specimens may include the presence of neoplasm, tumor grade, histologic subtype, and the presence of aggressive features, for example, sarcomatoid or rhabdoid features. The ability of RMB to accurately diagnose these features will be examined individually.
Advantages and disadvantages of performing renal mass biopsy (RMB).
Renal mass biopsy: safety and cost
It is appropriate to first consider the safety and cost of RMB prior to assessing its clinical utility. Potential complications of RMB include retroperitoneal hemorrhage, vascular complications, pneumothorax or biopsy tract seeding. However, the overall rates of post biopsy complications are low [Lane et al. 2008; Volpe et al. 2012] and complications requiring intervention are seen in less than 1% of patients from large modern series [Prince et al. 2014]. The most common complication following biopsy is bleeding from nearby vascular structures, the kidney parenchyma or the tumor itself. As biopsy techniques have evolved, the risk of significant hemorrhage has decreased [Caoili et al. 2002; Rybicki et al. 2003]. Similarly, the development of arteriovenous fistula or pneumothorax occurs in less than 1% of patients following biopsy [Leveridge et al. 2011]. One exceptionally rare complication which receives disproportionate attention is the possibility of biopsy tumor tract seeding. This complication has been reported in the literature twice in the last 20 years [Leveridge et al. 2011; Mullins and Rodriguez, 2013], despite a significant increase in the utilization of RMB over the same time period [Leppert et al. 2014].
Another concern when integrating biopsy into patient management of renal masses is the additional cost of undergoing a biopsy when surgery achieves both diagnosis and treatment objectives. However, if patients with benign tumors are spared the cost of treatment, biopsy may be cost effective. To address the cost effectiveness of RMB, Pandharipande and colleagues used a decision-analytic Markhov model to compare cost effectiveness of using RMB to triage patient management to surveillance or empiric surgery for SRMs [Pandharipande et al. 2010]. They found that a biopsy strategy yielded a minimally improved quality-adjusted life expectancy of 4 days compared with surgery at a lower lifetime cost of $3466. In similar fashion, while again using a Markhov model, a more recent report compared immediate surgery with biopsy or surveillance in a hypothetical 60-year-old man with a SRM. When adjusting for quality of life, biopsy outperformed immediate surgery as a more cost-effective diagnostic strategy at $33,840 per quality-adjusted life year gained [Heilbrun et al. 2012]. Although biopsy did not yield the best survival, this study highlights that low-risk patients may be treated with surveillance for a T1a renal mass while benefiting from a cost-effective strategy.
Ability of renal mass biopsy to diagnose the presence of malignancy
The accuracy of RMB to diagnose malignancy depends on multiple factors, including the ability to target small tumors using imaging guidance, the ability to diagnose malignancy from small pathologic specimens, and the inherent sampling error when evaluating heterogeneous tumors. Although no prospective studies have evaluated fine needle aspiration (FNA) versus core biopsy techniques for accuracy, it should be noted that diagnoses from FNA sampling are considerably dependent on the experience of the cytopathologist, who may be present at the biopsy to confirm the adequacy of sampling [Volpe et al. 2007]. Nondiagnostic findings from RMB are present in 15–22% of large contemporary series [Shannon et al. 2008; Leveridge et al. 2011; Prince et al. 2014] (Table 2). Some of the variation in incidence among series stems from the lack of a standardized definition for nondiagnostic RMB. Many series report only fibrosis or necrosis as nondiagnostic findings while other series include RMB with benign renal parenchyma when the tumor was ‘missed’. Nondiagnostic findings appear to be more common in patients with smaller tumors [Wang et al. 2009; Leveridge et al. 2011; Prince et al. 2014] and cystic features [Leveridge et al. 2011; Prince et al. 2014]. In addition, a longer distance from the skin to the tumor and a lack of enhancement with contrast imaging may also be associated with higher nondiagnostic rates [Prince et al. 2014]. Patient and tumor characteristics should be considered when deciding to obtain RMB, and lower overall nondiagnostic rates may be possible when selecting only patients with larger solid enhancing masses and shorter skin to tumor distance. When RMB is not diagnostic for either infection or a neoplasm, physicians should still suspect the presence of malignancy and consider repeating biopsy or proceeding with surgery or observation as indicated. However, there is minimal impact on risk stratification when physicians understand the continued risk of malignancy in patients with incidental renal masses and nondiagnostic RMB.
Renal mass biopsy series and nondiagnostic rate.

Ability of renal mass biopsy to diagnose renal cell cancer subtypes
Prior studies evaluating the concordance between biopsy specimens and surgical pathology for RCC subtype have ranged between 86% and 100% (Table 3) [Shannon et al. 2008; Wang et al. 2009; Millet et al. 2012]. High levels of concordance between biopsy and surgical pathology are especially noted in clear cell or conventional RCC [Shannon et al. 2008], which is the most common subtype of RCC [Lane et al. 2008]. Recent studies of non-clear cell RCC subtypes have also demonstrated high rates of concordance [Millet et al. 2012], with immunohistochemical staining facilitating diagnosis in some patients [Lane et al. 2008].
Studies comparing renal mass biopsy to surgical pathology.

One important diagnostic consideration is the ability to differentiate between chromophobe RCC and oncocytoma, which may be achieved using a panel of tissue markers [Huang et al. 2009]. Historically, there was significant concern over the ability to distinguish oncocytoma from RCC both histologically and radiographically [Gakis et al. 2011] and surgical resection remained the only modality to diagnose and treat oncocytoma. Concern for hybrid tumors consisting of oncocytoma juxtaposed with malignant tissue [Waldert et al. 2010] caused many surgeons to recommend treatment for all patients despite a biopsy diagnosis of oncocytoma. However, recent series have suggested that hybrid tumors are exceptionally rare. Ginzburg and colleagues identified 147 solitary sporadic tumors that contained any element of oncocytoma or angiomyolipoma following nephrectomy [Ginzburg et al. 2014] and found less than 3% of tumors included coexistent malignant tissue, with no tumors having any high-grade components. Importantly, at a median follow up of 44 months, no patient with a hybrid tumor experienced local, regional or metastatic progression. These results are encouraging and support less aggressive approaches for renal oncocytoma management.
Ability of renal mass biopsy to evaluate tumor grade in renal cell carcinoma
Tumor grade is often a reliable determinant of tumor behavior [Ficarra et al. 2010]. However, with recent studies demonstrating considerable tumor heterogeneity within RCC tumors, biopsy grade may be less accurate due to sampling error [Gerlinger et al. 2012]. To evaluate the possibility that tumor heterogeneity can lead to misrepresentation of biopsy grade, Ball and colleagues reevaluated 32 pT1a RCC surgical specimens for grade heterogeneity. Specimens consisted of either clear cell or papillary RCC with high- and low-grade features. The authors showed that 26 samples (81.3%) were heterogeneous and 15 of 16 high-grade tumors also exhibited significant low-grade components [Ball et al. 2015]. With significant grade heterogeneity demonstrated among high-grade cancers, it is obvious how biopsy sampling may miss a component of high-grade disease and underestimate RCC risk. Previous series substantiate the inaccuracy of predicting tumor grade from biopsy specimens [Neuzillet et al. 2004; Lebret et al. 2007; Millet et al. 2012], which has implications for reporting and interpreting RMB results. A recent report identified grade heterogeneity in single tumors in up to 25% of cases [Halverson et al. 2013]. Undergrading biopsy specimens could be significant clinically for some patients if they choose to defer treatment based on risk assessment from an erroneous tumor grade. The accuracy of tumor grading on RMB specimens varies considerably among series (43–75%) [Tomaszewski et al. 2014], and no studies included more than 100 patients. Although high-grade tumors are rare in small localized tumors [Abel et al. 2010b], the limited ability to predict tumor grade must be considered when making treatment decisions.
Ability of preoperative imaging to evaluate tumor stage in small renal cell carcinoma
Radiologic imaging may be used to evaluate the clinical T stage of the primary tumor, which is an important predictor of RCC recurrence and survival [Zisman et al. 2002; Sorbellini et al. 2005; Thompson et al. 2007], although clinical staging is not equivalent to pathologic staging in RCC. Renal masses equal to or less than 7 cm are staged as T1 or T3a when tumors invade into perinephric fat. However, imaging does not reliably identify perinephric fat invasion [Hedgire et al. 2013], which is an important predictor of poor outcomes in RCC. In a recent study of 860 patients with RCC stage T1–3 [Yoo et al. 2008], the authors showed a significant difference in disease-free survival [hazard ratio 2.21, 95% confidence interval (CI) 1.01–4.84; p = 0.05] among patients with fat invasion compared with lower stage disease. Furthermore, 85% of patients with recurrence of T3a tumors greater than 7 cm died of RCC compared with 33% of patients who had recurrence with tumors less than 7 cm (p = 0.001). When evaluating patients with tumors less than 7 cm specifically, metastatic recurrence was 14.6% compared with 6.0% in patients with fat invasion and without fat invasion, respectively [Ginzburg et al. 2014]. Siddiqui and colleagues also evaluated the significance of T3a disease across a spectrum of tumor size and found risk ratios of death for RCC fat invasion to be 6.15 (1.84–20.50, p = 0.003), 4.12 (2.50–6.78, p < 0.001) and 2.13 (1.53–2.97, p < 0.001) for tumors 4 cm or smaller, 4–7 cm, and more than 7 cm, respectively [Siddiqui et al. 2007]. The association of death with fat invasion remained significant on multivariate analysis. Attempts to identify T3a tumors based on preoperative imaging have demonstrated poor accuracy [Sokhi et al. 2015]. A recent study compared a combined approach of computed tomography/magnetic resonance imaging with nephrectomy assessment for perinephric fat invasion in renal masses with median diameter of 4.5 cm. Of 55 patients who were diagnosed with fat invasion, 26 (47.2%) did not have pathological fat invasion [Huang et al. 2009]. Likewise, detection of renal sinus fat invasion may carry equal importance as these tumors have been shown to be more aggressive than tumors with perinephric fat involvement [Thompson et al. 2005]. Unless more reliable methods for detecting perinephric fat and renal sinus fat invasion [Kim et al. 2014] are developed, understaging will likely remain a persistent limitation for approximately 5–10% of patients with clinically localized tumors that are pathologically T3a [Siddiqui et al. 2007; Gorin et al. 2013].
Ability of biopsy to identify aggressive pathologic features in small renal masses
Sarcomatoid dedifferentiation is an aggressive pathologic feature that may be present with any RCC subtype [Lane et al. 2008] and is associated with poor outcomes [Zhang et al. 2014]. However, the ability of percutaneous biopsy to identify sarcomatoid features may be limited by sampling error. In patients with mRCC, sarcomatoid dedifferentiation was identified preoperatively in only 11.8% and 9.2% of primary tumors and metastatic tumors, respectively [Chao et al. 2001; Crispen et al. 2011]. As seen with high tumor grade [Ball et al. 2015], sarcomatoid dedifferentiation may only be present in a minority of tissue and percutaneous biopsy is therefore prone to sampling error. However, sarcomatoid pathology is rare in lower stage tumors, with one study of 925 patients with pT1 and pT2 tumors demonstrating less than 1% incidence of sarcomatoid features in the surgical specimens [Abel et al. 2010b]. Given the rarity in low-stage tumors, the inability to identify sarcomatoid features from biopsy is likely less significant for this population.
Should the limitations of biopsy limit its use for risk stratification of incidental renal masses?
There are notable limitations (Table 4) when using RMB that may result in underestimation of risk in patients with nonmetastatic disease and incidental renal masses. These limitations should be considered when ordering RMB for healthy patients considering surgical treatment, because of the risk of mRCC. However, the potential benefits of RMB for many patients should not be dismissed regardless of RMB limitations. Biopsy is safe and likely cost efficient when used judiciously and has demonstrated the ability to reliably identify malignant and benign tumors in patients with incidental renal masses. For many patients with incidental renal masses, RMB can provide information that is helpful for management.
Potential limitations when using renal mass biopsy for estimating risk from incidental renal masses.

Patient selection for renal mass biopsy
Selecting appropriate patients for RMB is important to improve the evaluation of incidental renal masses and maximize the percentage of patients who benefit from this procedure. Patients who are considering active surveillance or thermal ablation should receive RMB in order to plan appropriate follow-up protocols [Volpe et al.2012]. When benign masses are identified, patients may receive minimal follow up as appropriate. Similarly, in patients who are borderline candidates for surgery, the identification of benign masses allows surgery to be deferred. However, in patients with comorbidities that significantly limit a patient’s life expectancy, RMB should only be ordered when the information gained from RMB may change the patient’s further treatment.
Patients with atypical renal masses that are concerning for infection or metastatic lesions are ideal patients for RMB. In addition, very young patients or those with masses that are suspicious for non-RCC lesions may benefit from identification of malignancy, as treatment for some tumors such as renal lymphomas [Cyriac et al.2010] or sarcomas [De Visschere et al.2013] may involve upfront chemotherapy or radiation therapy. Deciding which patients should receive RMB among patients who are otherwise acceptable surgical candidates is less clear. However, RMB does improve informed consent for patients who are considering surgical treatment for their renal masses. When patients are given the diagnosis of cancer from RMB, they may be more willing to be treated with surgical therapy. Conversely, patients with benign masses identified from RMB may be more willing to undergo observation.
Patients who are suspected of having metastatic renal masses may also obtain RMB for diagnosis, especially as the majority of patients with mRCC are not treated with cytoreductive nephrectomy [Tsao et al. 2012; Minnillo et al. 2014], but need a pathologic diagnosis prior to treatment. Despite the development of multiple new therapies, patients with mRCC continue to have a poor prognosis [Heng et al. 2009]. Aggressive features such as sarcomatoid dedifferentiation are associated with short overall survival and may not benefit from cytoreductive surgery [Mian et al. 2002; Molina et al. 2011; Przybycin et al. 2014]. An analysis of 417 patients undergoing cytoreductive nephrectomy for mRCC compared those with sarcomatoid histology with conventional RCC [Shuch et al. 2009]. Median survival in patients with sarcomatoid features was just 4.9 months compared with 17.7 months for conventional clear cell RCC (p < 0.001). However, sarcomatoid features are difficult to identify because of sampling error in large tumors or metastases using standard biopsy techniques [Abel et al. 2010a, 2012]. Similarly, distinguishing non-clear cell tumor subtypes may be helpful as targeted therapy appear to be less effective [Vera-Badillo et al. 2014]. In a meta-analysis consisting of 49 studies and 7771 patients treated with targeted therapy for mRCC, the median progression-free survival and overall survival for non-clear cell RCC was 7.4 and 13.4 months, respectively, compared with 10.5 and 15.7 months for clear cell RCC, respectively (p < 0.001). While cytoreductive nephrectomy may provide a survival benefit in metastatic non-clear cell RCC [Aizer et al. 2014], preoperative identification of non-clear cell RCC from RMB may allow enrollment in clinical trials of presurgical therapy.
Clinical protocols for decision making using renal mass biopsy for incidental renal masses
Information gained from biopsy may allow improved patient selection for surgery and other treatments. Several studies have critically analyzed the ability of RMB to impact decision making, although the optimal use remains debated. Halverson and colleagues evaluated 133 patients with SRMs and assigned patients to surgery or surveillance based on RMB findings [Halverson et al. 2013]. Of the 97 tumors that were assigned to surgery, agreement between biopsy and final pathology was 100% for identifying malignancy and 94% for distinguishing histology. According to their model, biopsy correctly assigned all 97 patients (90% sensitivity) to surgery while 11 of 36 patients were incorrectly assigned to surveillance based on final pathology. For the entire cohort, agreement between biopsy and final pathology was 92% (95% CI 0.64–0.90). Similarly, Tan et al.analyzed the role of RMB for SRMs to guide decision making [Tan et al. 2012]. The authors determined indications for RMB in 78 (38%) of 204 patients with T1 tumors and identified body mass index greater than 25, juxtahilar tumor location, and high R.E.N.A.L. (it is an acronym for Radius, Exophytic/endophytic properties, Nearness of tumor to hilum, Anterio/posterior, Location) nephrometry score as factors associated with use of RMB on multivariate analysis. The authors conclude that RMB was able to direct treatment-related decision making, with surveillance planned more often for patients with favorable and benign histology and surgical management reserved for aggressive tumors (p < 0.001). The approaches in these two studies highlight the potential for RMB to improve clinical decision making as more asymptomatic renal tumors are diagnosed by cross-sectional imaging. However, the limitations of RMB (Table 4) should be discussed with patients who are risk stratified using these approaches, given the risks with this approach.
Biopsy for evaluation of incidental renal masses: potential impact on patient care
Approximately 20–30% of renal masses are benign following surgical resection [Frank et al. 2003; Gill et al. 2003]. If RMB could reliably identify these patients prior to surgery, a significant proportion of patients with benign tumors could be spared surgery. Despite noted RMB limitations (Table 4), the majority of series have demonstrated accuracy to distinguish between benign and malignant tumors, when biopsy findings are diagnostic. Avoiding treatment in patients with benign tumors would improve overall renal function, as fewer patients would have treatment-related loss of renal function. In addition, patients with benign tumors could be spared the risk of treatment-related complications and the cost of treatment.
Another potential impact of routine RMB that is difficult to measure empirically is the improved ability for informed consent after RMB in patients considering definitive management. Patient awareness of biopsy-proven malignancy may lead to a more informed and assertive decision for management, which appears reasonable given the low procedural morbidity. When atypical renal masses are diagnosed from imaging [Leveridge et al.2010], RMB also allows for distinguishing between rare tumors and uncommon presentations of common tumors, which may also impact management for tumors when nonsurgical treatment is indicated.
Conclusion
Risk stratifying patients with unknown renal masses is important when choosing an acceptable treatment. RMB is associated with a low incidence of complications and may provide valuable information to help patients and physicians decide among treatments. It is important to recognize that RMB may underestimate risk and has limited accuracy when evaluating tumor grade, aggressive pathologic features or T stage. Future studies are necessary to evaluate the optimal use of biopsy in the evaluation and management of incidental renal masses.
Footnotes
Funding
No outside funding was used in this project.
Conflict of interest statement
The authors declare that there is no conflict of interest.