
Abstract
The treatment of metastatic castrate-resistant prostate cancer (mCRPC) has evolved rapidly with the recent approval of a number of treatments and agents, including docetaxel, sipuleucel T, abiraterone, cabazitaxel, and enzalutamide. Enzalutamide (previously MDV-3100) is a novel oral androgen receptor inhibitor that targets multiple steps in the androgen receptor signaling pathway. The randomized phase III AFFIRM study demonstrated significant improvements in a number of efficacy endpoints, including the primary endpoint of overall survival and secondary endpoints of progression-free survival, and time to prostate-specific antigen progression in patients with progressive mCRPC who had received prior treatment with docetaxel. Enzalutamide was well tolerated and there were comparable incidences of grade 3 or greater adverse events reported for the enzalutamide and placebo control arms in AFFIRM. Unlike some other treatments for mCRPC, enzalutamide does not require administration with steroids. The ongoing randomized phase III PREVAIL trial will investigate the efficacy and safety of enzalutamide in chemotherapy-naïve patients with mCRPC. Additional trials are investigating the use of enzalutamide in a number of disease settings.
Introduction
Prostate cancer is the second most commonly diagnosed malignancy in men, with approximately 900,000 new cases worldwide each year (http://globocan.iarc.fr/). The most current data from the GLOBOCAN database for 5-year prevalence estimates approximately 3,200,000 men living with the disease (see http://globocan.iarc.fr/). It is estimated that approximately 22% of patients have locally advanced or metastatic disease at presentation [British Association of Urological Surgeons, 2009].
For the past decade, the taxane docetaxel has been the cornerstone of treatment for metastatic castration-resistant prostate cancer (mCRPC) based on the survival benefit demonstrated in the landmark randomized phase III TAX 327 trial [Tannock et al. 2004; Berthold et al. 2008]. However, despite the clinical benefits associated with this cytotoxic chemotherapy agent, patients eventually progress in their disease. Until recently, a major challenge in the management of mCRPC has been the treatment of patients who no longer respond to androgen ablation therapy and whose condition has failed to respond to chemotherapy with docetaxel. Another taxane agent, cabazitaxel, has shown an incremental survival benefit of 2.4 months in patients with mCRPC who progressed on prior docetaxel and is now approved in the postdocetaxel setting [de Bono et al. 2010]. However in some patients, cabazitaxel can be associated with significant toxicities, such as neutropenia, febrile neutropenia, and anemia [de Bono et al. 2010]. Cabazitaxel may not be appropriate for certain patient populations, such as older people and patients with comorbidities. More recently, two efficacious agents with improved safety profiles have been approved in the postdocetaxel setting, abiraterone and enzalutamide (Table 1) [de Bono et al. 2011; Fizazi et al. 2012; Scher et al. 2012].
First- and second-line agents for the treatment of metastatic castrate-resistant prostate cancer.
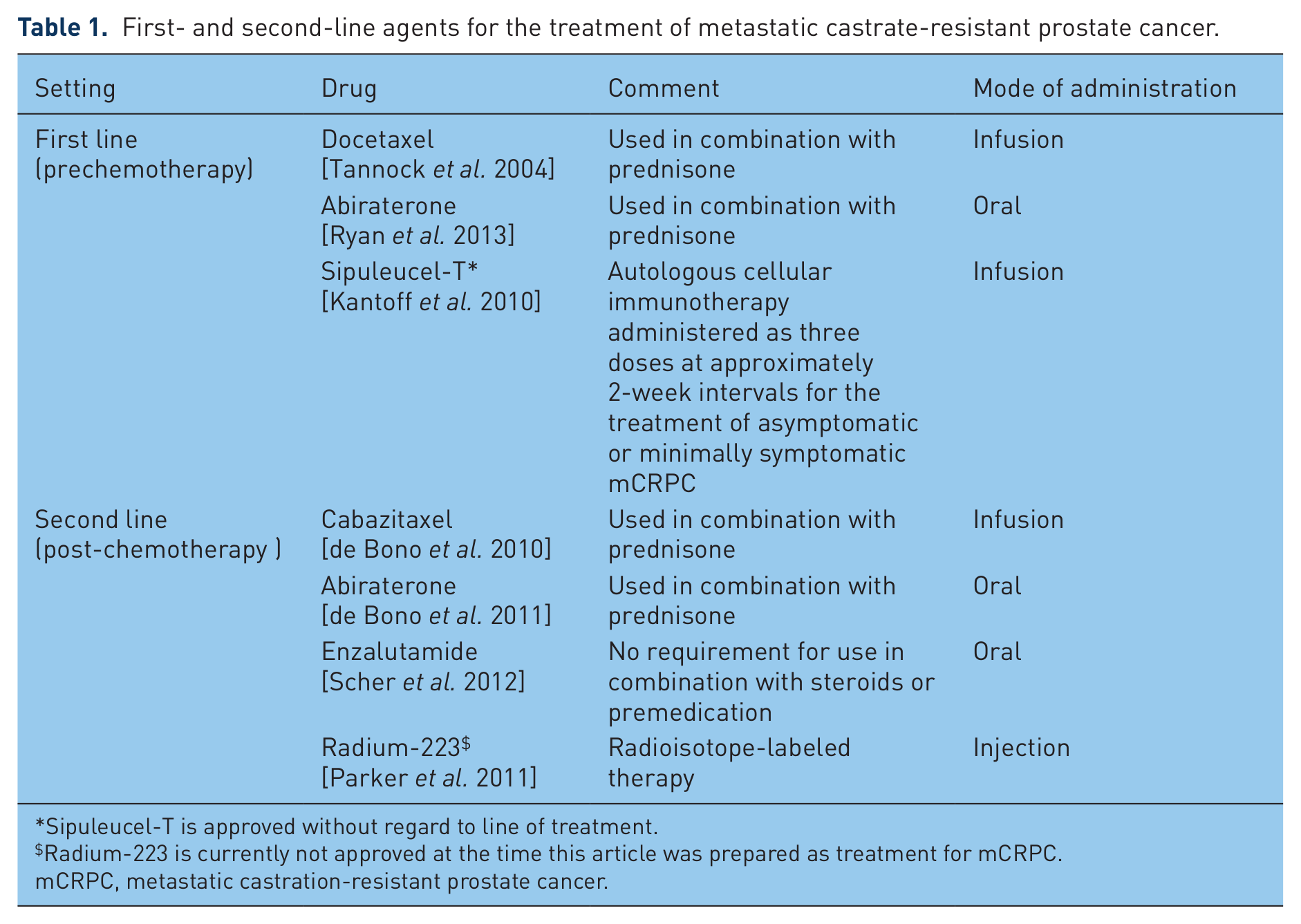
Sipuleucel-T is approved without regard to line of treatment.
Radium-223 is currently not approved at the time this article was prepared as treatment for mCRPC.
mCRPC, metastatic castration-resistant prostate cancer.
Abiraterone acetate is converted in vivo to abiraterone, an androgen biosynthesis inhibitor, that inhibits 17 α-hydroxylase/C17,20-lyase. This enzyme is expressed in testicular, adrenal, and prostatic tumor tissues and is required for androgen biosynthesis [O’Donnell et al. 2004]. Abiraterone, administered in combination with prednisone, has been shown to significantly improve overall survival (OS), time to prostate-specific antigen (PSA) progression, and radiographic progression-free survival (rPFS) in patients with mCRPC who had received prior chemotherapy [de Bono et al. 2011; Fizazi et al. 2012]. Mineralocorticoid-related adverse events (AEs), including fluid retention, hypertension, and hypokalemia, were more frequently reported in the abiraterone acetate–prednisone arm.
Enzalutamide is a potent oral androgen receptor (AR) inhibitor that has also shown significant OS, time to PSA progression and rPFS benefits [Scher et al. 2012]. In addition, enzalutamide does not require coadministration with corticosteroids. In this review of enzalutamide for mCRPC, the mechanism of action, early phase development, registrational phase III AFFIRM study in the mCRPC postchemotherapy setting, and ongoing clinical development will be discussed.
Enzalutamide mechanism of action
Hormone-resistant prostate cancer cells actually have an increased number of ARs on their membrane surface and are still sensitive to stimulation and growth by androgenic hormones [Mohler, 2008]. In addition there is evidence that prostate cancer cells themselves have the capacity to synthesize androgen and stimulate their own growth (autocrine mechanism). Significantly, the AR is expressed at high levels in the majority of cases of castrate-resistant prostate cancer, and these tumors resume their expression of multiple AR-regulated genes, indicating that AR transcriptional activity becomes reactivated at this stage of the disease [Yuan and Balk, 2009]. The molecular basis for this AR reactivation remains unclear.
Enzalutamide is a rationally designed oral AR inhibitor that inhibits multiple steps in the AR signaling pathway (Figure 1) [Tran et al. 2009]. The mechanism of action for enzalutamide is threefold. It is a potent, competitive binder of androgens at the level of the AR. It prevents the translocation of the AR from the cytoplasm to the nucleus. Within the nucleus, it inhibits AR binding to chromosomal DNA, which prevents further transcription of tumor genes.

Mechanism of action of enzalutamide. HSPs, heat shock proteins;
Early study of enzalutamide in metastatic castrate-resistant prostate cancer
The efficacy and safety of enzalutamide was first investigated in a phase I–II study of 140 patients with progressive mCRPC in five US centers [Scher et al. 2010]. Of the 140 patients, 65 had not received prior chemotherapy treatment. Patients were enrolled in dose-escalation cohorts of three to six patients and given an oral daily starting dose of 30 mg. The final daily doses studied for each patient cohort were 30 mg (n = 3), 60 mg (27), 150 mg (28), 240 mg (29), 360 mg (28), 480 mg (22), and 600 mg (3). Positron emission tomography imaging to assess AR blockade showed decreased 18-fluorodihydrotestosterone binding at dosages of 60 mg/day and above, well below the approved dose of 160 mg. Antitumor effects were observed at all dosages, including declines in serum PSA of 50% or more in 56% of patients, responses in soft tissue, stabilized bone disease, and conversion from unfavorable to favorable circulating tumor cell counts. The median time to progression was 47 weeks for radiological progression in this population. Only 1 of the 87 patients (1%) treated at 240 mg or below had to discontinue treatment for an AE. There were two witnessed seizures at 360 and 600 mg/day and one possible seizure at 480 mg/day. There was an increased frequency of grade 3 fatigue at 360 mg and 480 mg/day (which generally resolved following dose reduction). The maximum tolerated dose was established as 240 mg/day.
The durability of disease suppression was similar between the 150 mg/day and the 240 mg/day dose cohorts in postchemotherapy patients in this phase I–II study. Given this comparable efficacy, the dose-dependent increases in grade 3 fatigue (0% at 150 mg/day versus 9% at 240 mg/day) and reports of seizure at the higher doses, a dose of 160 mg/day was thought to have the optimal risk/benefit profile and was selected for investigation in the randomized phase III AFFIRM trial (a study evaluating the efficacy and safety of the investigational drug enzalutamide).
AFFIRM: a randomized phase III study of enzalutamide in postchemotherapy metastatic castrate-resistant prostate cancer
AFFIRM study design and patient population
The international randomized phase III AFFIRM trial was conducted in 15 countries at 156 sites [Scher et al. 2012]. A total of 1199 patients with progressive mCRPC were randomized in a 2:1 manner to enzalutamide 160 mg daily (n = 800) or placebo (n = 399) (Figure 2) [Scher et al. 2012]. Patients were treated until disease progression. Patients with a history of seizure, taking medicines known to decrease the seizure threshold, or with other risk factors for seizure were not eligible. The use of prednisone or other glucocorticoids was permitted but not required, and the study drug was given without regard to food intake. Overall, 47.6% of patients in the enzalutamide arm and 44.6% in the placebo arm received corticosteroids during the study. The primary endpoint was OS, with secondary endpoints as shown in Figure 2. Patient characteristics were well balanced for both treatment arms [Scher et al. 2012]. The median age of patients was 69 years in both treatment arms. Overall, approximately one-quarter of patients were 75 years or older (enzalutamide 24.9%, placebo 26.1%). The interval from the time of first diagnosis to enrollment in AFFIRM was a median of 6 years. Almost 92% of patients in each arm had an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1. All patients had received prior docetaxel and the vast majority of patients received one (72.4% and 74.2%) or two (24.5% and 23.8%) prior lines of chemotherapy treatment in the enzalutamide and placebo arms respectively. Approximately 43% of all patients had received prior bisphosphonate therapy.

AFFIRM trial schema. mCRPC, metastatic castrate-resistant prostate cancer; PFS, progression-free survival; PSA, prostate-specific antigen; QOL, quality of life.
AFFIRM efficacy
A planned interim analysis demonstrated a significant improvement in the primary endpoint of OS. Median OS was 18.4 months among patients receiving enzalutamide and 13.6 months among patients receiving placebo, an incremental benefit of 4.8 months (Figure 3) [Scher et al. 2012]. The hazard ratio for death was 0.63 (p < 0.001), indicating there was a 37% decrease in the risk of death compared with placebo. On the basis of these results, the independent data and safety monitoring committee recommended that the AFFIRM study be halted and unblinded and eligible patients in the placebo arm were offered treatment with enzalutamide. In the intention-to-treat population, 308 of 800 patients (39%) died in the enzalutamide arm and 212 of 399 patients (53%) died in the placebo arm.

Kaplan–Meier estimates of overall survival in the AFFIRM study.HR, hazard ratio; OS, overall survival.
Consistent with the significant and clinically meaningful improvement in median OS reported in the overall population, the survival benefit was maintained across all patient subgroups, including age, baseline ECOG performance status, baseline pain intensity, geographic region, and type of disease progression at entry (Figure 4). The effect of enzalutamide on OS was maintained after adjustment for stratification factors and baseline prognostic factors (hazard ratio for death 0.58; p < 0.001).

Subgroup analyses of hazard ratios for death in the two treatment arms of the AFFIRM study. BPI-SF, brief pain inventory -short form; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; LDH, lactate dehydrogenase; OS, overall survival; PSA, prostate-specific antigen.
The superiority of enzalutamide over placebo was further shown for all secondary endpoints, including the time to PSA progression [8.3 versus 3.0 months; hazard ratio 0.25; p < 0.001; Figure 5(a)] and rPFS [8.3 versus 2.9 months; hazard ratio 0.40; p < 0.001; Figure 5(b)]. Additionally, when comparing enzalutamide and placebo, PSA-level response rate (54% versus 2%, p < 0.001), soft-tissue response rate (29% versus 4%, p < 0.001), Functional Assessment of Cancer Therapy -Prostate questionnaire ( FACT-P) quality-of-life response (43% versus 18%, p < 0.001), and the time to the first skeletal-related event (16.7 versus 13.3 months; hazard ratio 0.69; p < 0.001) were all significantly improved (Table 2).

Kaplan–Meier estimates of (a) time to PSA progression and (b) radiographic PFS in the AFFIRM study. PFS, progression-free survival’ PSA, prostate-specific antigen.
Additional secondary endpoints related to response and disease progression in the AFFIRM study.

PSA, prostate-specific antigen.
AFFIRM safety
Overall, enzalutamide 160 mg orally daily was well tolerated by patients compared with the placebo control. Although the period of observation for the enzalutamide arm was more than twice that for the placebo group, the rates of AEs were similar in the two treatment arms (Table 3) [Scher et al. 2012]. The enzalutamide arm had a lower incidence of AEs of grade 3 or above (45.3% versus 53.1% for placebo). The median time to the first such AE was 12.6 months with enzalutamide compared with 4.2 months in the placebo arm [Scher et al. 2012]. Overall there was a higher incidence of all grades of fatigue, diarrhea, hot flashes, musculoskeletal pain, and headache in the enzalutamide arm compared with placebo. Cardiac disorders were noted in 6% of patients receiving enzalutamide and in 8% of patients receiving placebo (with cardiac disorders of grade 3 in 1% and 2% respectively). Hypertension or increased blood pressure was observed in 6.6% of patients in the enzalutamide group and 3.3% in the placebo group.
The incidence (%) of select adverse events by treatment arm in the AFFIRM study.
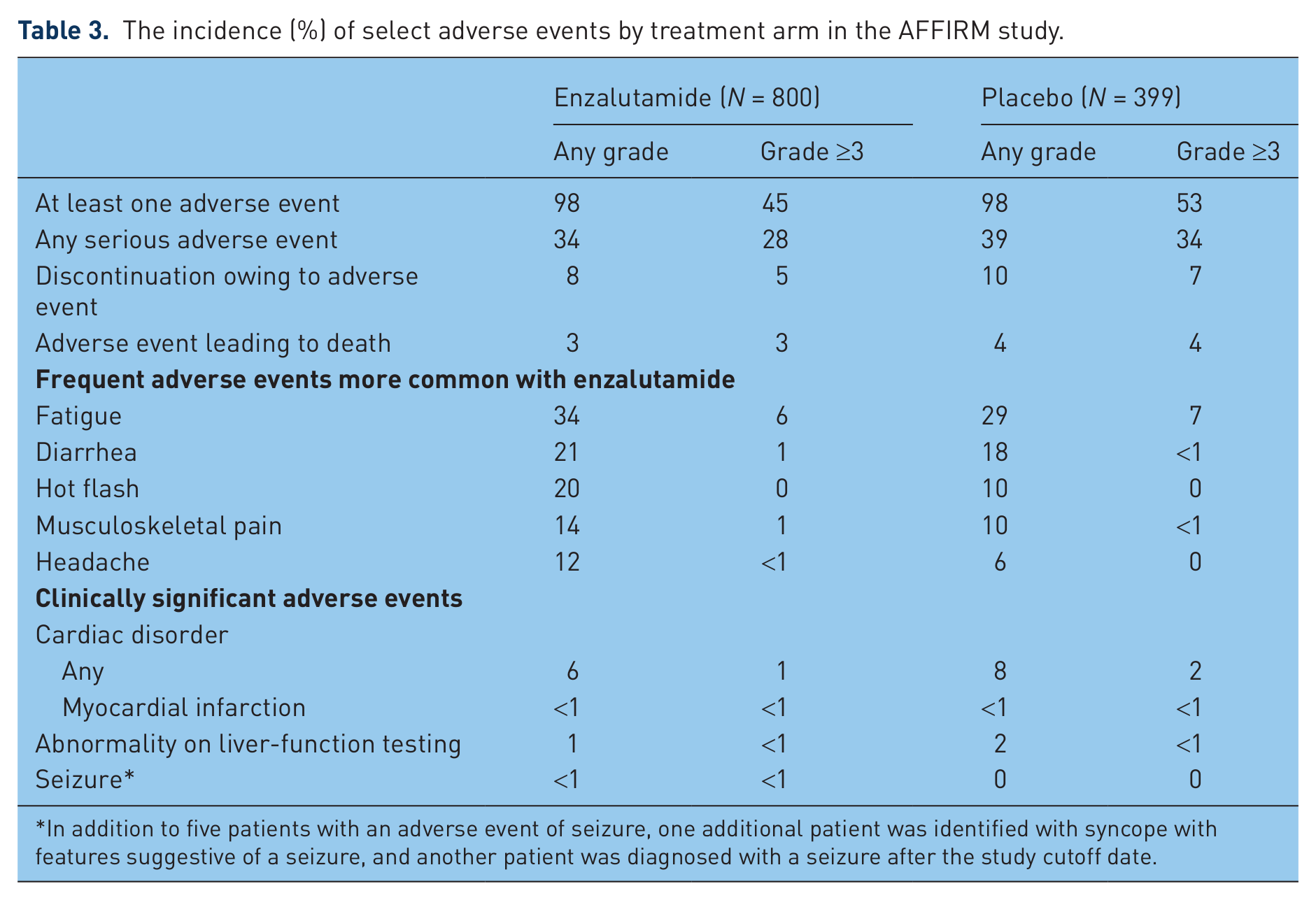
In addition to five patients with an adverse event of seizure, one additional patient was identified with syncope with features suggestive of a seizure, and another patient was diagnosed with a seizure after the study cutoff date.
There were no significant between study arm imbalances in the rates of hyperglycemia, weight gain, hyperlipidemia, or glucose intolerance. Thus, there was no evidence to suggest the development of a metabolic syndrome associated with enzalutamide; however, the AFFIRM study was not designed to formally evaluate this event. Liver function abnormalities were reported as AEs in 1% of patients receiving enzalutamide and in 2% of those receiving placebo.
At the time of data cutoff, five of the 800 patients (0.6%) in the enzalutamide arm were reported by the investigators to have had a seizure; no seizures were reported in the placebo arm until the data cutoff for analysis. One seizure case required medical intervention and four other seizures were self-limited and did not recur after study drug discontinuation. Potentially predisposing factors were present in several patients, including two patients with brain metastases, one of whom had a seizure reported 26 days after the last dose of enzalutamide. In addition to the five patients with an AE of seizure, one additional patient was identified with syncope with features suggestive of a seizure, and another patient was diagnosed with a seizure after the study cutoff date [Sternberg et al. 2013].
Discussion
The phase III AFFIRM trial demonstrated that enzalutamide significantly improved OS in men with mCRPC who had progressed in their disease after prior treatment with docetaxel chemotherapy. The incremental survival benefit of 4.8 months is the largest OS benefit ever recorded in a postchemotherapy setting for mCRPC and compares favorably with other agents. The hazard ratio of 0.63 translates into a 37% reduction in the risk of death in favor of enzalutamide. The survival benefit was observed across all patient subgroups analyzed. Further, enzalutamide also resulted in significant improvement in all secondary endpoints, including time to PSA progression, rPFS, and PSA response.
Enzalutamide was well tolerated with the exception of increased rates of all grades of fatigue, diarrhea, hot flashes, musculoskeletal pain, and headache compared with placebo. The rates of serious AEs were lower in the enzalutamide arm compared with the placebo group. The median time to experiencing an initial AE of grade 3 or higher was 8.4 months longer in the enzalutamide arm compared with placebo, presumably due to better control of their disease-related symptoms. Seizures occurred at a rate of less than 1% with enzalutamide but remain a concern. Enzalutamide does not have the side effects of chemotherapy, and benefits patients in several ways, including improvement of pain, activity level, prevention of bone-related complications, and resulting in improved quality of life and OS. Unlike other approved agents in the postdocetaxel setting, an important advantage is that steroid coadministration is not required with enzalutamide, and this may be of benefit for patients since this class of agents have their own side effects, including mild immunosuppression, loss of muscle mass and bone, as well as risk of hyperglycemia [Dorff and Crawford, 2013].
The extent of the quality of life improvement demonstrated in AFFIRM, along with the significant survival advantage, suggest that enzalutamide confers a significant and meaningful clinical benefit to men with mCRPC. These results establish enzalutamide as a standard of care treatment for patients whose disease has progressed after treatment with hormones and chemotherapy.
The results of the AFFIRM trial are also important with regard to the biology of the disease because they validate the rational drug design of enzalutamide and provide evidence that the AR remains active in patients with mCRPC who have castrate levels of testosterone, indicating that their tumors are not refractory to hormone therapy.
Current approaches to treatment of mCRPC are to delay or replace treatment with cytotoxic agents such as docetaxel and cabazitaxel with more efficacious and tolerable agents. A recent randomized phase III trial compared abiraterone plus prednisone with placebo plus prednisone in 1088 patients with mCRPC who were chemotherapy naïve [Ryan et al. 2013; Rathkopf et al. 2013]. The study was unblinded after a planned interim analysis when significant improvements were shown in the coprimary endpoints of rPFS and OS. The median rPFS was 16.5 months with abiraterone–prednisone and 8.3 months with placebo–prednisone (hazard ratio 0.53; p < 0.001) [Ryan et al. 2013]. Updated OS results showed a nonstatistically significant trend toward improvement with abiraterone–prednisone, with medians of 35.3 versus 30.1 months for prednisone alone (hazard ratio 0.79; p = 0.0151), as it did not reach the prespecified efficacy boundary [Rathkopf et al. 2013]. Abiraterone–prednisone showed superiority over placebo–prednisone alone with respect to time to initiation of cytotoxic chemotherapy (26.5 versus 16.8 months (hazard ratio 0.61; p < 0.0001). It is in this same chemotherapy-naïve setting that the ongoing randomized phase III PREVAIL trial will compare the efficacy and safety of enzalutamide with placebo in 1680 patients with progressive metastatic prostate cancer whose condition has failed to respond to androgen deprivation therapy but who have not yet received chemotherapy [ClinicalTrials.gov identifier: NCT01212991]. The coprimary endpoints in this trial are OS and rPFS. The current role and sequencing of enzalutamide may change based on the results of PREVAIL and other planned studies to assess relevant combinations (i.e. enzalutamide with abiraterone).
Additional ongoing clinical investigation includes two trials comparing enzalutamide with bicalutamide, the leading antiandrogen used in the treatment of patients with castrate-resistant prostate cancer before chemotherapy. The phase II TERRAIN and STRIVE studies are randomized, double-blind trials of enzalutamide head to head against bicalutamide, with a primary endpoint of PFS [ClinicalTrials.gov identifier: NCT01288911; NCT01664923] The trials differ in that TERRAIN is enrolling only patients with metastatic disease and is being conducted primarily in Canada and Europe, while STRIVE is enrolling patients with and without metastatic disease and is being conducted in the United States.
With its significant survival benefit and tolerable safety profile, combined with the convenience of oral administration with or without food, and no requirement for steroids or premedication, enzalutamide is an important addition to the treatment armamentarium of physicians for both young and older patients with mCRPC.
Footnotes
Funding
Enzalutamide is being codeveloped by Medivation, Inc. and Astellas. Funding for third-party editorial assistance by Eolas Communications for this publication was provided by both companies.
Conflict of interest statement
The author declares that there is no conflict of interest.