
Abstract
Voiding dysfunction encompasses a wide range of urologic disorders including stress urinary incontinence and overactive bladder that have a detrimental impact on the quality of life of millions of men and women worldwide. In recent years, we have greatly expanded our understanding of the pathophysiology of these clinical conditions. However, current gold standard therapies often provide symptomatic relief without targeting the underlying etiology of disease development. Recently, the use of stem cells to halt disease progression and reverse underlying pathology has emerged as a promising method to restore normal voiding function. Stem cells are classically thought to aid in tissue repair via their ability for multilineage differentiation and self-renewal. They may also exert a therapeutic effect via the secretion of bioactive factors that direct other stem and progenitor cells to the area of injury, and that also possess antiapoptotic, antiscarring, neovascularization, and immunomodulatory properties. Local injections of mesenchymal, muscle-derived, and adipose-derived stem cells have all yielded successful outcomes in animal models of mechanical, nerve, or external urethral sphincter injury in stress urinary incontinence. Similarly, direct injection of mesenchymal and adipose-derived stem cells into the bladder in animal models of bladder overactivity have demonstrated efficacy. Early clinical trials using stem cells for the treatment of stress urinary incontinence in both male and female patients have also achieved promising functional results with minimal adverse effects. Although many challenges remain to be addressed prior to the clinical implementation of this technology, novel stem-cell-based therapies are an exciting potential therapy for voiding dysfunction.
Keywords
Introduction
Voiding dysfunction represents a diverse spectrum of urologic conditions including stress urinary incontinence (SUI) and overactive bladder (OAB): two of the most common and challenging conditions faced by urologists today. Several of these disorders are precipitated by an acute injury such as vaginal delivery in female SUI, or radical prostatectomy in male SUI. The underlying pathophysiology comprises a complex interplay of injuries or altered function at the tissue, nerve, and vascular level that is then exacerbated by underlying comorbidities, including obesity, increasing age, and diabetes mellitus [Luber, 2004].
Despite significant strides in our understanding of the underlying pathophysiology of these clinical conditions, current gold standard therapies remain lacking in their ability to target these fundamental mechanisms of injury or etiology of disease. To date, none of the standard therapies focus on halting disease progression or reversing existing injury. Regenerative medicine concepts have emerged as an exciting means of fulfilling this therapeutic void by restoring and maintaining normal function via direct effects on injured or dysfunctional tissues [Furuta et al. 2007; Wang et al. 2011; Goldman et al. 2012; Vaegler et al. 2012]. Over the past decade, the use of stem cells has shown promise for a host of urologic disorders including applications in lower urinary tract dysfunction, ureteral and bladder trauma, erectile dysfunction, and renal disease [Al-Awqati and Oliver, 2002; Chermansky et al. 2004b ; Bivalacqua et al. 2007; Zhuo et al. 2013].
Stem cells are classically thought to improve tissue repair via multilineage differentiation and self-renewal [Vaegler et al. 2012; Kim et al. 2013]. Stem cells may also exert a therapeutic effect via the secretion of bioactive factors that have antiapoptotic, antiscarring, neovascularization, and immunomodulatory effects on innate tissues and can direct innate stem and progenitor cells to the area of injury [Gnecchi et al. 2008]. Multiple treatment avenues using stem cells for voiding dysfunction, especially SUI, have been evaluated with preclinical animal models and clinical trials demonstrating their potential to restore function via direct effects on the underlying mechanisms that lead to incontinence or voiding dysfunction [Chermansky et al. 2004a; Carr et al. 2008; Fu et al. 2010; Huang et al. 2010; Kim et al. 2010; Lim et al. 2010; Lin et al. 2010; Cruz et al. 2011; Woo et al. 2011; Lee et al. 2012; Carr et al. 2013; Dissaranan et al. 2013; Gotoh et al. 2013; Rovner, 2013]. Nonetheless, many challenges remain to translate these promising results to clinical practice.
In this review, we provide a brief overview of some of the most prevalent clinical conditions that constitute voiding dysfunction and urinary incontinence. We review stem cell sources and their potential mechanisms of action in aiding tissue repair. We then discuss the key preclinical and clinical trials using stem cell therapy for SUI and OAB, and, finally, highlight some of the challenges in translating this promising research from the bench to the bedside as well as future avenues for development.
The clinical problems
SUI in women
SUI, the involuntary leakage of urine during events that result in increased abdominal pressure in the absence of a bladder contraction, is a prevalent condition in women that results from failure of the urethral sphincter, pelvic floor muscles, and fascial support tissues to provide sufficient closure to prevent leakage [Nygaard and Heit, 2004; Chapple and Milsom, 2011]. SUI occurs when intra-abdominal pressure exceeds urethral pressure, resulting in leakage. The incidence of incontinence increases with increasing age and, while daily leakage is less common in young women, up to one third of middle-aged females report leakage at least weekly with 10% reporting daily or severe leakage [Hampel et al. 2004; Hunskaar et al. 2004; Nygaard and Heit, 2004; Appell et al. 2009]. In females, urinary continence relies on an intact urethral sphincteric mechanism. Multiple factors contribute to urethral pressure including bladder neck position, urethral sphincter musculature, sphincter innervation, and surrounding vascular supply and tissue support [Delancey, 1997]. Pregnancy and childbirth are well-recognized risk factors for SUI and four related major mechanisms of injury have been identified: (1) injury to connective tissue support during vaginal delivery; (2) vascular damage due to fetal compression of surrounding pelvic structures; (3) traumatic injury to pelvic nerves and musculature; and (4) direct injury to the lower urinary tract during childbirth [Baessler and Schuessler, 2003; Chapple and Milsom, 2011].
Patients with SUI can benefit from initial conservative measures including pelvic floor physiotherapy, biofeedback, electrical stimulation, and, in some countries, pharmacotherapy; however, surgical options remain the mainstay for cases nonresponsive to conservative measures [Nygaard and Heit, 2004; Dmochowski et al. 2011]. Urethral slings and suspensions aim to correct SUI by correcting hypermobility and augmenting intrinsic sphincter deficiency by allowing urethral compression during periods of increased intra-abdominal pressure without causing obstruction during voiding. At 48 months postoperatively, current surgical techniques for SUI have success rates of 30% for collagen injection, 73% for urethral suspensions, and 82–96% for urethral slings [Nygaard and Heit, 2004; Appell et al. 2009; Dmochowski et al. 2011]. A number of complications can result from sling implantation, including erosion rates in up to 23% of cases, permanent retention in up to 5% of cases, as well as wound complications, bladder perforation, and persistent groin/suprapubic pain and dyspareunia in up to 15% of cases [Kuhn et al. 2009; Dmochowski et al. 2011]. Although SUI is the culmination of diverse injuries to a host of pelvic structures, the current gold standard therapy only indirectly addresses one such aspect of injury by providing mechanical support to a weakened pelvic floor.
SUI in men
SUI in men is most commonly precipitated by radical prostatectomy with a historical incidence between 0.8% and 87% [Bauer et al. 2009]. Contemporary series report improved continence rates following prostatectomy although wide variation continues to exist due to discrepancies in data collection methodology, and patient- versus surgeon-reported outcomes [Walsh et al. 2000]. Nonetheless, while treatment options have improved in recent years, the burden of disease remains high due to the increasing numbers of radical prostatectomies performed annually [Lowrance et al. 2012]. Post-prostatectomy incontinence results from a failure to store urine secondary to inadequate resistance of the outlet sphincter [Potosky et al. 2004; Bauer et al. 2009]. Surgical damage to the urethral sphincter occurs due to direct injury to the sphincter itself, as well as to surrounding nerves and supportive tissue [Radomski, 2013]. As in females, surgical therapies are the mainstay of therapy and include transurethral bulking agents, bulbar urethral slings, and artificial urinary sphincters (AUS). These treatments aim to augment a deficient urinary sphincter by allowing urethral coaptation during periods of increased abdominal pressure without causing outlet obstruction during voiding. However, 5 years post-AUS implantation, up to 24% of men still report severe incontinence, and 28% will have undergone an AUS revision [Dalkin et al. 2003].
OAB
OAB affects up to 12% of men and women [Stewart et al. 2003; Drake and Abrams, 2011; Kim et al. 2013]. While overall prevalence of OAB is similar between genders, the severity of symptoms and phenotype differs. OAB without urgency incontinence is more prevalent in men, and increases in prevalence with increasing age from 0.3% to 8.9% with a marked increase by 64 years of age [Stewart et al. 2003]. In contrast, OAB with urgency incontinence is more prevalent in women and increases in prevalence with age from 2.0% to 19.0% with a significant increase after 44 years of age [Stewart et al. 2003]. OAB is characterized by urgency, with or without urgency urinary incontinence, usually accompanied by frequency and nocturia in the absence of infection or other pathology, and may or may not be associated with detrusor overactivity (DO) on urodynamic evaluation. Normal lower urinary tract function comprises a complex integration of detrusor muscle, urethral, and pelvic floor muscle with hierarchical neural control [Drake and Abrams, 2011]. In OAB, DO may result from increased cellular excitability of the detrusor muscle and/or abnormal neural propagation locally as well as altered peripheral afferent nerve and central nervous system function. Many treatment options are available for patients with OAB, including pharmacologic interventions such as anticholinergics and beta-3 adrenergics, and nonpharmacologic options such as behavioral/dietary modification, biofeedback, and sacral neuromodulation [Andersson, 2013]. However, not all patients obtain adequate relief with current therapies [Basra et al. 2008; Benner et al. 2010]. In addition, many suffer complications or side effects requiring discontinuation of therapy. In a retrospective study by Kelleher and colleagues of women with DO who were treated with immediate release oxybutynin, 59.5% of women reported symptom cure or improvement at 6 months; however, 40% had discontinued medication due to side effects [Kelleher et al. 1997]. Open-label extension studies of five commonly used OAB medications generally show higher levels of medication adherence, although discontinuation of therapy due to adverse events was reported to be as high as 24% of study participants [Basra et al. 2008]
In all of these clinical conditions, current therapies do not repair the original cause of the pathology and may be associated with significant side effects or the need for further invasive treatment. Regenerative medicine represents one promising avenue to restore normal voiding and continence function.
Stem cells: an overview
The field of stem cell research began with the discovery of mouse embryonic stem cells (ESCs) in the early 1970s and with the description of human ESCs in 1998 [Martin, 1981; Thomson et al. 1998]. Stem cells comprise a unique population of cells with three defining characteristics: (1) the ability to self-renew; (2) multipotent differentiation potential, or the ability to differentiate into a number of different cell types; and (3) clonogenicity, or the ability to form clonal cell populations derived from a single stem cell. It is these unique abilities for differentiation and self-renewal that give these cells the potential for restoration of function in multiple tissue types.
Sources of stem cells for therapy
Currently, four broad categories describe the diversity of stem cells being investigated in regenerative medicine: ESCs, stem cells derived from placenta or amniotic fluid (AFPS), induced pluripotent stem cells (IPSC), and adult stem cells (ASC) [Martin, 1981; Thomson et al. 1998; Goldman et al. 2012; Vaegler et al. 2012; Kim et al. 2013]. ESCs are stem cells isolated from an early stage embryo [Thomson et al. 1998]. They represent a pluripotent cell source and can differentiate into all adult cell types. These cells have great therapeutic potential; however, their use is limited by ethical factors. In addition, their clinical application is limited because they represent an allogeneic cell source with the potential to provoke an immune response and because of concerns regarding potential tumorigenicity. Nonetheless, ESCs are currently being investigated for application to type 1 diabetes mellitus and cardiomyopathy [Godfrey et al. 2012; Singla and Abdelli, 2014]. However, for the reasons stated above, ESCs are not being investigated as a treatment for voiding dysfunction or urinary incontinence.
AFPSs are a new class of stem cells with properties intermediate to those of ESCs and ASCs [In ‘T Anker et al. 2003]. They represent a heterogeneous stem cell population derived from the amniotic fluid and placental membrane of the developing fetus. Cells found in these tissues include mesenchymal stem cells (MSCs) as well as multipotent AFPS cells that possess extensive self-renewal capacity. In addition, AFPS cells can be induced to differentiate into cells of all three germ cell layers including cells of adipogenic, osteogenic, myogenic, endothelial, neural, and hepatic lineages. AFPSs are currently being investigated for a variety of applications including treatment of acute tubular necrosis, cardiac valve regeneration for the early correction of congenital cardiac malformations, and as a source of immunomodulatory cells for a variety of immunotherapies [Perin et al. 2010; Moorefield et al. 2011; Weber et al. 2012], but are not being investigated for application in urology.
IPSCs are a unique class of stem cells recently discovered by Takahashi and Yamanaka who demonstrated that specific transcription factors could be used to reprogram differentiated cells to a pluripotent state [Takahashi and Yamanaka, 2006]. Like ESCs, these cells have been shown to possess capacity for multipotent differentiation and self-renewal. In addition, they can be used autologously and their derivation from adult cells obviates concerns regarding ethical issues with ESCs. A disadvantage of IPSCs, however, is the time involved in resetting the cells to a pluripotent state followed by the additional time required to induce the cells to differentiate into the desired lineage [Morris and Daley, 2013]. Furthermore, there remain concerns that full transition to this new desired lineage may not occur [Morris and Daley, 2013]. To date, IPSCs have not yet been used for urologic applications.
ASCs are the most well-studied and well-understood cell type in the field of stem cell therapy and, thus far, are the only stem cell type that have been investigated for urologic applications [Wang et al. 2011; Goldman et al. 2012; Vaegler et al. 2012; Kim et al. 2013]. Over the past decade, ASCs have been identified throughout the body and are thought to act as tissue-specific progenitors that repair damage and restore function locally. MSCs, also known as multipotent adult progenitor cells, are a unique subset of ASCs first described by Friedenstein and colleagues in the 1970s [Friedenstein et al. 1974]. Classically, MSCs were isolated from bone marrow stroma although more contemporary studies have demonstrated that they may also be found in other well-vascularized tissues including adipose, muscle, endometrium, and kidney [Ding et al. 2011]. Unlike tissue-specific progenitor cells, they can be induced to differentiate into multiple cell lineages including bone, neuronal, adipose, muscle, liver, lungs, spleen and gastrointestinal tissues [Ding et al. 2011].
At the present time, MSCs are the primary source of stem cells tested for therapeutic benefit in urologic applications. However, this cell population is relatively rare in bone marrow (approximately 1 per 10,000 cells) and traditional bone marrow procurement is painful, requires general or spinal anesthesia, and potentially produces low yield [Krause et al. 2001]. Alternative cell sources that have been investigated for urologic application include both muscle-derived stem cells (MDSCs) and adipose-derived stem cells (ADSCs) which can be obtained via less-invasive biopsies and in larger quantities under local anesthesia [Goldman et al. 2012]. Investigators continue to identify novel, less-invasive cell sources for urologic application including cells derived from hair follicles, menstrual fluid, and urine [Lavker et al. 2003; Patel et al. 2008; Zhang and Atala, 2008].
Urine-derived stem cells (USCs) are of particular interest for potential urologic applications [Zhang et al. 2008; Bharadwaj et al. 2011; Wu et al. 2011; Liu et al. 2012; Lang et al. 2013; Liu et al. 2013a; Zhang et al. 2013]. In recent studies, Zhang and colleagues have reported the successful isolation and expansion of stem cells from voided human urine [Zhang et al. 2008]. These cells, thought to be MSCs or pericytes from the kidney [Bharadwaj et al. 2011], can be obtained noninvasively from human urine specimens and demonstrate stem-cell-like features including clonogenicity, self-renewal, and multipotent differentiation capacity [Liu et al. 2012]. Single clones of USCs have been shown to have the capacity to expand to yield a large population. Comprehensive characterization studies of these USCs demonstrate their ability to differentiate into multiple cell lineages at the gene/protein expression, cellular and tissue levels [Zhang et al. 2008; Liu et al. 2012]. In vitro studies show that USCs derived from a single clone were, following induction, able to differentiate into smooth muscle and urothelial lineages as evidenced by histologic examination and gene/protein marker assays [Lang et al. 2013]. USCs can also be induced to differentiate into osteogenic, adipogenic, and chondrogenic lineages using different differentiation protocols [Lang et al. 2013]. In vivo studies using BMP-2 and -9 transduced USCs also demonstrated their ability to form bone, fat, and cartilage tissue in immunodeficient female mice [Bharadwaj et al. 2013]. USCs hold several advantages as a cell source for incontinence and voiding dysfunction [Zhang et al. 2008]. They are easily harvested and do not require invasive surgical techniques to obtain. Furthermore, they are easily isolated with a significant cost advantage at US$50 to obtain cells from urine compared with approximately US$5000 to obtain cells using a biopsy procedure [Liu et al. 2013a]. Finally, they can be used autologously, obviating potential ethical issues or the potential of adverse immune reactions.
Stem cell procurement
The procurement and isolation of stem cells for therapeutic use typically occurs in three stages [Vaegler et al. 2012]. The patient initially undergoes a procedure to harvest the cells. Following procurement, the tissue specimen is then transported to a regulated facility for isolation from other cell types. Here, the cells are grown via a process of ex vivo stem cell expansion involving multiple cycles of differentiation and senescence until adequate numbers are reached. Finally, cell sorting may or may not be used to isolate stem cells prior to therapeutic application, as this process is often labor-intensive and expensive. Thus, the cells that are ultimately administered to the patient may comprise a heterogeneous combination of stem cells and differentiated cells. Although still investigational, it is feasible during this process to manipulate the cells for a variety of therapeutic applications. For example, cells can be predifferentiated toward a specific cell lineage, pre-exposed to an environment similar to the in vivo post-transplant environment, or transfected to produce specific cytokines or growth factors [Arthur et al. 2008; Yang et al. 2009].
Stem cell mechanisms of action
Stem cell homing
The process of innate systemic stem cell delivery to the site of injury is termed “homing” and can be taken advantage of in delivering cells systemically rather than locally. In contrast to tissue-specific progenitor cells, MSCs derived from the bone marrow traverse the circulatory system with access to all tissues in the body but then migrate to specific locations such as areas of acute injury following chemokine gradients where they can engraft and facilitate healing and regeneration [Deans and Moseley, 2000; Sohni and Verfaillie, 2013]. Much of the insight regarding stem cell homing derives from literature regarding leukocyte migration into injured tissue, metastatic cancer cells, and hematopoietic stem cells [Wynn et al. 2004; Sohni and Verfaillie, 2013]. Similar to leukocytes, MSCs express cell surface receptors and adhesion molecules responsible for directing cellular migration and homing to particular tissues, including the chemokine receptor CXCR4 and its binding partner CXCL12 [Wynn et al. 2004] as well as the chemokine ligands: CCR1, CCR4, CCR7, CCR10, CCR9, CXCR5, and CXCR6 [Honczarenko et al. 2006]. MSCs are hypothesized to migrate to target tissues via a process similar to that of leukocyte migration: initial localization by means of chemoattraction, adhesion to vascular endothelial cells at the target site, and, finally, transmigration across the endothelium to the site of injury. Integrins and selectins are other classes of cell surface molecules that direct migration and adhesion of a variety of cells, including MSCs [Docheva et al. 2007]. While the role of these molecules in leukocyte-endothelial adhesion is well established, their exact role in facilitating MSC interaction with endothelium is less well characterized. Ruster and colleagues found that binding and rolling of MSCs was mediated by P-selectin while migration involved binding of the integrin VLA-4 on MSCs with VCAM-1 on endothelial cells [Rüster et al. 2006].
A large body of literature utilizing animal models has demonstrated the ability of MSCs to home to injured tissues in several disease models including cardiac injury, renal failure, and skin wounds [Bartholomew et al. 2002; Askari et al. 2003; Tögel et al. 2005]. In addition, recent work investigating MSCs for SUI has shown that chemokine ligand 7 (CCL7), a homing factor for MSCs, is upregulated in both the urethra and vagina after vaginal distension (VD), suggesting that intravenously administered MSCs could have the potential to home to sites of injury in SUI [Woo et al. 2007; Wood et al. 2008; Lenis et al. 2012]. Subsequent literature examining intravenous injection of MSCs in a VD rat model of simulated childbirth injury showed that MSCs home to the urethra and vagina and facilitate recovery of continence as measured by leak point pressure (LPP) [Cruz et al. 2011; Dissaranan et al. 2013]. Recent work by Lenis and colleagues used a rat model of childbirth injury with both virgin rats that had undergone VD and postpartum rats to further investigate the expression of chemokines and receptors involved in stem cell homing and tissue repair [Lenis et al. 2013]. They showed that VD in virgin and postpartum rats resulted in upregulation of urethral CCL7 expression. In addition, pregnancy and delivery was found to upregulate the chemokine receptor CD191 but to decrease the expression of hypoxia inducible factor 1α (HIF1α) and vascular endothelial growth factor (VEGF). Similarly, in a mouse model of OAB via bladder outlet obstruction, Woo and colleagues showed that intravenously injected MSCs following bladder injury were associated with increased chemokine ligand 2 (CCL2) expression in the affected tissue [Woo et al. 2011].
In therapeutic applications, stem cell homing is affected by a variety of factors including age and passage number of the cells, culture conditions, and the delivery method [Sohni and Verfaillie, 2013]. Rombouts and Ploemacher demonstrated that with increasing age and passage number, the efficiency of MSC engraftment decreases, possibly due to rapid aging of the cells with increased in vitro multiplication [Rombouts and Ploemacher, 2003]. Reproduction of the innate MSC microenvironment in vitro is challenging and plays a significant role in stem cell homing potential. For example, in vitro expression of matrix metalloproteinases (MMPs), key factors to stem cell migration, is affected by cell culture factors such as hypoxia and culture confluence and may be upregulated with the addition of certain inflammatory cytokines, such as transforming growth factor beta 1 (TGFβ1), interleukin (IL)-1β, and tumor necrosis factor (TNF)-α [De Becker et al. 2007]. Despite the appeal of delivering cells systemically rather than locally, systemically infused MSCs often suffer from a first-pass effect whereby these larger cells become trapped in capillary beds of various tissues, especially the lungs, liver, and spleen, decreasing their therapeutic bioavailability and functionality [Fischer et al. 2009]. To overcome this, recent investigations have utilized an intraperitoneal delivery route for MSCs and have obtained higher yield in target tissues [Ghionzoli et al. 2010].
Stem cell differentiation
The mechanism of action of stem cells was initially thought to primarily derive from their ability to differentiate into multiple cell types and regenerate damaged tissues. To date, treatment avenues for voiding dysfunction and urinary incontinence have focused on this potential to restore function via differentiation to replace injured or diseased tissues such as smooth or striated muscle for urethral sphincter regeneration and urothelial tissue for bladder, urethral, and upper urinary tract reconstruction [Al-Awqati and Oliver, 2002; Chermansky et al. 2004b; Cruz et al. 2011]. It is thought that MSCs restore function in SUI primarily by their ability to differentiate into multiple cell lineages, with animal studies demonstrating increases in urethral muscle, nerves, and connective tissue following MSC injection [Chermansky et al. 2004b; Fu et al. 2010; Kim et al. 2010; Lin et al. 2010]. MSCs have also been induced to differentiate into a smooth muscle phenotype when exposed to conditioned media from smooth muscle cell cultures or when induced with specific myogenic growth factors for application to bladder reconstruction [Wu et al. 2013]. More recent work, however, suggests a more complex role of stem cells in functional recovery, with some studies demonstrating that paracrine secretions of MSCs play an important role in the regeneration process [Carvalho et al. 2011; Ranganath et al. 2012; Dissaranan et al. 2013].
Bioactive effects of stem cells
Recent research has demonstrated that, in addition to differentiating into target tissue types, stem cells likely exert a therapeutic effect via the secretion of bioactive factors since few MSCs engraft and remain long term in target tissues, in contrast to their large therapeutic effect [Carvalho et al. 2011; Ranganath et al. 2012; Dissaranan et al. 2013]. MSCs also activate and direct endogenous stem and progenitor cells to areas of injury via the secretion of cytokines and chemokines [Caplan and Dennis, 2006]. In addition, their secretions have antiapoptotic, antiscarring, and neovascularization effects, as well as immunomodulatory properties [Deans and Moseley, 2000]. The investigation of this protein milieu or “secretome” is a subject of growing interest with the increasing recognition of the paracrine/autocrine role of cell secretions in the regulation of many physiological processes and their potential for therapeutic application. The investigation of these cell-specific proteins often begins in cell culture. While in vitro studies cannot fully capture and test the totality of MSC secretions in the in vivo microenvironment, researchers seek to replicate the effects of the MSC secretome via the use of media conditioned by the MSCs and containing their secretions [Stastna and Van Eyk, 2012].
MSCs also possess immunomodulatory and immunological tolerance inducing characteristics. These cells typically express MHC-I but lack expression of MHC-II, CD40, CD80, and CD86. Owing to the lack of co-stimulatory cell surface molecules, MSCs fail to induce an immune response by the transplant host [Ryan et al. 2005]. MSCs have also been shown to play a role in suppressing immune responses by modulation of T-cell activation and proliferation through both direct cell–cell interaction and via the action of soluble factors [Ryan et al. 2005]. These immunomodulating properties are currently being investigated in myriad applications including prevention of graft-versus-host disease following allogeneic transplantation and Crohn’s disease [Duijvestein et al. 2008; Ball et al. 2013]. Clinical trials in cardiology have taken advantage of these properties of MSCs to investigate the efficacy of nontype-matched allogeneic MSC transplantation [Hare et al. 2009; Telukuntla et al. 2013]. In a study by Hare and colleagues 1 year after intravenous administration of allogeneic human MSCs in reperfused myocardial infarction patients, recovery, as measured by global symptom score, ejection fraction, ambulatory electrocardiogram monitoring, and pulmonary function testing, was significantly improved in treated patients compared with those that received a placebo [Hare et al. 2009]. In addition, no signs of rejection were observed and adverse event rates were comparable between treated and placebo arms.
A recent study by Dissaranan and colleagues demonstrates that the secretome of MSCs can facilitate recovery of continence as measured by LPP following VD in a rat model; moreover, rats treated locally with MSC secretome, as contained in conditioned media, exhibited an increase in elastin fibers and urethral smooth muscle, which may have contributed to the restoration of continence [Dissaranan et al. 2013]. A study of hamsters with heart failure suggests that MSCs act systemically as well as locally [Shabbir et al. 2009]. In this study MSCs injected into the hamstrings of affected animals were unable to migrate from the injection site; however, the authors found that treated animals still benefited from stem cell injection based on histologic and functional analysis of the myocardium. More recent work by Timmers and colleagues utilizes human MSC secretions collected as conditioned medium in a pig model of myocardial infarction [Timmers et al. 2011]. Pigs underwent left circumflex coronary artery and were then administered intravenous conditioned media for 7 days. At 3 weeks following initial cardiac injury and treatment, pigs treated with MSC conditioned media were found not only to have increased myocardial vascular density but also reduced infarction size and more preserved cardiac function.
These findings have been borne out in other urologic investigations as well. Lin and colleagues investigated rats subjected to VD and ovariectomy that were subsequently treated with intraurethral injection of ADSCs; despite limited cell engraftment on histologic analysis, these rats demonstrated significant functional recovery [Lin et al. 2010]. Similarly, a study by Song and colleagues utilizing bladder wall injections of MSCs demonstrated functional recovery in a rat model of OAB from partial bladder outlet obstruction (PBOO) despite limited engraftment 4 weeks post-treatment [Song et al. 2012]. Further investigations into the use of stem cell bioactive factors could someday obviate the need for cellular injections in future stem cell therapies.
Stem cell therapy for voiding dysfunction
Stem cells for stress urinary incontinence
Various animal models of simulated childbirth have been used to mimic the injuries that can produce SUI and enable preclinical testing of potential therapies for this prevalent condition [Jiang and Damaser, 2011]. The first animal model was introduced by Lin and colleagues in 1998 and utilized VD in female rats to simulate the trauma of childbirth [Lin et al. 1998]. VD results in damage to surrounding muscles and nerves responsible for continence as evidenced by increased levator muscle edema and smooth muscle disruption, as well as hypoxic injury [Lin et al. 1998]. Since this initial study, multiple models have been developed to investigate other putative mechanisms of injury to the continence mechanism, including nerve injury, direct urethral injury, and pelvic ligament injury [Kerns et al. 2000; Chermansky et al. 2004a; Kefer et al. 2009]. These include: (1) simulation of nerve injury via pudendal nerve crush (PNC); (2) simulation of anatomic support damage with urethrolysis or pubourethral ligament injury; (3) simulation of intrinsic urethral defects with periurethral cauterization, urethral sphincterectomy, or pudendal nerve transection; and (4) combination models such as those with both VD and PNC. Selected studies utilizing stem cell or stem cell secretome therapy for treatment of SUI are summarized in Table 1.
Selected preclinical and clinical studies of stem cells or stem cell secretome for stress urinary incontinence.

ADSC, adipose-derived stem cell; CCM, concentrated conditioned media; GFP, green fluorescent protein; LPP, leak point pressure; MDSC, muscle-derived stem cell; MSC, mesenchymal stem cell; SUI, stress urinary incontinence; VD, vaginal distension.
Most research testing novel cell-based therapies for SUI has focused on direct stem cell injection into the urethra with the hope of repairing or regenerating damaged rhabdosphincter tissue [Chermansky et al. 2004b; Carr et al. 2008; Fu et al. 2010; Kim et al. 2010; Carr et al. 2013; Gotoh et al. 2013]. Local injections of MSCs, MDSCs, and ADSCs have all demonstrated efficacy in animal models of either mechanical, nerve, or external urethral sphincter injury, as demonstrated by both anatomic and functional outcomes.
MDSCs have been shown to improve sphincter function in several animal models of SUI. Chermansky and colleagues investigated MDSCs in an animal model of urethral injury by midurethral cauterization. MDSC injection 1 week after injury led to significant tissue recovery as evidenced by increased LPP 2, 4, and 6 weeks afterwards compared with controls [Chermansky et al. 2004b]. Tissue staining confirmed integration of MDSCs into the striated muscle layer of the urethra. Similarly, Kim and colleagues injected MDSCs into the urethra of rats that had previously undergone pudendal nerve dissection 2 weeks prior [Kim et al. 2010]. By 4 weeks after MDSC injection, LPP and urethral closure pressure in animals that had undergone stem cell administration and nerve injury were restored to values comparable to rats that had undergone only a sham operation. Furthermore, the injected MDSCs stained positive for muscle-specific markers, suggesting the potential for MDSCs to differentiate into muscle lineage cells that may contribute to the repair of damaged muscle tissue.
ADSCs have also been investigated for treatment of SUI. A pilot study by Jack and colleagues investigated the potential for ADSCs to survive within bladder and urethral smooth muscle [Jack et al. 2005]. Human ADSCs derived from lipoaspirate of female patients undergoing liposuction were directly injected into the bladder and urethra of athymic rats and mice immediately following laparotomy. Histologic analysis of the bladder and urethra of treated animals was performed 2, 4, 8, and 12 weeks afterwards and demonstrated ADSC viability and incorporation into the recipient smooth muscle. By 8 weeks, ADSCs also demonstrated in vivo expression of α-smooth muscle actin, an early marker of smooth muscle differentiation. In a more recent publication by Fu and colleagues ADSCs that had been induced into myoblasts were injected periurethrally in rats that had undergone VD [Fu et al. 2010]. Both maximal bladder capacity and LPP were shown to be significantly increased 1 and 3 months post-injury compared with control rats that had been implanted with untreated ADSCs. In addition, histologic analysis showed increased thickness of the inferior muscularis in urethral mucosa which may have contributed to improved sphincter contractility and decreased SUI in injured rats. A study by Lin and colleagues investigated the use of periurethrally injected ADSCs in postpartum rats that then immediately underwent VD to simulate prolonged delivery [Lin et al. 2010]. One week following injury, rats were subjected to ADSC transplantation. Urinary function and histological analysis was then performed 4 weeks later. Cystometric analysis demonstrated that ADSC-treated animals had a significantly lower incidence of abnormal voiding compared with untreated animals. Histologic analysis demonstrated that treated animals, particularly treated animals that then achieved normal voiding function, had higher urethral elastin and smooth muscle content [Lin et al. 2010].
Recent studies have focused on elucidating the mechanism of action of cell treatment in SUI models: specifically, the potential contribution of paracrine/autocrine factors to tissue recovery following childbirth injury. A study by Cruz and colleagues demonstrated that intravenous injection of MSCs following childbirth injury may represent an effective route for cell-based therapy [Cruz et al. 2011]. In their work, green fluorescent protein (GFP)-labeled MSCs from bone marrow were injected into rats 1 hour after VD or sham VD. Imaging 4 and 10 days post-treatment demonstrated that significantly more MSCs homed to the urethra and surrounding tissues in animals that had undergone VD. Their work suggests that, following injury, tissues release factors that promote mobilization and attraction of MSCs to the injured site [Cruz et al. 2011]. A subsequent study by Dissaranan and colleagues further investigated MSC homing as well as the potential role of the MSC secretome in facilitation of functional recovery after VD [Dissaranan et al. 2013]. MSCs or media conditioned by the MSCs and then concentrated, or concentrated conditioned media (CCM), was administered intravenously and periurethrally, respectively, to rats 1 hour after VD or sham VD. Urethral histology and function were assessed one week following treatment. As with the study by Cruz and colleagues, significantly more MSCs were found in the urethra and surrounding tissues in animals that had undergone VD versus sham VD. Interestingly, continence, as assessed by LPP, was found to not only be improved in injured animals that had received intravenous MSCs but also in those that had received a periurethral injection of CCM. The recovery of function utilizing only the secretions of MSCs is a fascinating discovery that suggests the possibility of an acellular stem cell-derived therapy.
Carr and colleagues performed the first North American MDSC therapy trials for SUI [Carr et al. 2008]. A follow-up expanded study by the same group has demonstrated promising results [Carr et al. 2013]. A total of 38 women with SUI that had not improved with a trial of 12 or more months of conservative therapy received intrasphincteric injection of MDSCs derived from autologous lateral thigh muscle biopsies. Subjects also had the option of electing a second treatment of the same dose of MDSCs at 3-month follow up. Assessments were then made 1, 3, 6, and 12 months following the last treatment. Of the 33 subjects who completed the study, nearly 90% in the high-dose group experienced a 50% or greater reduction in pad weight, and nearly 80% had a 50% or greater reduction in diary-reported stress leaks. Adverse side effects from the treatment were limited to minor events such as pain or bruising at the injection or biopsy sites [Carr et al. 2013].
Gotoh and colleagues recently investigated the efficacy and safety of periurethral injection of ADSCs in 11 men who had persistent SUI more than 2 years following prostate surgery (radical prostatectomy or holmium laser enucleation of the prostate) [Gotoh et al. 2013]. One-year outcomes demonstrated 59.8% decrease in leakage volume on a 24-hour pad test, decreased frequency and improved quality of life. In addition, mean maximum urethral closure pressure and urethral functional profile length were increased compared with pretreatment values, and magnetic resonance imaging demonstrated the sustained presence of injected adipose tissue. No adverse events occurred during ADSC procurement and administration nor were any severe side effects or changes in serum prostate specific antigen levels reported during the follow-up period [Gotoh et al. 2013]. As with the study by Carr and colleagues, however, these feasibility studies are limited by their lack of a control group and small sample size. Nonetheless, these initial open label safety trials are necessary prior to moving on to controlled double-blinded clinical trials.
The use of stem cells in conjunction with existing or emerging therapies is another nascent area of research. For instance, Zou and colleagues have combined stem cell therapy with slings in an effort to augment the long-term efficacy of slings and reduce rates of sling erosion or extrusion [Zou et al. 2010]. In this study, female rats underwent bilateral proximal sciatic nerve transection and developed SUI confirmed by LPP measurement 4 weeks following injury. At this time, rats were treated with either no sling, a silk sling, or a tissue-engineered sling composed of a silk scaffold that had been seeded with MSCs. Histology and LPP testing 4 and 12 weeks later, and collagen and mechanical testing 12 weeks after implantation, showed that animals treated with the tissue-engineered sling had nearly normal LPP, higher collagen content, and higher failure force compared with untreated animals [Zou et al. 2010]. Liu and colleagues tested genetically modified urine stem cells that overexpress VEGF [Liu et al. 2013b]. Collagen hydrogel scaffolds containing VEGF-overexpressing stem cells were subcutaneously implanted in mice. This cell subset was found to enhance angiogenesis and improve cell engraftment in addition to promoting myogenic differentiation and innervation by USCs [Liu et al. 2013b].
Stem cells for OAB
The reliance on urgency as a defining symptom in OAB has been a complicating factor for its investigation because of the difficulty of assessing this symptom in animal models. At present, PBOO is the most well-known and well-established model for DO [Kim et al. 2013]. However, PBOO only comprises one possible etiology of OAB symptoms. Other models of voiding dysfunction including those involving bladder ischemia, diabetes, spinal cord injury, and cryo-injury have also been utilized to test cell-based therapies for voiding dysfunction [Nagatomi et al. 2004; Daneshgari et al. 2009; Chen et al. 2012; Kim et al. 2013]. Selected studies utilizing stem cell therapy for treatment of voiding dysfunction are summarized in Table 2.
Selected preclinical studies of stem cells for voiding dysfunction.
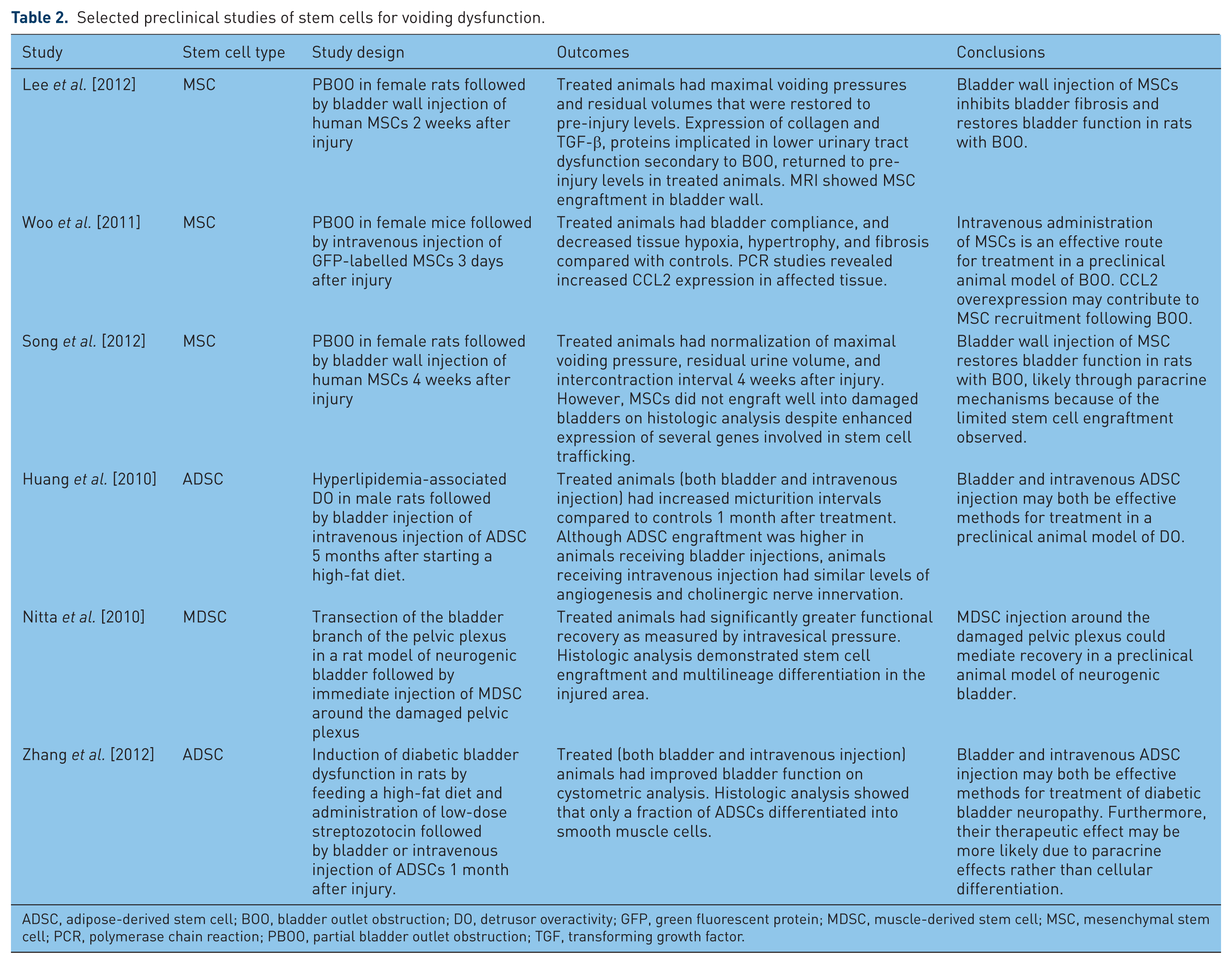
ADSC, adipose-derived stem cell; BOO, bladder outlet obstruction; DO, detrusor overactivity; GFP, green fluorescent protein; MDSC, muscle-derived stem cell; MSC, mesenchymal stem cell; PCR, polymerase chain reaction; PBOO, partial bladder outlet obstruction; TGF, transforming growth factor.
In a recent study by Lee and colleagues human MSCs labeled with nanoparticles were injected into the bladder wall of rats 2 weeks following induction of PBOO [Lee et al. 2012]. Follow up studies, including magnetic resonance imaging (MRI), histology, and functional studies, were performed 4 weeks after treatment. Following induction of PBOO, collagen and TGF-β protein levels increased, consistent with the hypothesis that increased collagen deposition in older men with PBOO leads to lower urinary tract dysfunction. Following MSC transplantation, however, the expression of both proteins returned to pre-injury levels along with maximal voiding pressures and residual volume. MRI confirmed engraftment of MSCs in the bladder wall while maximal voiding pressure and residual urine volume were found to be recovered after MSC transplantation [Lee et al. 2012]. In a different experiment mice received MSCs intravenously 3 days after induction of PBOO [Woo et al. 2011]. Urodynamic and histological evaluation were performed 4 weeks post-treatment and MSCs were found in the detrusor muscle and were correlated to decreased levels of tissue hypoxia, hypertrophy, and fibrosis as well as improved bladder compliance. PCR studies revealed increased CCL2 expression in the affected tissue, suggesting the CCL2 overexpression may contribute to MSC recruitment following PBOO [Woo et al. 2011].
As in SUI, growth factors also play an important role both in normal bladder development and in bladder remodeling following injury [Altuntas et al. 2012; Song et al. 2013]. In addition to direct effects via stem cell implantation and differentiation, the paracrine effects of MSCs have been studied in the repair of PBOO-induced DO [Song et al. 2012, 2013]. In a study by Song et al. injection of human MSCs into the bladder wall of rats was performed 4 weeks after onset of PBOO [Song et al. 2012]. MSC therapy led to normalization of OAB outcomes, including maximal voiding pressure, residual urine volume, and intercontraction interval within 4 weeks. Notably, histologic analysis demonstrated that the transplanted MSCs did not engraft well into the damaged bladders despite enhancing the expression of several genes responsible for stem cell trafficking [Song et al. 2012]. These changes in gene expression suggest that paracrine mechanisms of tissue repair may be the dominant mechanism of action of MSC therapy.
Stem cell therapy using other models of DO have also shown promise. Huang and colleagues report the use of autologous ADSCs to ameliorate DO in a hyperlipidemia-associated rat model of DO [Huang et al. 2010]. Rats were administered a high-fat diet for 5 months. At this time, all rats underwent fat harvest for procurement of ADSCs. After culture and purification, ADSCs were delivered by direct bladder injection as well as intravenously. Functional and histologic studies were then performed 1 month after treatment. ADSC-treated rats were found to have longer micturition intervals compared with untreated rats. In addition, nerve and blood vessel density were lower in untreated rats compared with ADSC-treated animals. While more ADSCs collected within the bladder following local injection compared with systemic injection, treatment with ADSCs via both routes improved both angiogenesis and cholinergic nerve innervation [Huang et al. 2010]. In another study, rats underwent transection of the bladder branch of the pelvic plexus and were immediately injected around the damaged pelvic plexus with rat MDSCs [Nitta et al. 2010]. Four weeks following injury and treatment, the transplantation group demonstrated significantly greater functional recovery as assessed by intravesical pressure compared with control treated groups. Histologic analysis showed that transplanted cells engrafted into the injured area with differentiation into multiple cell lineages.
Bladder dysfunction manifesting as urothelial dysfunction, alteration in smooth muscle, and neuronal damage is a known sequelae of diabetes mellitus. In a study by Zhang and colleagues rats were fed a high-fat diet and treated with low-dose streptozotocin to induce diabetes [Zhang et al. 2012]. A month later, rat ADSCs were either injected intravenously or directly into the detrusor. One month post-treatment, cystometric analysis demonstrated improved bladder function compared with untreated animals [Zhang et al. 2012]. Furthermore, histologic analysis showed that only a small fraction of transplanted ADSCs differentiated into smooth muscle cells, suggesting that cellular differentiation plays a minor role in the therapeutic benefit of ADSCs. They hypothesize that paracrine release of cytokines and growth factors may, in part, account for the beneficial effects of stem cell transplantation [Zhang et al. 2012].
Conclusions
To date, stem cells have shown promise for the treatment of voiding dysfunction. Applications in SUI and OAB have demonstrated success in both preclinical animal trials and limited clinical trials. However, stem cells have not yet been tested as a potential treatment for interstitial cystitis or painful bladder syndrome, both of which have the potential to be reversed or ameliorated via the immunomodulatory effects of stem cells. Many questions need to be answered before stem cell therapy can be introduced into urologic practice for voiding dysfunction.
For example, there remains much to be elucidated regarding the mechanisms of stem cell action. Previously, the beneficial effects of stem cells were primarily attributed to their ability to differentiate into multiple cell types and to thus directly augment injured or dysfunctional tissues in voiding disorders [Pittenger et al. 1999]. However, emerging concepts regarding the paracrine actions of stem cells and their effects on tissue healing from angiogenesis, antioxidant properties, and immunomodulation, have opened up new avenues for investigation [Deans and Moseley, 2000; Gnecchi et al. 2008]. The successful use of stem cell bioactive factors, or secretome, in nonurologic and early urologic applications could eventually pave the way for cell-based but cell-free therapies in the future [Carvalho et al. 2011; Ranganath et al. 2012; Dissaranan et al. 2013].
Practical considerations in translating stem cell technology from the bench to the bedside comprise another critical hurdle to overcome. SUI and many of the causes of OAB syndrome are chronic in nature. However, the preclinical models used to date only produce and address acute disease symptomatology. Assessing the efficacy of stem cell therapy for chronic voiding dysfunction will need to be validated further in clinical trials. In addition, work still needs to be performed to identify the best delivery method for stem cells including how to overcome first pass effects and subsequent loss of bioactive potential, as well as to identify the best sources of stem cells for urologic applications. In this vein, recent work by Zhang and colleagues utilizing USCs represents a promising alternate autologous cell source that could be easily harvested and isolated [Zhang et al. 2008]. However, to date, the potential of USCs in animal models of voiding dysfunction remains to be investigated.
Immune considerations regarding stem cell therapies represent another important avenue of necessary investigation. Future stem cell therapies may not always rely on the constraint of using autologous cell sources since autologous cell sources from older individuals, those with genetic disorders, and those who have received systemic treatments such as radiation may not be as efficacious as stem cells derived from younger healthy individuals [Fan et al. 2010]. While allogeneic stem cells have been tested safely for other diseases [Hare et al. 2012], efficacy of allogeneic cell sources for voiding dysfunction have yet to be demonstrated in humans.
In summary, voiding dysfunction and urinary incontinence constitute a variety of common disorders affecting millions of men and women worldwide. Current treatments are limited and do not address the underlying pathophysiology of disorder or disease, nor do they repair damaged or diseased tissue to restore normal function. In contrast to current therapies, stem cells have emerged as an exciting treatment avenue targeting disease progression and potentially correcting pathophysiology. Although many challenges remain to be addressed before clinical implementation of this technology, preclinical animal and early clinical studies show promise in the use of stem cell therapy for voiding dysfunction and urinary incontinence.
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This work was supported by the National Institutes of Health [grant number NIH R01 HD059859], the Rehabilitation Research and Development Service of the Department of Veterans Affairs [grant number B7225R], and the Cleveland Clinic.