
Abstract
Prostate cancer hypoxia is associated with inferior prognosis and resistance to treatment. The use of androgen deprivation therapy, both prior to and during radiotherapy, may exacerbate underlying hypoxia. Whilst larger radiation doses per fraction may achieve therapeutic gain, this is balanced by the reduced opportunity for re-oxygenation to take place during the course of treatment. Improving the underlying hypoxic tumour environment may therefore improve the treatment outcomes. Strategies to combat tumour hypoxia, with particular focus on the use of carbogen gas breathing concurrently with radiotherapy, is the subject of this review.
Introduction
The existence of hypoxia in tumours was first postulated by Gray and Tomlinson over half a century ago [Thomlinson and Gray, 1955]. This arises as the tumour outgrows its blood supply, resulting in diffusion-limited chronic hypoxia. The cyclical temporary collapse of immature and chaotic tumour vasculature can also result in perfusion-limited acute hypoxia. Hypoxia has been associated with inferior prognosis and resistance to both chemotherapy and radiotherapy in a variety of tumour sites [Hockel and Vaupel, 2001]. Whilst the subject of tumour hypoxia has been a major focus of preclinical and translational research, the application of hypoxic modifiers in wider routine clinical practice has been limited [Brown and Wilson, 2004; Overgaard, 2007].
Hypoxia modification may improve the outcome for patients undergoing prostate radiotherapy for the following reasons. Firstly, hypoxia is associated with poor prognosis among prostate cancer patients. Secondly, the use of androgen deprivation therapy can exacerbate the underlying hypoxia and confer radio resistance. Thirdly, the effect of hypoxia is potentially more detrimental with the increasingly popular hypofractionated radiotherapy schedules compared with conventional ones.
Hypoxia and radiotherapy
It has been argued that all radiosensitizers, however different their mechanisms of action, exert their effect either through improving tumour oxygenation or exploiting the existing hypoxia [Oronsky et al. 2011]. The oxygen fixation hypothesis has been the classical explanation for the enhancement of radiation-induced cytotoxicity by oxygen [Horsman and Overgaard, 2002]. However, there are other mechanisms, such as its role on cell cycle progression and its effect on tumour vasculature, which may also contribute to this effect.
The oxygen fixation hypothesis states that ionizing radiation induces the formation of highly reactive free radicals in DNA (R*). In the absence of oxygen, the damaged DNA is restored back to its original form when these free radicals react with H+. However, oxygen can ‘fix’ this damage by reacting with R* to form RO2*, which undergoes further reactions to result in DNA strand breaks and ultimately cell death. The fixation of radiation-induced damage to DNA by oxygen can actually be mimicked by a class of radiosensitizers called the nitro-imidazoles, which will be discussed in more detail in the latter part of this review.
Radiosensitivity is cell cycle dependent. In general, cells are most sensitive to radiation during mitosis and in the G2 phase of the cell cycle, less so in G1, and least sensitive during the latter part of the S phase [Pawlik and Keyomarsi, 2004]. Hypoxia can induce cell cycle arrest in all phases, in particular at the G1/S phase interface, whilst reoxygenation can promote resumption of cell cycle progression [Koritzinsky et al. 2001; Douglas and Haddad, 2003]. Interestingly, chronically hypoxic cells may actually be more radiosensitive compared with normoxic ones on reexposure to oxygen [Koritzinsky et al. 2001; Zolzer and Streffer 2002; Chan et al. 2008] possibly due to the impairment of the homologous recombinant DNA repair mechanism (HR) following hypoxic exposure [Sprong et al. 2006; Chan et al. 2008, 2010]. In theory, this impairment of HR can be further exploited for therapeutic gain through the use of an inhibitor of the poly (adenosine diphosphate ribose) polymerase (PARP) pathway. Oxidative stress from background cellular metabolism results in the formation of single strand breaks (SSBs) and nucleotide base damage. PARP is a critical component for their repair. In vitro studies have shown that cells with defective breast cancer genes (BRCA1 and BRCA2), which are involved in the HR repair mechanism of double strand breaks (DSBs), are particularly sensitive to PARP inhibition [Bryant et al. 2005; Farmer et al. 2005]. Suppression of PARP function prevents background endogenous SSBs from being repaired; the increased number of SSBs will cause the collapse of replication forks and generate DSBs, which eventually result in cell death if left unrepaired due to defects in the DSB repair mechanism.
At the molecular level, the hypoxia inducible factor pathway (HIF-1) has been shown to affect tumour radiosensitivity [Moeller and Dewhirst, 2006]. HIF-1 is a transcription factor that lies in the centre in mediating cellular responses to hypoxia. It impacts on a range of cellular physiological processes, such as angiogenesis, apoptosis, cellular metabolism and proliferation. In the presence of oxygen, HIF-1α (a subunit of HIF-1) is hydroxylated by proline hydroxylase. This leads to its polyubiquination by the product of the von Hippel–Landau gene and recognition by proteosomes for degradation. Under hypoxic conditions, proline hydroxylase is inactive. HIF-1α is thus no longer targeted for degradation and translocates into the nucleus to promote the transcription of its downstream effectors. These include vascular endothelial growth factor (VEGF), which promotes angiogenesis, osteopontin which regulates inflammatory response, and glucose transporter 1 (GLUT-1) which is involved in cellular metabolism of glucose. The levels of expression of HIF-1α and its effectors have been found to be of prognostic significance in radiotherapy studies across a range of tumour sites [Haber et al. 1998; Birner et al. 2000; Airley et al. 2001; Cooper et al. 2003; Hoskin et al. 2003; De Schutter et al. 2005; Eckert et al. 2010; Jans et al. 2010; Seeber et al. 2010].
The precise mechanism whereby HIF-1 affects radiosensitivity is yet to be fully elucidated. In addition to its direct impact on tumour cells, radiation may also indirectly result in cytotoxicity through its effect on the supporting tumour vasculature [Garcia-Barros et al. 2003]. During a course of conventionally fractionated radiotherapy, chronic and cyclical hypoxia may diminish tumour cell kill by offering protection to the tumour vasculature through the upregulation of the HIF-1 pathway [Moeller et al. 2004; Dewhirst et al. 2008]. The impressive local tumour control rates achieved by high-dose single-fraction radiotherapy delivered using stereotactic body radiotherapy under hypoxic conditions have been cited by some as clinical evidence to support the indirect effect of radiation on tumour cells via its effect on tumour vasculature [Yamada et al. 2008; Brown and Koong, 2008]. A significant increase in the radiation dose per fraction [Fuks and Kolesnick, 2005], or blockading the HIF-1 pathway [Moeller et al. 2005; Schwartz et al. 2010], can potentially overcome the protection of tumour vasculature via the upregulation of the HIF-1 pathway.
Hypoxia in prostate cancer
Hypoxia has been demonstrated in prostate tumours by direct measurement, immunohistochemical studies and imaging. Movsas and colleagues [Movsas et al. 1999] inserted Eppendorf oxygen partial pressure (pO2) microelectrodes into the prostate of 12 patients during surgery or brachytherapy. Muscle readings were used as an internal control. They found that pO2 measurements from the pathologically involved portions of the prostate were significantly lower than those from normal muscle or benign regions of the prostate. Also using direct Eppendorf electrode measurements, Parker and colleagues showed that localized prostate cancers were often markedly hypoxic and that significant heterogeneity in oxygenation level was present within the prostate tumours of individual patients as well as between patients with similar tumours [Parker et al. 2004].
Having established the existence of hypoxia in prostate cancer, Movsas and colleagues went on to show that a low prostate cancer:normal tissue pO2 ratio was predictive of prostate-specific antigen progression-free survival following brachytherapy treatment [Turaka et al. 2012]; however, the number of events (nine) and the total number of patients (57) were relatively small. Also caution must be exercised when interpreting results from electrode studies, as highlighted by Stewart and colleagues [Stewart et al. 2010]. The insertion of the electrodes themselves can disturb tumour blood flow and hence influence oxygen level. Furthermore, when obtained under general anaesthesia, the type of anaesthesia used can impact on the oxygen level readings [Movsas et al. 1999]. Moreover, the Eppendorf technique only measured the mean oxygen level in the tract rather than the overall oxygen status of the tumour.
Carnell and colleagues carried out immunohistochemical analyses on whole prostate specimens from 37 patients who had undergone radical prostatectomy for their localized prostate cancer. Prior to surgery, patients were intravenously given pimonidazole, which was used as an extrinsic marker of tumour hypoxia. Antibodies raised against pimonidazole were used to identify regions of hypoxia in the prostate specimen. Pimonidazole binding was present in the prostate carcinomas of 34 out of the 37 patients. Correlation between strong pimonidazole staining and Gleason score was demonstrated [Carnell et al. 2006].
Immunohistochemical studies carried out by Vergis and colleagues on 308 patients who had either undergone radical prostatectomy or radiotherapy demonstrated that those whose tumours had an increased expression of HIF-1α or VEGF were more likely to experience biochemical relapse following their initial local treatment [Vergis et al. 2008]. Osteopontin expression was predictive of outcome following surgery but not radiotherapy. The predictive value of VEGF for disease-specific survival following radiotherapy [Green et al. 2007] and biochemical progression-free survival following surgery [Shariat et al. 2004] has also been demonstrated in other cohorts of patients. Other studies have shown associations between the expression of other proteins involved in the hypoxia-driven HIF-1 pathway, such as GLUT-1 [Jans et al. 2010] and factor-inhibiting HIF-1 [Shaida et al. 2011].
Noninvasive multiparametric magnetic resonance imaging (MRI) modalities can be used to study the tumour microenvironment. Dynamic contrast-enhanced and dynamic susceptibility MRI (DCE-MRI and DSC-MRI) can provide information related to tumour blood flow, whilst intrinsic susceptibility weighted MRI (ISW-MRI, also known as blood oxygen level dependent MRI) can be used to assess relative changes in tumour oxygenation level [Li et al. 2011; Alonzi et al. 2007]. It has been demonstrated that ISW-MRI has high sensitivity in the detection of prostate hypoxia and a high negative predictive value when combined with blood volume information obtained through DSC-MRI [Hoskin et al. 2007]. The technical aspects of its use in this setting, in particular with regards to its reproducibility and correlation with information obtained from DCE-MRI scans, has been further evaluated [Alonzi et al. 2010]. As an alternative to nuclear medicine based imaging such as misonidazole positron emission tomography, MRI provides a noninvasive means to study prostate hypoxia in vivo without exposure to radiation.
Androgen withdrawal treatment prior to, or concomitant with, radiotherapy has been shown to improve the efficacy of prostate irradiation in many clinical trials [Bolla et al. 1997; Denham et al. 2005; D’Amico et al. 2008; Jones et al. 2011]. In vitro and in vivo studies have provided very strong evidence that androgen withdrawal leads to a reduction in tumour blood supply, possibly via the promotion of endothelial cells apoptosis [Lekas et al. 1997; Jain et al. 1998; Shabsigh et al. 1998; de la Taille et al. 1999; Hayek et al. 1999; Godoy et al. 2011]. This has been proposed as one of the numerous mechanisms whereby androgen deprivation can enhance the results of radiation therapy [Wo and Zietman, 2008]. However, the impact of this vascular degeneration on the oxygen status of the tumour environment is less clear. In one animal model study, the HIF-1α protein level was significantly elevated following castration, hence suggestive of an increase in hypoxia [Shabsigh et al. 2001]. The clinical evidence is inconclusive. Milosevic and colleagues, using direct microelectrode measurements, showed that pO2 increased after at least 3 months of treatment with the antiandrogen bicalutamide [Milosevic et al. 2007]. In contrast, Alonzi and colleagues showed the opposite after 3 months of goserelin treatment, as evaluated by ISW-MRI and DCE-MRI [Alonzi et al. 2011] (Figure 1). Reversing the hypoxic state may thus potentially further augment the ability of hormones to enhance the cytotoxicty of radiotherapy.

Effect of androgen deprivation of the oxygen status of the prostate as assessed on a magnetic resonance imaging scan. (a) T2W MRI image of the prostate of a patient before receiving neoadjuvant hormone treatment; (b) R2* maps of prostate in the same patient. The baseline R2* map is dark throughout the prostate, indicating no evidence of hypoxia; (c) after 1 month of androgen deprivation therapy; (d) after 3 months of androgen deprivation therapy, there was an increase in R2* across the prostate gland. (Reproduced with permission from Alonzi et al. [2011].)
Hypofractionated radiotherapy is when more than 2 Gray per fraction is used during the course of treatment. Different tumour types have different sensitivities to the radiation dose per fraction. In vitro studies have shown that in prostate cancer a higher clonogenic cell kill is achieved using higher doses per fraction, whilst keeping the same total radiation dose. The benefits in terms of therapeutic gain, reduced number of treatment visits and cost have led to a worldwide interest in the clinical application of hypofractionated radiotherapy schedules for the treatment of prostate cancer [Ritter, 2008]. Improvements in radiotherapy technology in the last decade have pushed the boundaries further to enable the dose per fraction during external beam radiotherapy to be escalated far beyond previous limits, a practice which has been termed ‘ultra-hypofractionation’ [Katz, 2010]. Both classical radiobiology in vitro studies and recent mathematical modelling [Carlson et al. 2011] have confirmed the detrimental effect of hypoxia on hypofractionation due to the insufficient time for reoxygenation to take place. In fact, the use of hypoxic modifiers has been shown to benefit moderately hypofractionated schedules more than conventionally fractionated schedules [Overgaard, 2007] and has been advocated in the era of ultra hypofractionation [Brown et al. 2010]. An ultra-hypofractionated schedule may have the advantage of being able to overcome the HIF-mediated vascular protective effect [Fuks and Kolesnick, 2005].
Preclinical studies of hypoxia modification during radiotherapy
Inhalation of hyperbaric oxygen (> 1 atmospheric pressure) during radiotherapy treatment provides the most direct means to raise pO2 in the blood. However, the practical difficulties in the simultaneous delivery of hyperbaric oxygen and radiotherapy in clinical trials, together with the increase in normal tissue side effects [Henk, 1986; Mayer et al. 2005], have lead researchers to favour alternative means to improve tumour oxygen supply.
Preclinical evidence supports the use of high concentrations of normobaric oxygen in conjunction with carbon dioxide and nicotinamide (the amide of vitamin B3, niacin). This gas mixture of oxygen and carbon dioxide is known as carbogen and is usually administered in a ratio of 95–98% oxygen and 2–5% carbon dioxide. Carbon dioxide acts to counteract the vasoconstrictive effect of pure oxygen whilst nicotinamide reduces the temporal microregional fluctuations in tumour blood flow which are responsible for acute hypoxia [Chaplin et al. 1990, 1993]. Alonzi and colleagues have demonstrated that carbogen inhalation could improve the oxygenation status in prostate tumour xenografts and in human prostate cancers as evaluated by ISW-MRI [Alonzi et al. 2009] (Figure 2).

Graph showing the change in the R2* values on the blood oxygen level dependent magnetic resonance imaging scan after the administration of carbogen. Changes in the median R2* values of the prostate among 14 patients before and after carbogen breathing. The mean reduction in R2* values was 21.6%. (Reproduced with permission from Alonzi et al. [2009].)
As discussed earlier, chronic hypoxia may render prostate cancer cells more radiosensitive by decreasing the synthesis of HR proteins [Sprong et al. 2006; Chan et al. 2008]. Chan and colleagues have shown in an ex vivo clonogenic assay that HR-deficient hypoxic cells pretreated with ABT-888, a PARP inhibitor [Sandhu et al. 2011], 24 h prior to being irradiated, had lower surviving fraction compared with the control [Chan et al. 2010]. The 24 h gap between the final dose of ABT-888 and 5 Gray irradiation ensured that the ABT-888 had been washed out completely from the system and thus any synergistic effects observed would be the result of prior SSB formation induced by ABT-888.
Clinical studies
A recently updated meta-analysis of hypoxia modification during radiotherapy has supported the beneficial impact of combining standard radiotherapy with different methods of hypoxic modification [Overgaard, 2007]. A total of 10,108 patients treated in 86 randomized trials were identified. The odds ratios for the outcome of loco-regional control and survival were 0.77 (95% confidence interval 0.71–0.86) and 0.87 (0.80–0.95) respectively in favour of the interventional group.
The various hypoxia modification strategies tested in early phase clinical trials have been comprehensively reviewed by Oronsky and colleagues [Oronsky et al. 2011]. However, only two of them have been incorporated into routine standard clinical practice. They are the use of nitro-imidazole compounds and carbogen with nicotinamide.
Nitro-imidazole compounds such as misonidazole, pimonidazole and nimorazole undergo reductive activation under hypoxic conditions. When they enter a viable cell they undergo a single electron reduction to form a potentially reactive species. In the presence of normal oxygen level they are immediately reoxidized. In hypoxic tissue the low oxygen concentration is not able to effectively compete to reoxidize them; further reductions thus take place, culminating in the association of the reduced nitroimidazole with various intracellular components. As mentioned earlier, these reduced nitro-imidazoles can mimic oxygen and ‘fix’ DNA damages induced by radiation. In the diagnostic setting, they are used to identify areas of hypoxia in immunohistochemical analyses and nuclear medicine imaging [Nunn et al. 1995]. Therapeutically, the concurrent administration of nimorazole during radiotherapy in the treatment of patients with pharyngeal and supra-glottic laryngeal carcinoma has become the standard in Denmark following the encouraging results of the pivotal Danish Head and Neck Cancer Study (DAHANCA 5). In this phase III randomized controlled trial, the use of nimorazole improved the 5-year local regional control rate from 33% to 49% [Overgaard et al. 1998]. Agents which are selectively cytotoxic against hypoxic cells are very attractive in principle. Tirapazamine is the most developed drug in this class. Despite its early promise, it has not been shown to augment the effect of radiation in a randomized phase III trial for patients with advanced head and neck cancer [Rischin et al. 2010].
The results from a number of phase II trials in the use of carbogen and nicotinamide (CON) have been promising [Kaanders et al. 2002]. Two phase III trials were reported last year. In the first trial, 333 patients with locally advanced bladder cancer (T2, T3 or T4a) were recruited in the UK [Hoskin et al. 2010]. They were randomized to receive either radiotherapy alone (RT) or radiotherapy plus CON. The radiotherapy regimes were identical in both arms (55 Gray in 20 fractions or 64 Gray in 32 fractions). The primary endpoint was local control as assessed by cystoscopic examination at 6 months, and secondary endpoints were overall survival, local relapse-free survival and urinary and rectal toxicities. The median follow-up times were 57 months and 60 months respectively for the control and combination arms. The 6-month cystoscopic control rates were 81% for the RT + CON group and 76% for the RT alone arm (p = 0.3). The 3-year overall survival rates were 59% for the combination arm and 46% for the RT alone arm (p = 0.04), thus representing a 13% absolute survival benefit in favour of the use of CON with RT. Late toxicities were similar in both groups.
A second trial conducted in the Netherlands involving 345 patients with locally advanced laryngeal cancer demonstrated a significant advantage for CON in terms of regional control rate amongst patients with hypoxic tumours as defined by pretreatment high pimonidazole staining [Kaanders et al. 2011]. In this group of patients, there was a 40% absolute difference in their 5-year regional control rate – 100% for the RT + CON group versus 60% for the RT alone group (p = 0.01). For patients with low pimonidazole staining there was no significant difference – the 5-year regional control rates were 90% (RT alone) and 94% (RT + CON).
Executive summary of this review.
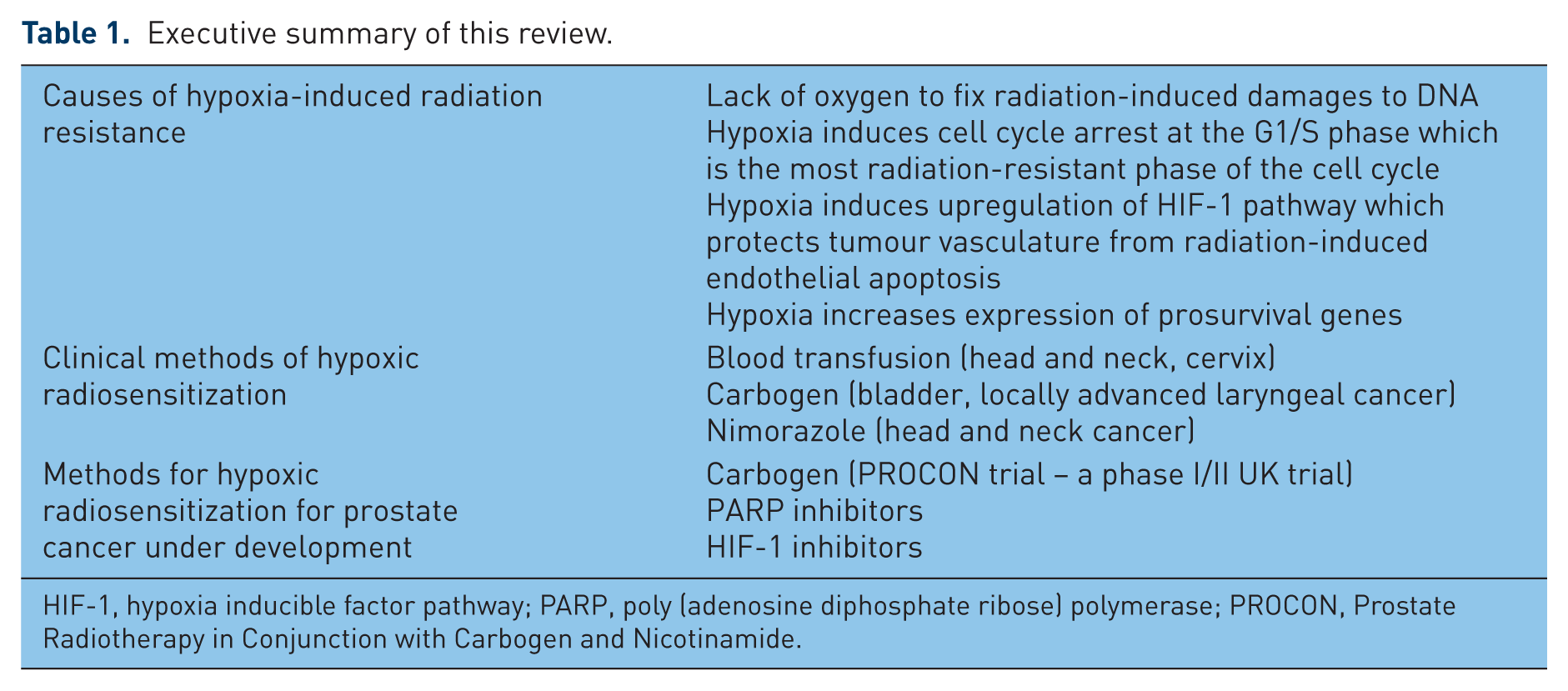
HIF-1, hypoxia inducible factor pathway; PARP, poly (adenosine diphosphate ribose) polymerase; PROCON, Prostate Radiotherapy in Conjunction with Carbogen and Nicotinamide.
Future directions: PROCON and PARP
The application of hypoxic modifiers in the treatment of prostate cancer has been slow compared with other cancers. Prostate radiotherapy research has mainly focused on the use of androgen deprivation, escalated radiotherapy dose, fractionation and the technical method of dose delivery. In contrast to the promising new targeted drugs that are under development [Begg et al. 2011], hypoxia modifications have attracted less commercial support.
A phase I/II study (PROCON) in the UK is now open to recruitment to assess the feasibility of using carbogen and nicotinamide in conjunction with radiotherapy in patients with locally advanced prostate cancer [Alonzi and Hoskin, 2010]. In addition to assessing the toxicity arising from this treatment regime, prostate tissue samples from the patients recruited will be analysed for expression of hypoxic markers, including HIF 1, osteopontin, GLUT-1, as well as markers for tumour vascularity (VEGF, CD 34) and cellular proliferation (Ki67). Multiparametric MRI scans, including ISW-MRI, DCE-MRI, DSC-MRI, DW-MRI, will be carried out in these patients both before and during their radiotherapy. Correlation between biological and imaging markers can thus be explored, and in vivo assessment of the changes in oxygenation status of the prostate in response to carbogen and nicotinamide during the course of radiotherapy can be assessed.
The results from three early phase clinical trials testing an oral PARP inhibitor appear to substantiate this concept of synthetic lethality whereby cells defective in their HR mechanism are particularly sensitive to PARP inhibition. In the one trial which was open to patients regardless of their BRCA status, durable objective antitumor activity was observed only in those with BRCA1 or BRCA2 mutations [Fong et al. 2009]. In two subsequent trials which specifically targeted those with the above mutations, objective response or stable disease were seen in 70% of patients with ovarian cancer [Audeh et al. 2010] and 80% of those with breast cancer [Tutt et al. 2010] – quite an impressive figure in a heavily pretreated population. Following the promising data in the use of PARP inhibitors in combination with radiotherapy in preclinical prostate cancer models [Dewhirst et al. 2008; Chan et al. 2010], early phase trials in the use of this class of drugs as radiosensitizers during prostate radiotherapy are planned [Chalmers et al. 2010].
Conclusion
Hypoxia poses a significant barrier to tumour eradication during radiotherapy for prostate cancer. Neoadjuvant androgen deprivation therapy prior to radiotherapy may potentially worsen tumour hypoxia, which could compromise the therapeutic gain achieved with hypofractionated schedules. Early phase clinical trials are currently under way to explore the use of carbogen, nicotinamide and PARP inhibitors to overcome this hypoxic barrier.
Footnotes
Acknowledgements
We are grateful for Professor Peter Hoskin for reviewing the manuscript and offering helpful advice.
Funding
The PROCON project and KY’s research fellowship are funded by a grant from the Prostate Cancer Charity, UK. RA’s senior lecturership is supported by the Medical Research Council, UK.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.