
Abstract
The outcome of penile cancer is proportional to the stage at presentation. Strategies aimed at primary prevention would have a clear advantage, both for the individual and in terms of health economics. A number of preventative measures could be employed, including circumcision, smoking cessation, education on hygiene and human papillomavirus (HPV) prevention. There is a high prevalence of HPV infection associated with penile cancer worldwide. The recent development of HPV vaccines has facilitated interest in their use for the prevention of penile cancer. In this article we review the literature surrounding penile cancer prevention and HPV vaccination in men.
Introduction
Penile cancer is a rare malignancy. Wide variations are seen in its incidence, and global health burden, worldwide ranging from 0.1 to 0.9/100,000 men in Europe, where it accounts for approximately 1% of male malignancies, to as high as 4.4 or 4.2/100,000 men in Uganda and Paraguay where it accounts for up to 10% of male malignancies [Wabinga et al. 2000; Rubin et al. 2001]. A number of aetiological risk factors have been identified in penile cancer, including phimosis, chronic inflammation, poor hygiene, smoking, and human papillomavirus (HPV) infection (see Table 1). The differing prevalence of these factors worldwide may account for the geographical variations in incidence.
Risk of penile cancer associated with selected characteristics, stratified to circumcision status.

From Daling et al. [2005].
CI, confidence interval; OR, odds ratio.
The outcome of treatment for penile cancer directly correlates with the stage at presentation. Early identification and treatment may improve the chances for penile preservation, and ensure optimal oncological and functional outcomes. Strategies aimed at primary prevention, however, would have a clear advantage, both for the individual and in terms of health economics. A number of preventative measures can be employed, including circumcision, smoking cessation, education on hygiene and HPV prevention. There has been increasing interest in the latter given the high prevalence of HPV infection in penile cancer, seen in approximately 50% of cases worldwide, and the recent development of HPV vaccines. In this review we explore the issues surrounding penile cancer prevention and HPV vaccination in men.
Risk factors and prevention strategies
Phimosis, hygiene and circumcision
Globally it is estimated that 25% of men are circumcised, primarily for religious or cultural reasons [Moses et al. 1998]. Penile cancer is extremely rare in men who are circumcised at birth. A recent systematic review and meta-analysis examining the effect of circumcision on penile cancer has confirmed a beneficial effect if performed before 18 years of age [odds ratio (OR) 0.33; 95% confidence interval (CI) 0.13–0.83] compared with an increased risk of cancer if performed as an adult (OR 2.71; 95% CI 0.93–7.94) [Larke et al. 2011]. However, the protective effect of circumcision in the under 18 age group was no longer evident when analysis was restricted to boys with no history of phimosis, indicating that the beneficial effect of circumcision may be through the prevention of phimosis [Larke et al. 2011].
Phimosis has a strong association with the development of penile cancer (OR range 4.9–37.2; four studies) [Daling et al. 2005; Tseng et al. 2001; Brinton et al. 1991; Madsen et al. 2008]. This may be due to the underlying cause of the phimosis, such as chronic inflammation, or due to the resultant poor hygiene as a consequence of the inability to retract the foreskin. Lichen sclerosus (LS) is the most common chronic inflammatory cause of phimosis, and is frequently found in patients with invasive squamous cell carcinoma (SCC) of the penis, with reported rates between 28% and 50% [Pietrzak et al. 2006; Powel and Wojnarowska, 1999; Perceau et al. 2003]. This has led to the conclusion that LS represents a premalignant process. However, the development of new tumours on follow up of patients with LS is low (5.8%), with a long latency from onset of changes to invasive tumour of 17 years (range 10–24 years) [Nasca et al. 1999]. This suggests that LS is an associated risk factor, as opposed to a true premalignant condition. Due to the long latency period and low prevalence, it is not feasible or practical to follow up all patients with LS, but patients should be instructed on routine self-examination and have an early clinical review in the event of the development of any new changes.
There is very little evidence linking hygiene and penile cancer. Poor genital hygiene is commonly observed in uncircumcised (26%) compared with circumcised men (4%) [O’Farrell et al. 2003]. Previous held beliefs that retained smegma was carcinogenic have been largely discarded. However, the observation of falling rates of penile cancer in Denmark over a period when rates of circumcision remained stable have been attributed to improvements in hygiene and sanitation over the same period of time [Frisch et al. 2000]. Simple health education programs aimed at improving hygiene are simple to instigate, but their cost efficacy in terms of disease prevention would be difficult to evaluate given the uncertain aetiological role.
There has been a renewed interest in the primary preventative role of circumcision due to the observed 50–60% risk reduction of contracting HIV demonstrated in recent studies [Bailey et al. 2007; Gray et al. 2007]. Adopting a putative program of population-based circumcision in sub-Saharan countries where the incidence of HIV is high would have clear health benefits that outweigh the potential risk or cost. Circumcision has been shown to also significantly reduce the risk of developing HPV infection (OR 0.37; 95% CI 0.16–0.85) [Castellsagué et al. 2002]. However, despite the clear benefit, a similar putative population-based program would be hard to justify in terms of penile cancer prevention alone given the rarity of the condition. An argument for neonatal circumcision based on the potential benefits of decreasing HIV and HPV transmission, and its subsequent related pathology, in addition to preventing urinary tract infections, inflammatory penile dermatoses and penile cancer would be one potential model, although no economic evaluation of this approach has been formulated to date.
Smoking
There is a clear association between smoking or chewing tobacco and penile cancer [Harish and Ravi, 1995]. A dose-dependent relationship between tobacco use and the risk of penile cancer has been demonstrated, with an OR for active smokers of 2.3, and 1.9 for former smokers [Daling et al. 2005]. Current smokers were also shown to have a considerably increased OR (4.5) for developing invasive disease (see Table 2). Programs aimed at reducing smoking would therefore have the potential of reducing the risk of developing invasive penile cancer, in addition to the obvious health economic benefits on reducing the rate of other smoking-related conditions, including lung cancer, bladder cancer, cardiovascular and respiratory disease.
Risk of invasive penile cancer and in situ disease by smoking status.

From Daling et al. [2005].
CI, confidence interval; OR, odds ratio.
Human papillomavirus infection and penile cancer
HPV is an uncoated double-chain DNA virus. There are more than 100 known variants of HPV. Approximately 4% of all global cancers are attributable to the carcinogenic effects of HPV (see Table 3). Subtypes thought to confer a high risk of carcinogenesis include 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58 and 59. The intermediate-risk subtypes include 26, 53, 66, 73 and 82. The low-risk subtypes are 6, 11, 40, 42, 43, 44, 54, 61, 70, 72, and 81.
HPV infection-attributable cancer in 2002.
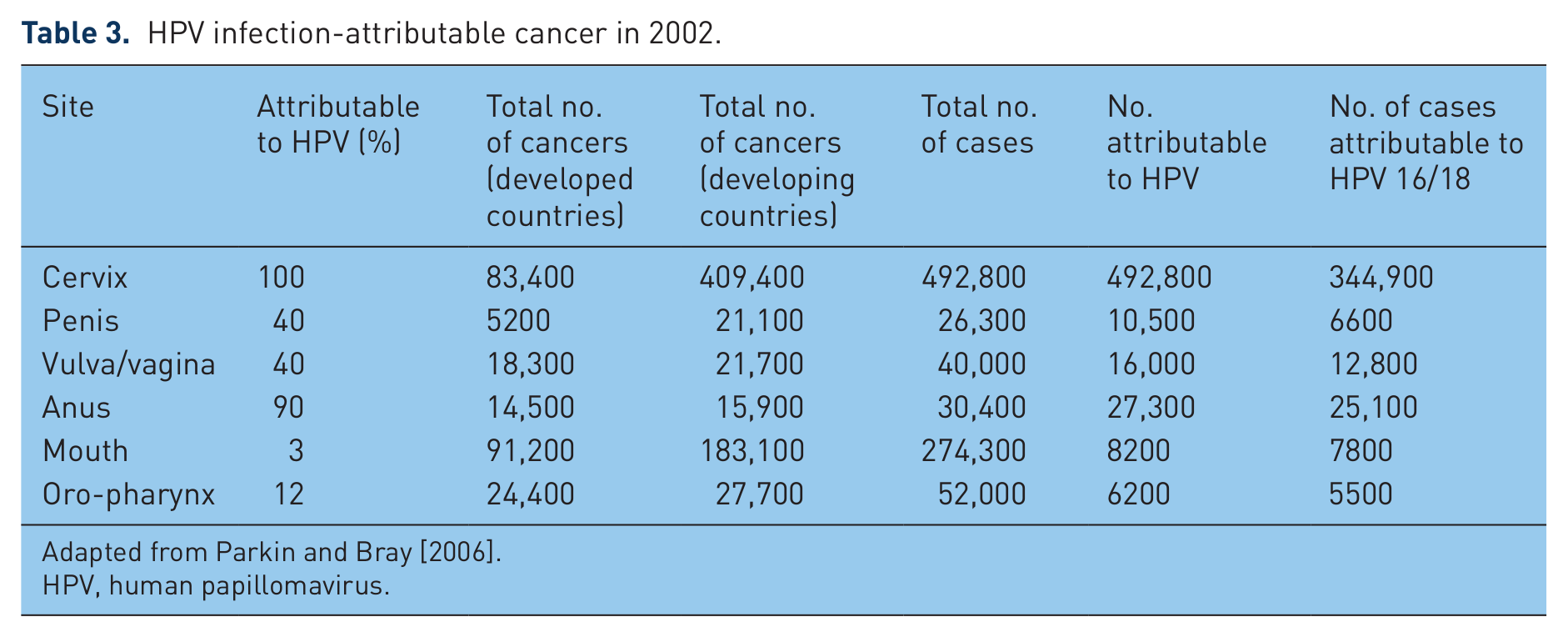
Adapted from Parkin and Bray [2006].
HPV, human papillomavirus.
The understanding of how HPV infection may lead to premalignant lesions and invasive tumours is based on studies of carcinogenesis in cervical cancer, in which almost 100% of cervical SCCs are related to sexually transmitted HPV infection. While HPV is also found in approximately 90% of anal cancers, 50% of vulval cancers, and approximately 10% of oropharyngeal cancers, reported rates of HPV infection in penile cancer have varied from 12% to 82% [Rubin et al. 2001; Gregoire et al. 1995; Bezerra et al. 2001; Iwasawa et al. 1993; Sarkar et al. 1992; Ambrosio et al. 2008]. The reasons for this wide range include geographical variations and different cultural attitudes towards sex between the reporting centres, as well as technical differences in the methodology used for HPV detection. Recent systematic reviews of established polymerase chain reaction techniques have found HPV DNA in approximately 50% of all penile SCCs [Backes et al. 2009].
The virus exerts its tumourgenic effect via expression of viral oncogenes E6 and E7, which inhibit the activity of tumour suppressor genes p53 and RB [McDougall, 1994]. The resultant deregulation of cell cycle control and apoptotic mechanisms results in malignant transformation to carcinoma in situ or invasive malignancy if left untreated [zur Hausen 2002]. The marked difference in the prevalence, age of peak incidence and rate of progression of both cervical and penile tumours may underlie either differing pathogenic mechanisms or differing tissue susceptibility and pathogenic response to the same HPV infection in these two malignancies. Whilst the cervical model of carcinogensis gives a good basis for tumour development and progression in penile cancer, it does not fully explain the complete pathogenesis. In this respect, penile cancer shares more common ground with vulval SCC, with similar rates of HPV infection, and an aetiological link to LS.
Several types of HPV have been identified in premalignant penile lesions. ‘High risk’ HPV types 16 and 18 are the most common, being found in 60–75% of HPV-related premalignant lesions, including Bowen’s disease, erythroplasia of Queyrat and Bowenoid papulosis [Heideman et al. 2007]. Low-risk HPV types 6 and 11 are associated with other premalignant lesions such as giant condylomata acuminata.
Not all invasive SCC subtypes have the same association with HPV infection. In a review of 200 cases, Cubilla and colleagues reported a preferential association of basaloid and warty-basaloid SCC subtypes with HPV infection in approximately 80% of cases, whilst no HPV was detected in verrucous, mixed verrucous–papillary, pseudohyperplastic, and pseudoglandular SCCs [Cubilla et al. 2010]. Lower rates of HPV DNA were detected in usual type (24%), sarcomatoid (17%), mixed (19%), and papillary not otherwise specified (15%) carcinomas. HPV-16 was the most commonly found genotype (72%) followed by HPV-6 (9%) and HPV-18 (6%). No specific correlation was found between HPV subtype and histological type of SCC, although usual type SCC had the greatest variety of HPV subtypes detected. In 6% of tumours, only low-risk HPV-6 and HPV-11 were found. Half were usual type, and the remainder were warty-basaloid type, underlining the invasive malignant potential of even ‘low-risk’ HPV lesions.
A significant association between HPV status and histological grade was also reported in this study, with 6% of grade 1, 21% of grade 2 and 53% of grade 3 tumours being HPV positive (p < 0.0001) [Cubilla et al. 2010]. This is in keeping with previous studies showing HPV DNA associated with higher grade and more aggressive penile tumours [Gregoire et al. 1995], and would suggest a detrimental prognostic effect of HPV-positive status. This would seem logical given its increased association with a basaloid subtype. However, no other study has been able to show any such correlation, with other retrospective reviews reporting no association between tumour grade, incidence of nodal involvement, or survival based on HPV status [Bezerra et al. 2001; Wiener et al. 1992].
HPV vaccines
Two HPV vaccines have been recently developed. A quadrivalent HPV vaccine Gardisil® (Merck Sharp & Dohme Corp., USA) targeting HPV-6/11/16/18, and a bivalent vaccine Cevarix® (GSK, USA) targeting high-risk HPV-16/18 only. Both are given on a three-dose schedule, with effective periods of protection of 5 and 6.4 years respectively post inoculation [Stanley, 2010]. Both have been shown to be safe and effective. For the bivalent vaccine, efficiency for prevention of HPV-16/18-related cervical intraepithelial neoplasia (CIN) was 98% [Paavonen et al. 2009]. For the quadrivalent vaccine, the efficacy for CIN was 100% for all four HPV subtypes, in addition to a 98.9% reported efficacy for prevention of HPV-6/11/16/18-related genital warts, and 100% efficacy for HPV-16/18-related vulval and vaginal intraepithelial neoplasia [Kjaer et al. 2009; Munoz et al. 2009].
Vaccination programs have been introduced in several countries over the last few years, aimed at primary prevention of cervical cancer, immunizing girls prior to first sexual contact. In the UK this began in 2008, using the bivalent vaccine in 12–13-year-old girls, with a catch-up program for girls up to the age of 18. The reported uptake was 76.4% for England and 86.9% for Scotland [Department of Health, 2011], although significantly lower uptake has been seen in other countries such as the Netherlands, where vaccine coverage only achieved 51.9% [Oomen et al. 2011]. The use of ‘female-only’ vaccination programs may confer some ‘herd immunity’ to the male population by reducing the burden of HPV in sexually active individuals. This has the potential advantage of reducing the risk of cross reinfection in the community, as well as providing some protection to men from HPV-related health problems. However, adopting a female-only approach has a number of downsides. First, herd immunity, while providing some benefit to the male population, will not give as complete coverage as vaccination aimed at both sexes. Second, vaccinating both sexes avoids stigmatization of HPV as a female-only issue in the general population. Finally, female-only vaccination does not provide herd immunity for men who have sex with men (MSM), a subgroup at higher risk of developing anal intraepithelial neoplasia (AIN) and anal cancer as a consequence of HPV exposure.
Evidence of the limitations of a herd immunity effect has been seen in Australia, where a national vaccination program using the quadrivalent vaccine was introduced for all women aged 12–26 in 2007. Coverage of 65.1% was achieved. After introduction of the vaccine, the rate of genital warts in women fell significantly by 59% (p < 0.0001). A 28% (p < 0.0001) fall in the number of genital warts in heterosexual men was also seen over the same period, demonstrating some herd immunity effect. However, no such change was seen in the MSM population [Donovan et al. 2011]. Given that the rate of HPV infections is similar in men and women, adopting an approach aimed at boys as well as girls, prior to first sexual contact, would therefore have an added advantage of preventing a greater number, and wider range, of HPV-related conditions, albeit at a greater total cost.
HPV vaccines have been shown to be clinically effective in men. In a recent randomized, multicentre, placebo-controlled, double-blind trial of 4065 men aged 16–26 years, vaccination using the quadrivalent vaccine effectively reduced the incidence of genital warts in 90% of patients with no HPV at enrolment [Giuliano et al. 2011]. Subgroup analysis of 602 MSM patients showed the quadrivalent vaccine was also able to reduce the incidence of HPV-6/11/16/18-related grade 2 or 3 AIN by 74.9% in those who had no HPV at enrolment. However, the efficacy of the vaccine at preventing penile intraepithelial neoplasia (peIN) or penile cancer could not be assessed given the low incidence of the disease in the study population (only four cases of PeIN and no cases of penile cancer in the entire study group) [Palefsky et al. 2011].
Cost efficacy of human papillomavirus vaccines
When deciding on the instigation of a national vaccination program, cost is a major consideration. In terms of female-only vaccination aimed at the prevention of cervical cancer, the cost/benefit analysis is well tipped in favour of vaccination, due to clear aetiological links to HPV infection, the ability of vaccination to effectively reduce the incidence of CIN, and the considerable global burden of the disease. When assessing the overall cost effectiveness of the vaccine, it is also important to take into account its wider-ranging effects and the potential noncervical benefits of any vaccination program. Figures from the USA in 2003 estimated the annual economic burden of noncervical HPV-6/11/16/18-related conditions to be US$418 million (range US$160 million to 1.6 billion) [Hu and Goldie, 2008]. The economic burden of these diseases is likely to have increased further over the last decade. A study from the Netherlands analysed the cost effectiveness of HPV vaccination for preventing cervical cancer alone compared with the cost effectiveness of preventing all HPV-16/18-related malignancies in women [de Kok et al. 2011]. They estimated that the additional noncervical benefits of vaccination would result in an increase in life years gained of 14%, with an additional cost saving of 18% and a reduction in the cost-effectiveness ratio of 13%.
The cost effectiveness of instigating a national vaccination program is unique to each individual country, and needs to take into account their incidence of HPV-related conditions, the prevalence of HPV infection, the cost of treatment compared with vaccination, as well as the likelihood that sufficient coverage will be achieved by vaccination to be effective. It may be that in some countries the low prevalence of HPV, or high cost of vaccination, may render a national program ineffective financially despite the potential public health benefit. In some countries such as the UK, a national program of vaccination in women was instigated in 2008 using the less costly bivalent vaccine. While this approach lowered the total cost for the program, it does not offer the same extent of cover provided by the quadrivalent vaccine, and would therefore be less effective at preventing the broader range of noncervical HPV-related conditions, such as anogenital warts, respiratory papillomatoses, anal cancer and head and neck cancers. Subsequent economic evaluation in the UK of both bivalent and quadrivalent vaccines has shown the latter to be more cost effective given its additional health benefits [Jit et al. 2011].
When extending the use of HPV vaccines to men, careful statistical modelling needs to be employed to ensure such an expensive strategy would be cost effective. In the USA, studies deigned to assess the public health impact and cost effectiveness of adding men aged 9–26 years to the existent female HPV vaccination programs found improved disease prevention in both sexes, with a direct effect on male HPV-related conditions as well as an additional indirect effect of female HPV-related illness. Extension of such national programs to the male population would increase the mean incremental cost-effectiveness ratio (ICER) from US$3282/quality-adjusted life year (QALY) to US$25,664/QALY, if one takes into account all the possible HPV-related conditions which may be prevented using the quadrivalent vaccine [Elbaha and Dasbach, 2010]. Although this is a substantial increase in the ICER, it is still substantially less than the commonly cited thresholds of US$100,000/QALY and US$50,000/QALY [Eichler et al. 2004]. The Advisory Committee on Immunizations Practices from the Centers for Disease Control and Prevention has recently changed its guidelines on immunization of boys and men in the USA. They recommend use of the quadrivalent vaccine in boys/men aged 13–22 who have not already been vaccinated. Men aged 22–26 may also be vaccinated. This was based on using models looking at all HPV-related disease in both men and women. It was particularly cost effective when uptake among girls/women is low, that is, less than 50% of the target population have been vaccinated; whereas it is less cost effective when uptake in girls/women is high, that is, over 70%. With increasing age at vaccination, the cost effectiveness reduces, with the QALYs for men over 21 years being two to four times that for boys/men under 18 years [Centers for Disease Control and Prevention, 2011].
When arguing the case for HPV vaccination specifically for the prevention of penile cancer in isolation, it is not possible to have the same clarity. Given the rarity of the disease, an aetiological role of HPV in only approximately 50% of cases, and uncertainty in the timescale of progression from HPV exposure to cancer, it is very difficult to assess the potential impact of vaccination on penile cancer. In their trial of the quadrivalent vaccine in approximately 4000 men, Palefsky and colleagues encountered no cases of penile cancer, and only four cases of PeIN [Palefsky et al. 2011].
Scenario planning and forecasting can be used as a possible means of strategic planning to assess the potential effect of modifying a risk factor on future outcome of a disease. An estimate of the impact of a vaccination program on the incidence of penile cancer in the UK can be forecast based on the age distribution of 100 consecutive cases [Hegarty et al. 2006] and using data of projected demographics from the Organisation for Economic Co-operation and Development (http://www.oecd.org/statsportal/). Assuming full vaccination uptake, and a resultant risk reduction of 50% in those receiving the vaccination, the predicted fall in the incidence of penile cancer is 5% by the year 2050, levelling off at 50% by 2090 (see Figure 1). Given this, a national vaccination program aimed solely at preventing HPV-related penile cancer alone is unlikely to be cost effective in the UK. In countries with a greater incidence of penile cancer and a greater prevalence of HPV infection, such as Brazil, there may be more of a role for male vaccination, although statistical modelling would be required to assess its cost effectiveness (prevalence 8.3/100,000 men in Brazil; reported HPV DNA rate 75%) [Scheiner et al. 2008]. However, if one takes into account the wider-ranging benefits of extending vaccination to men in terms of its effect on all HPV-related conditions and malignancies, the argument for introducing a program in both sexes is considerably strengthened in terms of public health benefit and cost efficacy.

Projected changes in overall incidence of penile cancer for a fixed population over the coming decades, with and without a male vaccination programme for human papillomavirus.
Summary
Strategies aimed at the primary prevention of penile cancer offer an opportunity to avoid the morbidity associated with the treatment of established disease. Education on the cessation of smoking, improved hygiene, sexual health, and the use of effective barrier contraception provides simple and achievable measures. While the instigation of routine neonatal circumcision would effectively reduce the incidence of penile cancer, the cost/benefit of such an approach for a rare disease is hard to justify in isolation.
HPV vaccination has been instigated for the primary prevention of cervical cancer and offers a tantalizing option for the primary prevention of penile cancer, especially in countries with a high incidence of penile cancer and a high prevalence of HPV. However, at present, male HPV vaccination solely for the purpose of penile cancer prevention cannot be recommended due to a lack of clear data able to directly demonstrate its benefit for penile cancer or PeIN. In terms of cost efficacy, male vaccination solely for the prevention of penile cancer would be untenable given the rarity of the disease. However, if one takes into account the wider ranging benefits of extending vaccination to men in terms of reducing the burden of other HPV-related conditions and malignancies, the argument for introducing a program in both sexes is considerably strengthened in terms of public health benefit and cost efficacy. As such, any beneficial effect of male vaccination on the prevention of penile cancer would be an added bonus rather than the main indication for extending the vaccination program to both sexes, with the preventative effects on more common diseases such as genital warts, anal cancer, and head and neck cancers taking a greater precedence in the decision-making process. As in the USA, a program of vaccination using the quadrivalent vaccine prior to first sexual contact would provide the most cost-effective approach.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.