
Abstract
Bone metastases in patients with genitourinary cancers are associated with increased risk for skeletal-related events including pathologic fractures, spinal cord compression, and the requirement for surgery or palliative radiotherapy to bone. The nitrogen-containing bisphosphonate zoledronic acid and the monoclonal antibody against RANK, denosumab, are approved for the prevention of skeletal-related events in genitourinary cancers. These agents have different mechanisms of action and pharmacokinetic profiles, and while both are effective in reducing the risk of skeletal-related events, other clinical effects differ. There is evidence for direct and indirect anticancer activity with zoledronic acid from preclinical studies and emerging data from clinical studies suggesting an effect on patient survival. Potential anticancer mechanisms include inhibition of angiogenesis, enhanced immune surveillance via stimulation of γδ T cells, and reduction of circulating tumor cells. A synergistic effect of chemotherapy plus zoledronic acid has also been suggested. Further research is ongoing regarding the roles of these antiresorptive therapies in patients with bone metastases or at high risk for malignant spread to skeletal sites.
Keywords
Introduction
Patients with genitourinary (GU) malignancies are at risk for deterioration of bone throughout the disease continuum as a result of treatment, underlying disease, or both [Coleman, 2001; Saad et al. 2006]. Androgen-deprivation therapy for prostate cancer is associated with decreased bone mineral density, increased risk for osteoporosis, and in one large meta-analysis, a 1.17-fold relative increase in the risk of skeletal fractures [Mittan et al. 2002; Serpa Neto et al. 2010]. Moreover, a significant proportion of patients with GU malignancies may develop metastatic skeletal involvement, further exacerbating loss of structural bone integrity [Coleman, 2001; Zekri et al. 2001; Woodward et al. 2011]. Bone metastases are associated with a vicious cycle of bone destruction and tumor growth. As a result, patients with bone metastases typically experience severe bone pain and are at high risk of developing potentially debilitating skeletal-related events (SREs) including pathological fractures or spinal cord compression that may require surgical or radiotherapy intervention [Coleman, 1997; Saad and Lipton, 2005]. Inevitably, SREs reduce a patient’s quality of life and functional independence, which are of particular relevance in patients who have a long life expectancy [Saad, 2008].
Antiresorptive therapies have demonstrated favorable efficacy in reducing bone pain and delaying the onset and reducing the risk of SREs [Saad et al. 2002, 2004; Lipton et al. 2003; Rosen et al. 2004; Bouganim et al. 2011; Fizazi et al. 2011; Henry et al. 2011]. There are two main classes of antiresorptive compounds currently approved for prevention of SREs in patients with GU malignancies: bisphosphonates (BPs) and the more recently developed monoclonal antibody against the receptor activator of nuclear factor κB ligand (RANKL), denosumab (Dmab). There are important differences in the antiresorptive mechanisms of action and pharmacokinetics of BPs and Dmab that may result in differences in efficacy and safety, particularly in oncology settings. This review focuses on fundamental differences between the two antiresorptive therapies and the potential implications for use of these agents in the context of GU malignancies.
Mechanism of action of antiresorptive therapies in bone
Bisphosphonates are synthetic analogues of pyrophosphate that are resistant to enzymatic degradation through the substitution of the central oxygen atom by a carbon atom [Yuasa et al. 2007; Green and Clezardin, 2010]. Variation in the substituent groups bound to the central carbon account for differences in therapeutic activities of the BPs. There are two broad classifications of BPs: non-nitrogen-containing BPs and the most recent generation, nitrogen-containing BPs (NBPs), which have greater antiresorptive activity. Non–nitrogen-containing BPs are internalized and metabolized by osteoclasts to nonhydrolyzable adenosine triphosphate (ATP) analogues that inhibit osteoclast activity and lead to apoptosis [Yuasa et al. 2007]. In contrast, the NBPs inhibit farnesyl pyrophosphate synthase in the mevalonate pathway, thereby inhibiting the post-translational prenylation and function of small guanosine 5′-triphosphatase (GTPase) proteins. Small GTPase proteins modulate signaling pathways that are essential for osteoclast function and survival [Green and Clezardin, 2010].
Denosumab inhibits osteoclast-mediated bone destruction by binding and neutralizing RANKL [Castellano et al. 2011]. Soluble and membrane-bound RANKL, synthesized by various cell types including osteoblasts and activated T cells, plays a key role in normal bone remodeling by binding and activating the receptor activator of nuclear factor κB (RANK) receptor on the surface of osteoclasts. Activation of RANK modulates several signal transduction pathways, including protein kinase pathways and activation of the transcription factor nuclear factor κB that leads to stimulation of osteoclast formation, function, and survival and, as a result, increased bone resorption. Inhibition of RANKL by high-affinity binding to Dmab prevents activation of RANK, thereby reducing bone resorption and increasing bone volume, density, and strength [Castellano et al. 2011].
Pharmacokinetics of antiresorptive therapies
Following intravenous administration, BPs are rapidly cleared from the systemic circulation by deposition in bone and renal excretion of unmetabolized drug within a few hours [Chen et al. 2002; Kimmel, 2007]. Bisphosphonates are retained in the bone via binding to areas of exposed hydroxyapatite crystals where they act to reduce bone resorption by osteoclasts. During bone remodeling, low levels of BP are released from bone, accounting for the longer terminal phase of elimination. Pharmacokinetics of the NBP zoledronic acid (ZOL) measured in patients with bone metastases demonstrate multiphasic plasma disposition with plasma half lives of 0.2 and 1.4 h initially, followed by longer half lives of 39 and 4526 h for subsequent elimination phases of very low concentrations between day 2 and day 28 post dose [Chen et al. 2002]. This study confirmed that the antiresorptive effects of ZOL persisted over 28 days, thus supporting monthly infusions of ZOL. Furthermore, a study evaluating adjuvant endocrine therapy in combination with ZOL in women with early-stage breast cancer demonstrated that ZOL improved bone mineral density (BMD) for 2 years after discontinuation of ZOL therapy, suggesting a prolonged duration of effect [Gnant et al. 2008].
Denosumab is administered subcutaneously every 4 weeks in patients with bone metastases; however, unlike BPs, Dmab is distributed systemically and follows nonlinear, dose-dependent pharmacokinetics with detectable serum levels as early as 1 h post dose and maximum serum concentrations within 1–3 weeks. Following a single 3 mg/kg injection, the elimination half life for Dmab ranged from 33.3 to 46.3 days in patients with multiple myeloma and breast cancer, respectively [Body et al. 2006]. These properties have clinical implications for specificity of action and duration of benefit. Because Dmab is not retained at its site of action in the bone, the antiresorptive effect of this agent is quickly reversed after the drug is cleared [Miller et al. 2008].
Incidence of skeletal-related events and clinical efficacy of antiresorptive agents
The clinical efficacy of antiresorptive agents is based on their ability to inhibit osteoclast-mediated bone degradation and thus prevent or delay development of SREs (Table 1) [Saad et al. 2002, 2004; Dearnaley et al. 2003, 2009; Ernst et al. 2003; Lipton et al. 2003; Small et al. 2003; Saad and Lipton, 2005; Mason et al. 2007; Fizazi et al. 2009, 2011; Zaghloul et al. 2010; Henry et al. 2011]. Placebo-controlled trials of antiresorptive therapy in patients with GU malignancies and bone metastases show that without treatment, 44–90% of patients will experience at least 1 SRE [Saad et al. 2002, 2004; Lipton et al. 2003; Saad and Lipton, 2005; Zaghloul et al. 2010; Woodward et al. 2011]. In the absence of bone-targeted therapy, approximately half of patients with bone metastases from castration-resistant prostate cancer (CRPC) experienced an SRE [Saad et al. 2004] and 79% of patients with bone metastases from renal cell carcinoma (RCC) experienced an SRE [Saad and Lipton,. 2005]. A small, prospective, placebo-controlled trial in patients with bone metastases from bladder cancer reported that 90% of patients in the placebo group developed an SRE [Zaghloul et al. 2010]. The skeletal morbidity rate (mean SREs per patient years) for patients with advanced prostate cancer with a history of bone metastases was 1.49 SREs per patient year in 15 months in one study [Saad et al. 2002], and in patients with RCC and at least one site of bone metastases, the mean skeletal morbidity rate was 3.38 [Lipton et al. 2003].
Efficacy of antiresorptive therapy for skeletal-related event prevention in patients with genitourinary cancers.
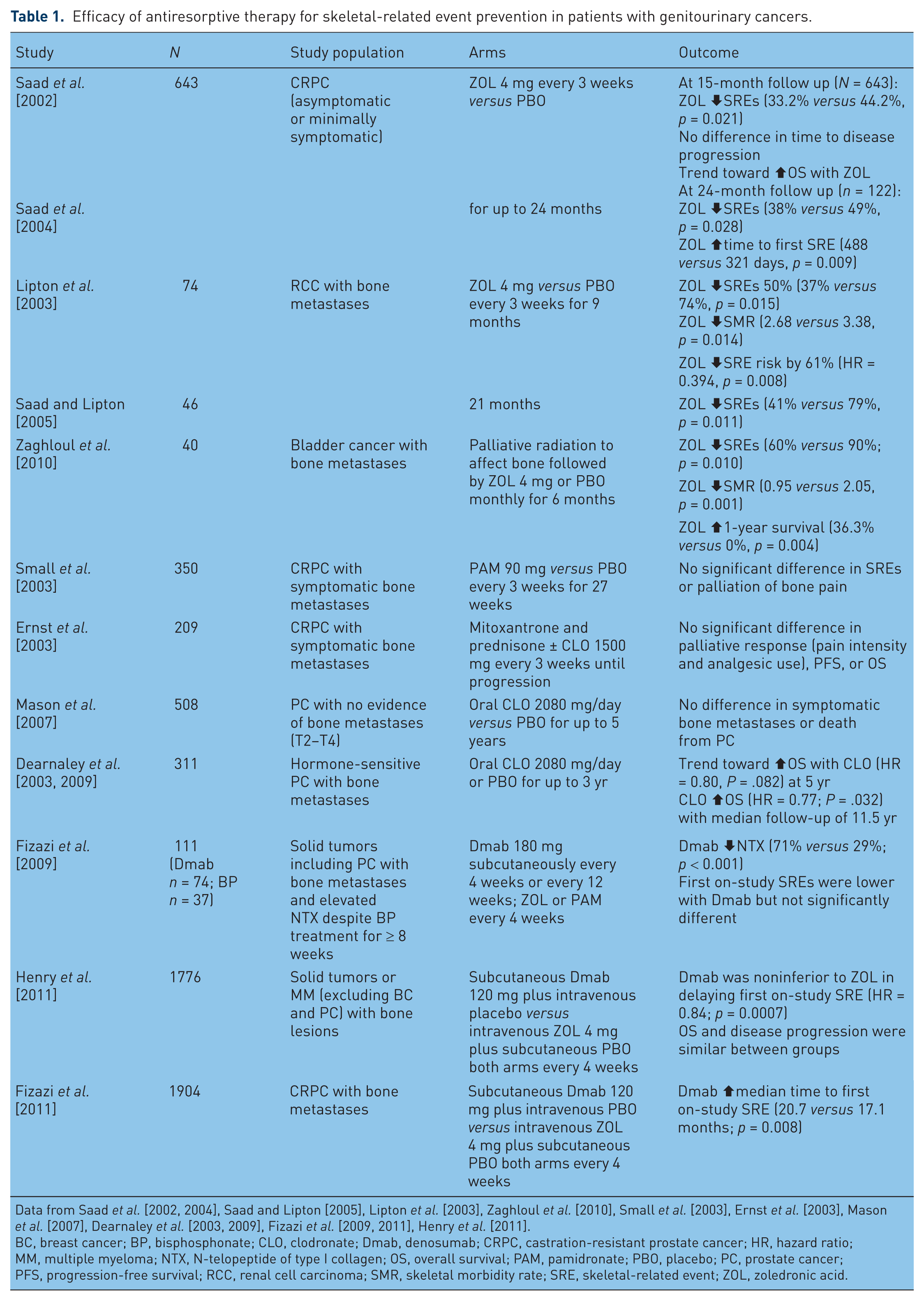
Data from Saad et al. [2002, 2004], Saad and Lipton [2005], Lipton et al. [2003], Zaghloul et al. [2010], Small et al. [2003], Ernst et al. [2003], Mason et al. [2007], Dearnaley et al. [2003, 2009], Fizazi et al. [2009, 2011], Henry et al. [2011].
BC, breast cancer; BP, bisphosphonate; CLO, clodronate; Dmab, denosumab; CRPC, castration-resistant prostate cancer; HR, hazard ratio; MM, multiple myeloma; NTX, N-telopeptide of type I collagen; OS, overall survival; PAM, pamidronate; PBO, placebo; PC, prostate cancer; PFS, progression-free survival; RCC, renal cell carcinoma; SMR, skeletal morbidity rate; SRE, skeletal-related event; ZOL, zoledronic acid.
Pooled data from two multicenter, randomized, placebo-controlled trials of pamidronate in patients with metastatic prostate cancer and bone pain demonstrated no significant treatment benefit as measured by reduction in SREs or palliation of bone pain [Small et al. 2003]. In contrast, ZOL, a much more potent NBP than pamidronate, has demonstrated broad efficacy in the context of SRE prevention in patients with bone metastases from multiple tumor types, including GU malignancies [Rosen et al. 2004; Saad et al. 2004; Saad and Lipton, 2005].
A placebo-controlled, randomized, phase 3 trial (N = 643) evaluating the efficacy of ZOL (4 mg intravenously over 15 min every 3 weeks) for prevention of SREs in patients with bone metastases from CRPC followed 122 patients for 24 months [Saad et al. 2004]. The incidence of at least one SRE was significantly lower among patients receiving ZOL (38% versus 49%, p = 0.028). Treatment with ZOL resulted in a significant reduction in the ongoing risk of SREs by 36% (p = 0.002) and significantly reduced the median time to first SRE (488 days versus 321 days; p = 0.009) [Saad et al. 2004]. The annual incidence of SREs was 0.77 for patients in the ZOL treatment group compared with 1.47 for the placebo group (p = 0.005) [Saad et al. 2004]. In an exploratory analysis in 422 patients with CRPC, the effect of ZOL (4 mg every 3 weeks) on SRE incidence was stratified according to baseline pain status [Saad and Eastham, 2010]. Among patients with baseline bone pain, ZOL reduced the proportion of patients with at least one SRE by 18% versus placebo, and by 39% in patients without pain at baseline.
A retrospective, subset analysis of patients with RCC (n = 74) enrolled in a single multicenter, prospective, placebo-controlled trial of ZOL for treatment of skeletal metastases from solid tumors has been reported at 9-month [Lipton et al. 2003] and 21-month follow up [Saad and Lipton, 2005]. The trial enrolled patients with a variety of solid tumors, including 74 patients with RCC [Lipton et al. 2003]. At 9-month follow up, ZOL therapy significantly reduced the proportion of patients in this subset with an SRE (37% versus 74%; p = 0.015) and reduced the risk of developing an SRE by 61% compared with placebo [hazard ratio (HR) = 0.394; p = 0.008] [Lipton et al. 2003]. The extended 21-month follow up of 46 patients in the RCC subset demonstrated continued benefit of ZOL with a significantly delayed time to first SRE by nearly 1 year and a significantly delayed time to disease progression compared with placebo (586 days for ZOL versus 89 days for placebo; p = 0.014) [Saad and Lipton, 2005]. A retrospective survival analysis of patients with RCC enrolled in this same phase III study demonstrated that ZOL therapy was associated with a significant improvement in overall survival compared with placebo (11.4 versus 7.1 months, respectively; HR = 0.54; p = 0.014) [Michaelson et al. 2010].
Additionally, a recent prospective, randomized, placebo-controlled trial has also confirmed the benefit of ZOL in patients with bladder cancer and bone metastases (N = 40) [Zaghloul et al. 2010]. Patients treated with ZOL experienced a significantly reduced number of SREs by 54% (p = 0.001), prolonged time to first on-study SRE (p = 0.0001), and decreased bone pain scores compared with placebo (p = 0.015). Notably, there was a significantly increased 1-year survival rate for patients in the ZOL treatment group (36.3% versus 0% for placebo; p = 0.004). These studies demonstrate consistent reduction and delay in the development of SREs for patients with GU malignancies who are treated with ZOL.
Recently, Dmab achieved noninferiority versus ZOL in delaying the time to first on-study SRE (20.6 versus 16.3 months, respectively) in patients with bone metastases from solid tumors (excluding breast and prostate cancer) or multiple myeloma (N = 1776; HR = 0.84; 95% confidence interval [CI] 0.71–0.98; p = 0.0007) [Henry et al. 2011]. It is important to note that the patient population in this trial included only 218 (12%) patients with GU cancers (n = 155 for RCC; n = 63 for bladder cancer) [Henry et al. 2009]. However, post hoc analyses by tumor type, although underpowered for statistical analyses, demonstrated similar benefits with Dmab for delaying first on-study SRE in patients with renal, colorectal, or bladder cancer as in the overall trial population [Henry et al. 2009]. In the overall population, Dmab was neither statistically superior to ZOL in time to first on-study SRE (p = 0.06) nor in time to first and subsequent (multiple) SREs (p = 0.14) [Henry et al. 2011]. Overall survival and disease progression were similar for both treatment groups as well. A second double-blind, randomized, phase III trial compared Dmab and ZOL in 1904 patients with CRPC. The median time to first on-study SRE was significantly longer in the patients receiving Dmab compared with those in the ZOL treatment group (20.7 versus 17.1 months, respectively; p = 0.008) [Fizazi et al. 2011].
In addition to reduction of SRE risk, antiresorptive agents have been shown to reduce bone pain. Patients with CRPC receiving treatment with ZOL had a significant reduction in composite Brief Pain Inventory (BPI) score compared with placebo-treated patients at 2 years (p = 0.024) [Saad et al. 2004]. Visual analog scale (VAS) scores for pain were significantly reduced in another trial of ZOL therapy in patients with solid tumors, including prostate cancer (p < 0.05) [Vogel et al. 2004]. An open-label study of ZOL evaluated the safety and efficacy in patients with a variety of malignancies, including GU cancers, over the course of 12 ZOL (4 mg) infusions administered every 3 or 4 weeks. Mean VAS scores decreased significantly by 13.9 ± 32.3 (p < 0.0001), and mean analgesic scores decreased by 0.56 ± 1.42 (p < 0.0001) [Kretzschmar et al. 2007]. Recent evidence from analysis of phase III data comparing ZOL and Dmab demonstrated similar benefits for both treatments in patients with CRPC and bone pain [Patrick et al. 2011]. The proportion of patients with decreased pain interference of general activity declined over 18 months, and treatment prolonged the time to worsening of pain interference for patients in both treatment arms. These studies highlight the clinical benefit associated with prevention of abnormal bone resorption in patients with metastatic bone disease. Both ZOL and Dmab have been shown to reduce bone pain and significantly reduce the incidence of SREs in patients with GU malignancies.
Tolerability profiles of antiresorptive agents
Antiresorptive therapies are generally well tolerated, particularly with close adherence to established guidelines for drug administration and adverse event (AE) management. ZOL has a long-term, well defined safety profile [Saad et al. 2002, 2004; Aapro and Saad, 2012] with well established protocols regarding AE management [Zometa PI, 2011]. In contrast, because it is a newer antiresorptive agent, the long-term safety profile for Dmab has yet to be established [Xgeva PI, 2010]. However, in the phase III trials of Dmab versus ZOL, total AEs and serious AEs were similar between treatment arms and both agents were well tolerated [Fizazi et al. 2011; Henry et al. 2011].
Osteonecrosis of the jaw (ONJ), renal toxicity, hypocalcemia, and acute phase reactions (APRs) are AEs of interest that have been reported in patients receiving antiresorptive therapies. Rates of renal AEs and ONJ were also similar for Dmab and ZOL. Indeed, the incidence of ONJ was uncommon and was reported at similar rates in phase III trials comparing Dmab with ZOL (1–2%) in patients with advanced cancer [Fizazi et al. 2011; Henry et al. 2011]. AEs potentially associated with renal impairment were similar in patients with CRPC receiving Dmab (15%) compared with ZOL (16%) [Fizazi et al. 2011]. Moreover, renal AEs also were similar across treatment arms in patients with solid tumors (excluding breast or prostate cancer) or multiple myeloma (8% Dmab versus 11% ZOL; p = 0.07) [Henry et al. 2011].
Hypocalcemia and APR AEs were notably different for Dmab compared with ZOL [Fizazi et al. 2011; Henry et al. 2011]. Indeed, hypocalcemia was significantly more common in patients receiving Dmab compared with ZOL (11–13% versus 6%, respectively; p < 0.0001) [Fizazi et al. 2011; Henry et al. 2011]. Notably, monitoring serum calcium to assess hypocalcemia for patients receiving Dmab is indicated in the Dmab prescribing information [Xgeva PI, 2010]. Furthermore, AEs related to APR occurred less frequently in patients receiving Dmab (7–8%) compared with ZOL (15–18%) [Fizazi et al. 2011; Henry et al. 2011]. Generally, APR AEs are easily managed with analgesics, and prophylactic use of acetaminophen can reduce the incidence and severity of these events [Tanvetyanon and Stiff, 2006; Aapro et al. 2008]. Furthermore, APRs are generally mild and reversible and either do not manifest in subsequent cycles of therapy or are of reduced severity [Maxwell et al. 2003].
Use of bone turnover markers to optimize treatment
The use of bone turnover markers has been suggested as a way to further optimize and define treatment outcomes for the antiresorptive agents. Given their differing mechanisms of action, there may be differences in physiological effect beyond prevention of SREs that occurs with ZOL or Dmab therapy. Studies suggest that elevated bone turnover markers may be associated with a greater risk of SREs and reduced survival duration [Brown et al. 2005; Cook et al. 2006; Saad et al. 2007]. For example, a marker of bone metabolism, N-telopeptide of type I collagen (NTX), which is a marker of osteoclast-mediated bone resorption, has been identified and provides a useful surrogate measure for monitoring skeletal health in patients with bone metastases [Coleman et al. 2005, 2011]. In an exploratory analysis of data from three separate phase III trials of ZOL in patients with bone metastases, 61% (193/314) of patients with CRPC had elevated NTX levels at baseline [Lipton et al. 2008]. Normalization of NTX after 3 months of ZOL therapy correlated with a 59% reduced risk of death [relative risk (RR) = 0.41; 95% CI 0.29–0.59; p < 0.0001] (Figure 1), a nonsignificant 29% reduced rate of first fracture (p = 0.3653), and a 49% increase in SRE-free survival (p = 0.0009) compared with patients with persistently elevated NTX levels [Lipton et al. 2008]. In a study of patients with prostate cancer undergoing hormonal therapy it was reported that elevated levels of bone turnover markers correlate with recurrence and progression of bone metastases [Noguchi et al. 2003]. Thus, bone turnover markers may have utility for assessing response to treatment in patients with bone metastases, including overall tumor response. In fact, in a recent study of patients with prostate cancer metastatic to bone undergoing ZOL treatment, overall survival was longer in patients whose bone turnover marker levels decreased within 3 months [Izumi et al. 2012].
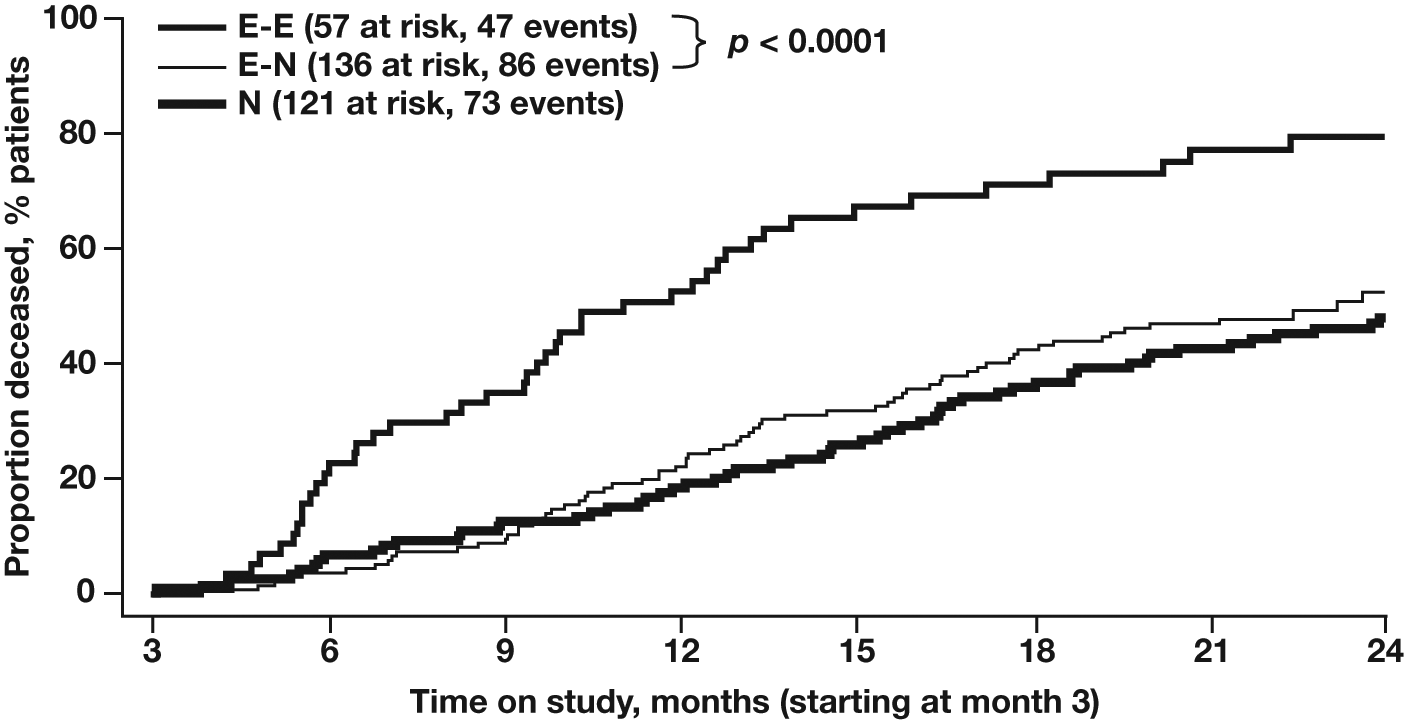
Kaplan–Meier survival estimates stratified by baseline and 3-month N-telopeptide of type I collagen (NTX) levels. Patients with bone metastases from hormone-refractory prostate cancer treated with zoledronic acid. E-E, patients with elevated baseline and 3-month NTX; E-N, patients with elevated baseline and normalized 3-month NTX; N, patients with normal baseline NTX. Reprinted with permission from Lipton et al. [2008].
Denosumab therapy is also associated with reduced NTX levels that correlate with fewer on-study SREs [Fizazi et al. 2009, 2011]. In the phase III trial comparing Dmab with ZOL for treatment of bone metastases in CRPC, Dmab was associated with significantly greater reductions in NTX and bone-specific alkaline phosphatase compared with ZOL [Fizazi et al. 2011]. However, both agents reduced bone turnover marker levels, and there was no difference between Dmab and ZOL in time to disease progression (HR = 1.06, p = 0.30) or overall survival (HR = 1.03, p = 0.65) [Fizazi et al. 2011]. Survival was not analyzed according to bone turnover marker response. Another study that evaluated the effect of Dmab on BMD and turnover markers in postmenopausal women with low bone density observed a reversal of effect on BMD and turnover makers such that levels of bone alkaline phosphatase and NTX increased above baseline levels after discontinuation of Dmab [Miller et al. 2008]. Further research regarding the correlation of bone turnover marker levels with anticancer and bone disease outcomes from antiresorptive therapies will aid in understanding differences between the current antiresorptive agents.
Evidence for the potential anticancer benefits of antiresorptive agents
In preclinical and clinical studies in patients with advanced cancer, BPs have been shown to elicit a variety of anticancer responses from direct effects on tumor cell survival and proliferation to indirect antitumor effects mediated by their modulation of angiogenesis, host immunosurveillance, and inhibition of tumor-promoting processes in the bone microenvironment [Yuasa et al. 2007; Clezardin, 2011]. In general, antiresorptive agents inhibit a broad range of cellular functions, including cell differentiation, which is particularly relevant in the context of osteoclast activity and may provide important anticancer effects as well. For example, the NBP-mediated inhibition of farnesyl pyrophosphate synthase also causes accumulation of isopentenyl-pyrophosphate (IPP) that has been shown to activate γδ T cells. The γδ T cells are a subset of the peripheral blood T cells that play a role in tumor-specific immunity. Cytotoxic activity of γδ T cells toward a range of malignant cell types, including bladder cancer, has been demonstrated in vitro [Kato et al. 2001].
Zoledronic acid is a potent inducer of γδ T-cell proliferation, which may in part account for ZOL-induced anticancer effects [Mariani et al. 2005]. Two small studies in patients with prostate cancer have shown that ZOL activates and increases the number of γδ T cells [Dieli et al. 2007; Naoe et al. 2010], and in one of the studies ZOL treatment was associated with a reduction in prostate-specific antigen (PSA) velocity in 50% (5/10) of the patients [Naoe et al. 2010]. Interestingly, activation of γδ T cells after ZOL treatment alone was also associated with reduced PSA velocity in two patients [Naoe et al. 2010]. These studies further suggest that ZOL combined with interleukin-2 may offer further benefit in terms of γδ T-cell proliferation and immunotherapy effect.
In addition to immunomodulatory effects, data suggest that NBPs may inhibit tumor-mediated angiogenesis and render the bone microenvironment less conducive to growth of micrometastases [Wood et al. 2002]. The effect of NBPs on angiogenesis and neovascularization is presumed to be related to inhibition of angiogenic factors [eg, vascular endothelial growth factor, platelet-derived growth factor, basic fibroblast growth factor (bFGF)] necessary for proliferation of endothelial cells [Wood et al. 2002]. Furthermore, ZOL has been shown to modulate cellular adhesion and migration and inhibit angiogenesis induced by subcutaneous implants containing bFGF in vivo [Wood et al. 2002]. The effects of NBPs on the bone microenvironment, angiogenesis, and stimulation of immune surveillance via γδ T-cell proliferation suggest the potential of these agents for additional anticancer benefits.
In addition to indirect effects, preclinical studies have shown direct anticancer activity of ZOL in RCC cell lines. Indeed, ZOL treatment induced apoptosis in several RCC cell lines [Pandha et al. 2006; Ullen et al. 2009; Zwolak et al. 2010]. Furthermore, a single case study in which lung and bone metastases displayed remission after BP therapy and a small retrospective analysis demonstrating improved objective response rate with ZOL therapy add support for the potential direct anticancer effects of ZOL in RCC [Kijima et al. 2008, 2009].
The potential anticancer activity of ZOL has also been observed when used in combination with traditional anticancer agents. A number of studies have demonstrated an additive or synergistic effect of ZOL with chemotherapy against leukemias and solid tumors [Kimura et al. 2004; Matsumoto et al. 2005; Neville-Webbe et al. 2005, 2006, Sato et al. 2006]. The combination of an NBP (minodronic acid) with cisplatin or paclitaxel has been shown to kill bladder cancer cells in culture and has inhibited growth of bone metastases in vivo in a bladder cancer mouse model [Sato et al. 2006]. Doxorubicin-induced apoptosis has also been shown to be synergistically enhanced by the use of ZOL in breast and prostate cancer cells [Neville-Webbe et al. 2005]. This study highlights the importance of drug sequence when adding ZOL for treatment of malignant cells, as apoptosis was only enhanced by the use of ZOL after treatment by doxorubicin. There is also evidence for an additive anticancer effect of ZOL when combined with endocrine therapy. Long-term follow up of a trial comparing adjuvant endocrine therapy with or without ZOL has recently demonstrated that the addition of ZOL improved disease-free survival of patients with early-stage breast cancer (92% versus 88%, log-rank p = 0.008) [Gnant et al. 2011].
Circulating tumor cells (CTCs) have not been extensively explored in GU malignancies; however, data from other solid tumors suggest that CTCs are associated with a worse prognosis and that reducing CTC numbers may be associated with reduced risk of recurrent/progressive disease [Cristofanilli et al. 2004, 2005; Budd et al. 2006; Hayes et al. 2006; Janni et al. 2011]. Two studies in metastatic prostate cancer have demonstrated a correlation between greater numbers of CTCs, elevated serum PSA, and poor overall survival (Figure 2) [Moreno et al. 2005; Garcia et al. 2007]. Another study evaluating CTCs in relation to disease spread and outcome in patients with CRPC found that the baseline CTC number was strongly correlated with survival, and that the predictive value increased when baseline PSA and serum albumin were included in the analysis. Higher numbers of CTCs were observed in patients with bone metastases compared with other sites of metastases [Danila et al. 2007]. Most recently, research in patients with metastatic CRPC receiving chemotherapy showed that CTCs and lactate dehydrogenase levels may be useful as surrogate markers for overall survival [Scher et al. 2011]. ZOL has previously been shown to reduce CTC numbers in patients with cancer, suggesting another mechanism by which ZOL may potentially improve overall outcomes in patients with GU malignancies [Solomayer et al. 2012; Aft et al. 2010]. These observations of a potential direct anticancer effect from ZOL have not been reported with Dmab, indicating important differences in the pharmacologic effects of these agents that are likely based on their different mechanisms of action and pharmacokinetic profiles.

(a) Probability of overall survival time in the subset of patients with CRPC (n = 26) for those with less than 5 CTCs/7.5 ml blood (solid line) and 5 or more CTCs/7.5 ml blood (dotted line). Reprinted with permission from Moreno et al. [2005]. (b) Overall survival versus CECs/ml in patients with CRPC. Reprinted with permission from Garcia et al. [2007]. CEC, circulating epithelial cell; CRPC, castration-resistant prostate cancer; CTC, circulating tumor cell.
To date, there is no clinical evidence of anticancer effects with Dmab; however, preclinical studies with inhibitors of RANKL signaling (which may mimic Dmab effects) have been conducted. Potential mechanisms of anticancer effects from Dmab are related to the role of RANK, RANKL, and endogenous osteoprotegerin (OPG), a surrogate for Dmab activity in animal studies, in regulation of osteoclastogenesis and bone resorption [Wada et al. 2006]. While it has been shown that OPG binding to RANKL prevents the osteolytic action of prostate cancer [Zhang et al. 2001], OPG can prevent tumor necrosis factor-related apoptosis-induced ligand (TRAIL)-mediated apoptosis [Holen et al. 2002]. In contrast, the soluble receptor activator of nuclear factor κB (sRANK) inhibited RANKL in a mouse model but did not prevent TRAIL-induced apoptosis and did reduce prostate tumor cell growth [Zhang et al. 2003]. These data suggest that inhibition of RANKL by molecules that do not interact with TRAIL may prevent metastatic cancer progression in bone. However, a preclinical study showed that Dmab could not induce apoptosis or inhibit proliferation of a breast cancer cell line (MCF-7), but that ZOL could [Ebert et al. 2011]. Moreover, based on the mechanism of Dmab’s antiresorptive effect, an immune-mediated anticancer response to Dmab therapy is unlikely, and there have been concerns regarding increased immunosuppression resulting from RANKL inhibition because, in addition to expression on osteoclasts, RANKL is expressed on T and B cells of the immune system [Kawai et al. 2006; Benzaïd et al. 2011]. Indeed, a preclinical study has shown that Dmab does not induce γδ T-cell expansion in a breast cancer model [Benzaïd et al. 2011].
Although there is no clinical evidence for antitumor activity associated with Dmab, a clinical trial to assess the potential of Dmab to prevent bone metastases in patients with prostate cancer and at high risk for development of bone metastases has recently been presented [Oudard et al. 2011; Smith et al. 2012]. In this phase III trial in patients with CRPC at high risk for bone metastases (N = 1432), Dmab (120 mg every 4 weeks) significantly prolonged bone-metastases-free survival by 4.3 months versus placebo (29.5 versus 25.2 months, respectively; HR = 0.85, p = 0.028) [Oudard et al. 2011; Smith et al. 2012]. However, Dmab did not prolong progression-free (HR = 0.89, p = 0.093) or overall survival (HR = 1.01, p = 0.91) versus placebo [Oudard et al. 2011; Smith et al. 2012].
Conclusions
Questions remain regarding the optimal duration and dosing of antiresorptive therapies to prevent or palliate SREs. Bone turnover markers such as NTX may be useful surrogates to monitor therapeutic effects on bone and help guide future trials. Furthermore, assessment of circulating angiogenic markers and CTCs may provide greater insight into the anticancer activity of antiresorptive therapies. Currently, three large trials are ongoing in patients with prostate cancer to evaluate the effect of ZOL on event-free and overall survival [Coleman et al. 2011].
Clinical trials of antiresorptive agents confirm the value of this therapy in prevention of potentially debilitating and life-limiting SREs, and provide evidence for a further role in delaying disease progression and prolonging survival in some cases. The potential for synergistic benefit with combined chemotherapy or androgen therapy plus ZOL in GU malignancies is encouraging, and future trials are anticipated.
Footnotes
Acknowledgements
I thank Colleen Gilbert, PhD, ProEd Communications, Inc., for her medical editorial assistance with this manuscript.
Funding
Financial support for medical editorial assistance was provided by Novartis Pharmaceuticals Corporation. No additional funding was provided.
Conflict of interest statement
None declared.