
Abstract
Objectives:
Two innovative pharmaceutical forms of leuprorelin acetate have been developed as 1-month and 3-month implants for the treatment of advanced hormone-dependent prostate cancer. These products contain active substance dispersed homogeneously in a biodegradable polymer. Here we present the key results from the clinical development of these slow-release implant formulations of leuprorelin.
Methods:
Two therapeutic studies of the 1-month implant were performed: a randomized, controlled study comparing the leuprorelin implant with leuprorelin prolonged-release microspheres (Enantone) as the active control; and a single-arm study of the leuprorelin implant. For the 3-month implant, four therapeutic studies were performed: a randomized, controlled study comparing the leuprorelin implant with leuprorelin prolonged-release microspheres (Trenantone) as the active control; a single-arm study of the leuprorelin implant; and two long-term studies with the 3-month implant administered twice, either 12 or 16 weeks apart. A pooled analysis of data from the comparator-controlled and single-arm studies of the 3-month implant was also conducted. The main inclusion criterion for all studies was histologically confirmed advanced prostate cancer, with primary endpoints based around successful testosterone suppression (≤0.5 ng/ml).
Results:
In the comparator-controlled studies, both implants were as effective as the microspheres for achieving successful testosterone suppression and normalization of prostate-specific antigen (PSA) levels. Data from the single-arm and long-term studies were consistent with those from the comparator-controlled studies. In the pooled analysis, significantly more patients treated with the 3-month implant achieved successful testosterone suppression compared with the comparator (p ≤ 0.01). The safety profile of the implants in the comparator-controlled studies was similar to that of the prolonged-release microsphere formulation, and consistent with that of the luteinizing hormone-releasing hormone agonist class.
Conclusions:
The innovative 1-month and 3-month implants of leuprorelin acetate are at least as effective as leuprorelin acetate prolonged-release microspheres for achieving successful testosterone suppression and normalization of PSA in men with advanced hormone-dependent prostate cancer, with a comparable safety profile.
Introduction
Prostate cancer is the second most frequently diagnosed cancer and the sixth leading cause of cancer death among men globally [Jemal et al. 2011]. In 2008, the estimated number of new prostate cancer cases worldwide was almost 900,000; this burden is expected to increase to 1.7 million by 2030 due to the growth and aging of the global population [Ferlay et al. 2010]. According to international guidelines, androgen deprivation therapy (ADT) is the mainstay of treatment for advanced hormone-dependent prostate cancer [Heidenreich et al. 2012]. Luteinizing hormone-releasing hormone (LHRH) agonists have been used in advanced prostate cancer for a number of years and are currently the main forms of ADT [Heidenreich et al. 2012; McLeod, 2003]. These agents are synthetic analogues of LHRH that are generally administered as depot injections [Heidenreich et al. 2012]. They initially stimulate pituitary LHRH receptors, inducing a transient rise in luteinizing hormone (LH) and follicle-stimulating hormone (FSH) release that in turn elevates testosterone production. With chronic exposure to LHRH agonists, LHRH receptors are downregulated, secretion of LH and FSH is suppressed, and testosterone levels are reduced to castration levels within 2–4 weeks [Limonta et al. 2001].
Two innovative slow-release forms of leuprorelin acetate (a 1-month and 3-month implant; developed by Sandoz/Hexal, Holzkirchen, Germany) were first approved for clinical use in 2007, and are currently available in 20 countries. The products are rod-shaped implants in which the active substance is dispersed homogeneously in a biodegradable polymer comprising lactic acid and glycolic acid (1-month implant) or lactic acid alone (3-month implant). The implants are inserted by subcutaneous injection into the anterior abdominal wall, where they are hydrolytically degraded to release the active substance. Potential benefits compared with other available leuprorelin products are that the implants are supplied ready to use, with no reconstitution required, and are also convenient to store given that no refrigeration is needed. In addition, compared with LHRH agonists more generally the implants may represent a more affordable option with the potential to expand patient access to treatment. This article presents the key results from the clinical development of these innovative formulations of leuprorelin in patients with advanced hormone-dependent prostate cancer. Data are included from two studies of the 1-month implant and four studies of the 3-month implant.
Methods
Study populations
All studies were conducted according to the Declaration of Helsinki and Good Clinical Practice guidelines and approved by the relevant ethics committees. Inclusion and exclusion criteria were similar for all studies; the main criteria are shown in Table 1.
Main inclusion and exclusion criteria.

One-month implant: study designs
Two therapeutic studies of the 1-month implant were performed: a randomized, controlled study comparing the leuprorelin implant with leuprorelin prolonged-release microspheres as the active control; and a single-arm study of the leuprorelin implant. The leuprorelin implant (3.6 mg leuprorelin, equivalent to 3.78 mg leuprorelin acetate) or suspended leuprorelin prolonged-release microspheres (Enantone, Takeda Pharma GmbH, Aachen, Germany; 3.57 mg leuprorelin, equivalent to 3.75 mg leuprorelin acetate) were administered subcutaneously into the abdominal wall by a physician. In both studies, treatments were administered four times at 4-week intervals.
Testosterone levels were measured at each visit (once-weekly up to the end of the studies) and prostate-specific antigen (PSA) levels were determined every 4 weeks. The primary endpoints were the proportion of patients with successful testosterone suppression, defined as a testosterone concentration of ≤ 0.5 ng/ml at a minimum of two consecutive time points within 8 weeks after the first administration of leuprorelin and continuing thereafter up to 8 weeks after the first administration; and the proportion of patients with successful testosterone suppression up to week 16. Data were evaluated using descriptive statistics, stating absolute and relative frequencies and the lower bound of the 95% confidence interval (CI), based on a binomial distribution.
Three-month implant: study designs
Four therapeutic studies of the 3-month implant were performed: a randomized, controlled, single-dose study comparing the leuprorelin implant with leuprorelin prolonged-release microspheres as the active control; a single-arm, single-dose study of the leuprorelin implant; and two long-term studies with the 3-month implant administered twice, either 12 or 16 weeks apart. The leuprorelin implant (5 mg leuprorelin, equivalent to 5.25 mg leuprorelin acetate) or suspended leuprorelin prolonged-release microspheres (Trenantone, Takeda Pharma GmbH; 10.72 mg leuprorelin, equivalent to 11.25 mg leuprorelin acetate) were administered subcutaneously into the abdominal wall by a physician. In the long-term studies, a second leuprorelin implant was administered after 12 or 16 weeks.
Testosterone levels were measured at each visit (daily measurements for the first 10 days, then once weekly up to the end of the studies), and PSA levels were determined every 4–8 weeks. The primary endpoints in the single-dose studies were: the proportion of patients with successful testosterone suppression, defined as a testosterone concentration of ≤ 0.5 ng/ml at a minimum of two consecutive time points within 8 weeks after the first administration of leuprorelin and continuing thereafter up to 8 weeks after administration; the proportion of patients with successful testosterone suppression up to week 12. In the long-term studies, the primary endpoint was the proportion of patients with successful testosterone suppression within and up to 8 weeks and up to week 24 (12-week administration interval) or week 32 (16-week interval). Data were evaluated using descriptive statistics, stating absolute and relative frequencies and the lower bound of the 95% CI, based on a binomial distribution.
The designs of the comparator-controlled and single-arm studies were similar (e.g. eligibility criteria, treatment duration), allowing a pooled analysis of data from these studies. Comparisons between the treatments were made using Fisher’s exact test.
Results
One-month implant studies
Patient demographics and baseline characteristics for the studies of the 1-month implant are shown in Table 2. In the comparator-controlled study, patient demographics and baseline characteristics were generally similar between the treatment arms; an exception was PSA level, which was higher in the 1-month implant group (median 47.4 ng/ml) than the comparator group (median 20.6 ng/ml), suggesting more severe disease in the implant group.
Patient demographics and baseline characteristics (1-month implant studies).

Data expressed as mean (SD) except for PSA (median values shown) and no. of patients. BMI, body mass index; G1, tumor well differentiated; G2, tumor moderately differentiated; G3, tumor poorly differentiated; G4, tumor undifferentiated; GX, grade not determinable; PSA, prostate-specific antigen.
Figure 1 shows the concentration–time profile for serum testosterone in the comparator-controlled study. At week 8, successful testosterone suppression was achieved in 96% of patients in the 1-month implant group and 86% of those who received microspheres (Table 3). Successful suppression persisted 16 weeks after first administration in 85% and 79% of patients treated with the implant and microspheres, respectively. In both groups, PSA levels decreased substantially until 4 weeks after treatment initiation; thereafter, PSA values remained ≤ 4 ng/ml (normal value) in most patients for the period 8–16 weeks after treatment initiation.

Concentration–time profile for serum testosterone in the 1-month implant comparator-controlled study.
Successful testosterone suppression in the comparator-controlled study of the leuprorelin 1-month implant.

N=number of patients in the per-protocol evaluation; n=number of patients with successful testosterone suppression.
LB 95% CI= lower bound of the 95% confidence interval.
Data from the single-arm study were consistent with those from the comparator-controlled study; all 20 patients achieved successful testosterone suppression at both 8 and 16 weeks after treatment initiation, and 90% (18/20) had a PSA level ≤ 4 ng/ml at the end of the study.
Three-month implant studies
Table 4 shows patient demographics and baseline characteristics for the studies of the 3-month implant. In the comparator-controlled study, these were generally similar between the treatment arms, except for PSA level. This was higher in the 3-month implant group (median 40.1 ng/ml) than in the comparator group (median 20.6 ng/ml), pointing to more severe disease in the implant group.
Patient demographics and baseline characteristics (3-month implant studies).

Data expressed as mean (SD) except for PSA (median values shown) and no. of patients. BMI, body mass index; G1, tumor well differentiated; G2, tumor moderately differentiated; G3, tumor poorly differentiated; G4, tumor undifferentiated; GX, grade not determinable; PSA, prostate-specific antigen.
Figure 2 shows the concentration–time profile for serum testosterone in the comparator-controlled study. At week 8, successful testosterone suppression was achieved in 97% of patients in the implant group and 81% of those who received the microsphere product (Table 5). Successful suppression was sustained for 12 weeks in 97% and 16 weeks in 90% of implant patients; corresponding values for the microsphere group were 81% and 73%. In both groups, PSA levels decreased markedly until 4 weeks after treatment initiation; thereafter, PSA values remained ≤ 4 ng/ml in most patients for the period 8–16 weeks after treatment initiation.

Concentration–time profile for serum testosterone in the 3-month implant comparator-controlled study.
Successful testosterone suppression in the comparator-controlled study of the leuprorelin 3-month implant.

N=number of patients in the per-protocol evaluation; n=number of patients with successful testosterone suppression.
LB 95% CI= lower bound of the 95% confidence interval.
Data from the single-arm and long-term studies were consistent with those from the comparator-controlled study. In the single-arm study, all 32 patients achieved successful testosterone suppression at weeks 8, 12 and 16 after treatment initiation; additionally, 86% of patients had a PSA level ≤ 4 ng/ml at week 16. In the study of a 12-week administration interval, 100% of patients analysed had achieved successful testosterone suppression after 8 weeks. At 12 and 24 weeks, the success rate was 93%. In the study of a 16-week administration interval, 100% of patients analysed had achieved successful testosterone suppression after 8, 16 and 32 weeks; in addition, 93% of patients had a PSA level ≤ 4 ng/ml at week 32.
Data from the pooled analysis of the comparator-controlled and single-arm studies with the 3-month implant are shown in Figure 3. At the 8-, 12- and 16-week timepoints, significantly more patients treated with the leuprorelin 3-month implant achieved successful testosterone suppression compared with those treated with the microspheres (all p ≤ 0.01).
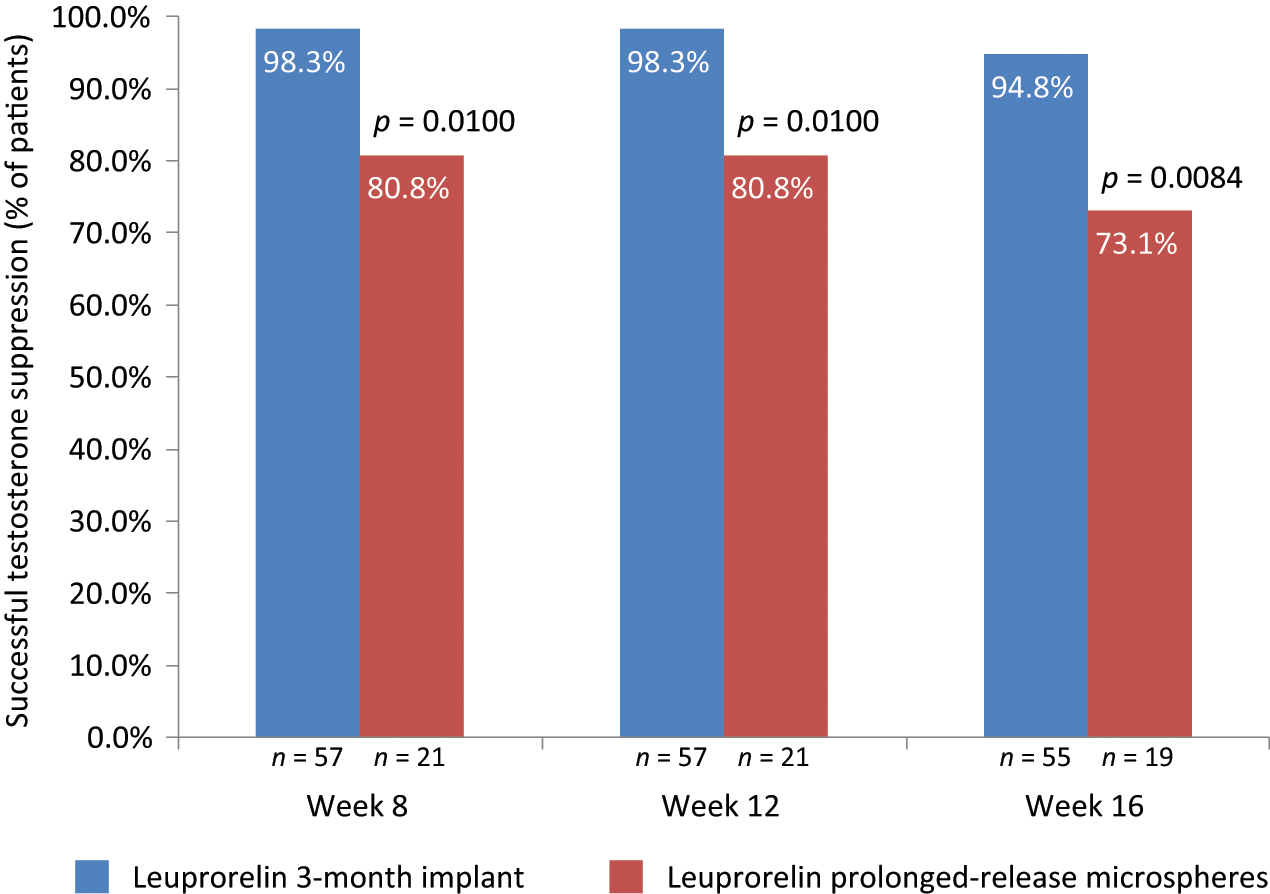
Successful testosterone suppression in a pooled analysis of the 3-month implant comparator-controlled and single-dose studies.
Safety and tolerability
In the comparator-controlled study of the 1-month implant, adverse events (AEs) were reported in eight patients (15 events) in the implant group and nine patients (11 events) in the microspheres group. No patient withdrew from the study due to AEs. The most common treatment-emergent AEs (each occurring in at least two patients in either treatment group) were hot flushes (1-month implant group, n = 2; microspheres group, n = 3), hypertension (1-month implant group, n = 2; microspheres group, none), urinary retention (1-month implant group, n = 2; microspheres group, none) and urinary tract infections (1-month implant group none; microspheres group, n = 2). No injection-site reactions were reported in either group. Serious AEs were reported for one patient in each treatment group; a patient in the implant group died as a result of pneumonia and heart failure, and a patient in the microspheres group was hospitalized for pneumonia. Both cases were deemed to be unrelated to study treatment.
In the comparator-controlled study of the 3-month implant, AEs were reported in 14 patients (22 events) in the implant group and 10 patients (22 events) in the microspheres group. No patient withdrew from the study due to AEs. The most common treatment-emergent AEs (occurring in two or more patients in either treatment group) were hot flushes (3-month implant group, n = 2; microspheres group, n = 1), bone metastases (3-month implant group, n = 1; microspheres group, n = 2), dysuria (3-month implant group, n = 1; microspheres group, n = 2), sleep disorders (3-month implant group, n = 2; microspheres group, none), fever (3-month implant group, n = 2; microspheres group, none) and nocturia (3-month implant group, none; microspheres group, n = 2). Injection-site reactions were reported in two patients in the comparator group (none in the 3-month implant group), while flare symptoms requiring antiandrogen treatment occurred in two patients in each group. Three deaths occurred during the study, one in the 3-month implant group (aneurysm) and two in the comparator group (pneumonia, bone metastases). None of these events was considered related to study treatment.
In both comparator-controlled studies, the tolerability of the implant and prolonged-release microspheres was rated as good/very good by all physicians and patients, using a five-point scale (very good, good, indifferent, bad, very bad).
Discussion
This clinical development program has confirmed the efficacy of two innovative pharmaceutical forms of leuprorelin acetate for the treatment of hormone-sensitive advanced prostate cancer. Both the 1-month and 3-month implants of leuprorelin acetate demonstrated similar efficacy to a comparator formulation, based on prolonged-release microspheres, in achieving successful testosterone suppression and normalization of PSA levels. In the case of the 3-month implant, data from a pooled analysis of two studies (one comparator controlled and one single arm) suggests superior testosterone suppression with the implant formulation compared with leuprorelin acetate prolonged-release microspheres (Trenantone).
The safety and tolerability profile of the leuprorelin implants was similar to that of the prolonged-release microsphere formulation, and generally consistent with that of the LHRH agonist class. While other implant forms of LHRH agonists may result in substantial (albeit tolerable) pain on injection in some patients [Kinoshita et al. 2010], very few injection-site reactions were recorded in the comparator-controlled studies reported here. Further evidence for the good tolerability of the leuprorelin implants is available from two large post-marketing surveillance studies. In the first of these, 1148 patients with advanced hormone-dependent prostate cancer were treated with three injections of the 3-month implant [Thyroff-Friesinger et al. 2012a]; 98% of patients assessed the tolerability of the implant as very good/good/satisfactory. The second study assessed 818 patients with advanced hormone-dependent prostate cancer who were treated with three injections of either the 1-month or 3-month implant; while injection-site pain was one of the most frequently reported AEs during the course of treatment, both physicians and patients rated the tolerability of the implants as very good or good in more than 90% of cases (Sandoz data on file; manuscript in preparation).
Efficacy data in this report are based on a castrate testosterone level of ≤ 0.5 ng/ml. While this was widely considered the standard level when the studies were conducted several years ago, newer technology based on chemiluminescence suggests that the mean value of testosterone after surgical castration is 0.15 ng/ml [Oefelein et al. 2000]. This has led to suggestions that the castrate testosterone level should be redefined as less than 0.2 ng/ml [Zlotta and Debruyne, 2005]. However, limited information exists on whether applying this lower level of castrate testosterone is associated with better clinical outcomes than a level of ≤ 0.5 ng/ml, which remains the standard level in international clinical guidelines [Heidenreich et al. 2012].
The dimensions of both the 1-month and 3-month implant are approximately 10 mm in length and 1.5 mm in diameter. The 1-month implant is a polymer of lactic acid and glycolic acid (1:1), while the 3-month implant is polylactic acid. Similar polymers have been used in medicine for many years in the form of surgical suture materials, suture clips, screws and stents.
The 3-month leuprorelin implant contains 5 mg of active substance, which is less than half the amount in the comparator product (e.g. Trenantone prolonged-release microspheres, 10.72 mg leuprorelin). In dose-finding studies, a dose of 5 mg was found to be as effective as 10 mg for achieving castrate testosterone levels (unpublished results), therefore 5 mg was selected as the dose to be developed as a 3-month implant. In the comparator-controlled study of the 3-month implant, the maximum serum concentration of leuprorelin was higher for prolonged-release microspheres than for the 3-month implant up to 24 h after administration. After this time point, however, more leuprorelin was released from the implant than from the microspheres during the course of the study [Thyroff-Friesinger et al. 2012b]. Leuprorelin from the 3-month implant has an approximately fourfold higher bioavailability than in the prolonged-release microspheres; this explains why the 3-month implant formulation is at least as effective in achieving successful testosterone suppression despite containing less than half the amount of active substance.
In conclusion, the innovative implant forms of leuprorelin acetate are at least as effective as leuprorelin acetate prolonged-release microspheres for achieving successful testosterone suppression and PSA normalization in men with advanced hormone-dependent prostate cancer, with a comparable safety profile.
Footnotes
Acknowledgements
Medical writing assistance in the preparation of this paper was provided by Tony Reardon of Spirit Medical Communications Ltd and funded by Sandoz International GmbH.
Funding
This study was funded by Sandoz International GmbH.
Conflict of interest statement
Goetz Geiges has received honoraria for speaking at Sandoz-sponsored events. Elisabeth Schapperer and Ursula Thyroff-Friesinger are employees of Hexal AG. Patricia Gravel has acted as a consultant to Sandoz.