
Abstract
Around 70% of men presenting with prostate cancer will have organ-confined disease, with the majority presenting with low- or intermediate-risk prostate cancer. This article reviews the evidence supporting the current standard of care in radiation oncology for the evaluation and management of men with intermediate-risk prostate cancer. Dose escalation, hormonal therapy, combined modality therapy, and modern techniques for the delivery of radiation therapy are reviewed.
Keywords
Introduction
Prostate cancer is the most common cancer in men and the second most common cause of cancer death. Extrapolating from data gathered between 2005 and 2007, US men have a 16.2% lifetime risk of being diagnosed with prostate cancer. Around 70% of these patients will present with organ-confined disease, with the majority presenting with low- or intermediate-risk prostate cancer [Jemal et al. 2010].
Risk stratification into low-risk, intermediate-risk, and high-risk prognostic groups is based on prostate specific antigen (PSA), clinical tumor stage, and Gleason score, and dictates appropriate initial management options. Based on the work of D’Amico and colleagues, the following inclusion criteria are most commonly used to define the prognostic groups: the low-risk group includes stage T1c–T2a tumors, PSA ≤ 10 ng/ml and Gleason score ≤ 6; the intermediate-risk group includes those with stage T2b–T2c tumors, and PSA >10 but ≤20 ng/ml, and Gleason score 7; the high-risk group includes stage T3–T4 tumors, PSA > 20 ng/ml, and Gleason score 8–10 [D’Amico et al. 1998]. Intermediate-risk prostate cancer correlates with American Journal of Critical Care seventh edition group IIA [Edge et al. 2010]. Percentage of positive prostate biopsy cores, pretreatment PSA velocity, and presence or absence of perineural invasion observed on biopsy provide further prognostic information when selecting the most appropriate treatment strategy for individual patients. Patients with two or more intermediate risk factors have been noted to behave more similarly to patients at high risk [Briganti et al. 2007; D’Amico et al. 2004b, 2005]. This review focuses on the evaluation and management of men diagnosed with prostate cancer in the intermediate-risk category.
Pretreatment evaluation of patients with intermediate-risk prostate cancer
In addition to routine history and physical examination, including a digital rectal examination, serum PSA, and serum testosterone, radiographical imaging of the abdomen and pelvis using computed tomography (CT) or magnetic resonance imaging (MRI) should be obtained to assist in the evaluation of the extent of primary disease. Although the likelihood of bone metastases is low in men with intermediate-risk prostate cancer, bone scan may be appropriate for patients in whom there is high suspicion for metastatic disease based on laboratory, imaging, or clinical findings [Chybowski et al. 1991].
While CT imaging of the pelvis is the current standard, T2 MRI is superior to CT as it provides adequate soft tissue resolution to delineate the anatomy of the prostate, seminal vesicles, neurovascular bundles, and pelvic floor. MRI offers the ability to detect disease within and adjacent to the prostate gland that is not as easily visualized on CT [Flanigan et al. 1996; Heesakkers et al. 2008]. MRI, if obtained, can be fused to treatment planning CTs, allowing improved accuracy in contour definition of target and normal tissue volumes [Kagawa et al. 1997; Rasch et al. 1999; Roach, 1996]. This may result in improved clinical outcomes by decreasing normal tissue toxicity [Villeirs and De Meerleer, 2007]. MRI and magnetic resonance spectroscopy may have a role in the evaluation of tumor response to external beam radiation therapy (EBRT) and prostate brachytherapy (BRT) [Mazaheri et al. 2011; Pickett et al. 2004; Pucar et al. 2005].
Clinical trials
The rationale driving the current standard of care for intermediate-risk prostate cancer is predicated on the results of several prospective, randomized controlled trials. These trials can be generally divided into two broad categories: dose escalation trials and conventional dose radiation therapy (RT) with or without androgen deprivation trials. The most significant improvements in disease control and overall survival have been observed with the addition of neoadjuvant hormonal therapy (NHT) to conventional dose RT [Bolla et al. 2010; Crook et al. 2004, 2009; D’Amico et al. 2004a, 2008; Denham et al. 2005, 2011; Laverdiere et al. 1997; McGowan et al. 2010; Roach et al. 2008].
The dose escalation trials established that high-dose RT delivered via a conformal technique [78–81 Gray (Gy) delivered to the prostate] is well tolerated and results in significant improvement in freedom from biochemical failure and disease-free survival versus conventional dose (64–70 Gy) regimens for men with intermediate-risk prostate cancer, although it has not been shown to confer an overall survival advantage [Al-Mamgani et al. 2008; Dearnaley et al. 2007; Kuban et al. 2008; Peeters et al. 2002, 2006; Sathya et al. 2005; Shipley et al. 1995; Zietman et al. 2005, 2010]. The trials evaluating the addition of hormonal blockade to RT demonstrated improvement in local control, disease-free survival, cancer-specific survival, and overall survival. Studies are currently underway evaluating the optimal combination of dose escalation with hormonal therapy, as well as the optimal duration of androgen deprivation therapy for patients with intermediate-risk prostate cancer.
Dose-escalation trials
Prior to the advent of three-dimensional conformal RT (3DCRT), 70 Gy was established as the maximal tolerable dose due to limitations conferred by rectal and bladder toxicity [Lawton et al. 1991; Pilepich et al. 1987b]. With improved dose conformality, the ability to safely deliver higher doses to the prostate was established, and resultant improvements, especially in biochemical progression-free survival, were seen.
MD Anderson Cancer Center 93-002
This trial evaluated the effect of dose escalation from 70 to 78 Gy on freedom from failure, and was among the first to include biochemical (PSA) freedom from failure as an endpoint. Between 1993 and 1998, 301 patients with T1–T3 tumors, including 139 patients with intermediate-risk cancer, were randomized to receive 70 or 78 Gy via EBRT to the prostate gland. All patients received an initial 46 Gy in 2 Gy daily fractions via a four-field box technique. Following delivery of 46 Gy, each group received a 3DCRT boost commensurate with their remaining prescribed total dose, such that the conventional dose arm received an additional 24 Gy via a four-field technique, and the high-dose arm received a 32 Gy boost via a six-field technique. At 8-year follow up, freedom from biochemical failure favored the 78 Gy arm, 59% versus 78% (p = 0.04). The subset of patients with an initial PSA of more than 10 ng/ml gained the greatest benefit from dose escalation with 78% versus 39% freedom from failure (p < 0.001). Among patients with intermediate-risk cancer, the subset with pretreatment PSA greater than 10 ng/ml similarly benefitted most substantially from dose escalation, with biochemical freedom from failure of 94% versus 65% (p = 0.076) [Kuban et al. 2008; Pollack et al. 2002]
Notably, the rate of Radiation Therapy Oncology Group (RTOG) grade 2 or greater rectal toxicity was 14% higher in the 78 Gy arm and was found to correlate with the volume of rectum receiving at least 70 Gy [Kuban et al. 2008]
Proton Radiation Oncology Group 95–09
This trial evaluated the effect of dose escalation from 70.2 to 79.2 Gray equivalents (GyE) on local failure, biochemical failure, and overall survival in patients with localized prostate cancer. A total of 393 patients with stage T1b–T2b prostate cancer and PSA levels less than 15 ng/ml were randomized to receive EBRT to a total dose of either 70.2 or 79.2 GyE delivered via conformal photon therapy with conformal proton boost. The prostate gland plus a 12–15 mm margin received a conformal proton dose of 19.8 or 28.8 GyE in 1.8 GyE fractions. Subsequent to initial proton treatment, all patients received 50.4 Gy to the prostate gland and seminal vesicles plus a 10 mm margin via a conformal four-field technique. At 10-year follow up, biochemical failure rates were halved from 32.3% for the conventional dose arm to 16.7% for the dose-escalated arm. High-dose therapy conferred improved outcomes in all risk groups, though this was only statistically significant for those with low-risk disease (58% of the cohort) in which 28.2% of those receiving conventional dose therapy failed versus 7.1% of those receiving high-dose therapy (p = 0.0001). Patients with intermediate-risk cancer trended toward a benefit with high-dose RT, though the study was not powered to detect differences on subgroup analysis, and this result did not reach statistical significance. Patients with intermediate-risk cancer represented 37% of the cohort. Of these patients, 42.1% receiving conventional dose therapy failed to respond versus 30.4% who received the dose-escalated regimen (p = 0.06) [Shipley et al. 1995; Zietman et al. 2010].
Dutch Trial CKTO 6910
This trial was conducted to evaluate the effect of dose escalation from 68 to 78 Gy on freedom from failure. To that end, 669 patients with stage T1b–T4 prostate cancer at four institutions in the Netherlands were randomized to receive either 68 or 78 Gy via a 3DCRT technique. The clinical target volume (CTV) included the prostate plus or minus the seminal vesicles depending on assessed risk for seminal vesicle involvement based on the Partin method. Planning target volume (PTV) included a 10 mm expansion for the initial 68 Gy for all patients, followed by an additional 10 Gy with 5 mm expansion, except 0 mm toward the rectum, for patients receiving 78 Gy. In two institutions, neoadjuvant hormone therapy was prescribed for some, mostly patients with high-risk cancer. The study was not statistically powered to detect a difference due to the addition or withholding of hormonal therapy. With 4 years of follow up, the freedom from biochemical failure was 64% in the high-dose arm versus 54% in the low-dose arm (p = 0.02). There was no significant difference in overall survival between the treatment arms. For patients with intermediate-risk cancer, there was a statistically significant 15% improvement in freedom from failure in the high-dose arm [Peeters et al. 2006].At 70 months of follow up, the 7-year biochemical control rates continued to favor the high-dose arm, 56% versus 45%, p = 0.03. The cumulative incidence of late grade 2 or greater gastrointestinal (GI) toxicity manifested by rectal bleeding and incontinence was increased in the 78 Gy arm compared with the 68 Gy arm (35% versus 25% at 7 years; p = 0.04) [Al-Mamgani et al. 2008]
Medical Research Council RT01 trial
This trial sought to evaluate whether NHT combined with dose-escalated RT (74 Gy versus 64 Gy) would improve cancer control as measured by biochemical progression-free survival, freedom from local progression, metastasis-free survival, and overall survival, without a prohibitive increase in treatment-associated toxicity compared with NHT followed by standard dose RT. This is the largest randomized prospective dose-escalation trial, and the only one to prescribe NHT uniformly to all patients.
A total of 843 men with stage T1b–T3a, N0, M0 prostate cancer, and serum PSA of less than 50 ng/ml first received between 3 and 6 months of NHT and were randomly assigned to receive 64 Gy over 32 fractions in 6.5 weeks or 74 Gy over 37 fractions in 7.5 weeks.
The gross tumor volume for all patients included the prostate gland and all or a portion of the seminal vesicles, depending on the risk group. In patients with low-risk cancer, gross tumor volume (GTV) included the base of the seminal vesicles, and in patients with intermediate- and high-risk cancer, all of the seminal vesicles. A 5 mm expansion was made from GTV to CTV and a subsequent 5 mm to 1 cm expansion from CTV was made to PTV. Biochemical progression-free survival at 5 years (63 months average) favored the patients on dose-escalation therapy across all risk groups, 71% versus 60% (p = 0.0007), and in the intermediate-risk group, by 9 percentage points (79% versus 70%). There was no observed difference in freedom from local progression or overall survival. There was an increased incidence of late GI toxicity and genitourinary (GU) toxicity in the 74 Gy arm [Dearnaley et al. 2007].
As a group, these trials demonstrated a benefit for dose-escalated RT for intermediate-risk prostate cancer in terms of biochemical freedom from failure and local control, but failed to demonstrate an improvement in overall survival. Table 1 summarizes the outcomes of the dose-escalation trials. Overall, GI and GU toxicity in the high-dose arms were increased versus The conventional dose arms, with the exception of those treated with protons. A caveat is that these trials were conducted prior to the advent of intensity modulated RT (IMRT) or did not allow this therapy, which has permitted substantial improvements in the conformality of delivered doses and resultant reduction in normal tissue dose profiles and toxicity. The results of RTOG 0126 will provide prospective evaluation of toxicity and survival outcomes for dose escalation to 79.2 Gy versus 70.2 Gy delivered via a 3DCRT/IMRT technique for patients with intermediate-risk cancer.
Dose escalation trials.
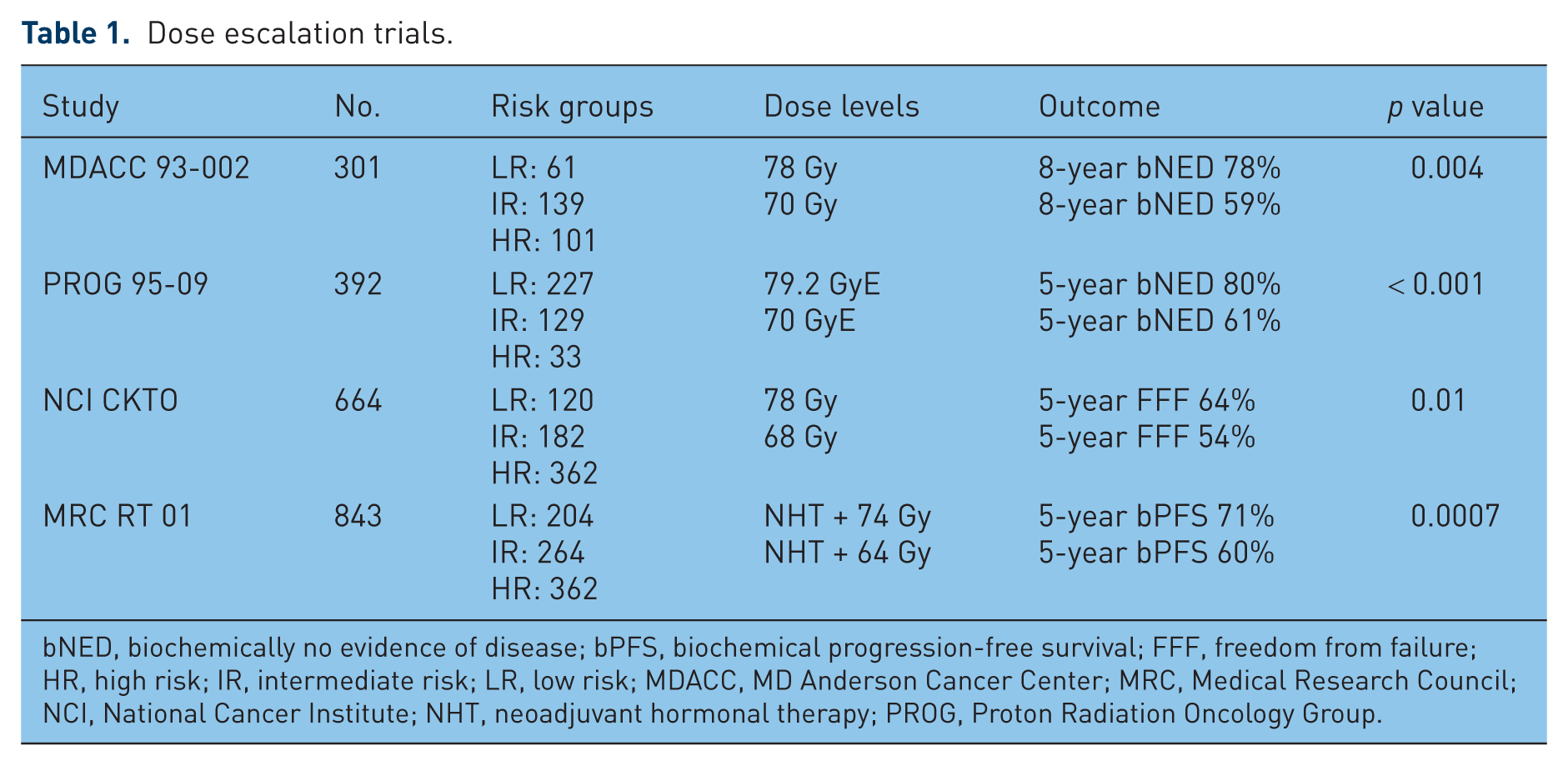
bNED, biochemically no evidence of disease; bPFS, biochemical progression-free survival; FFF, freedom from failure; HR, high risk; IR, intermediate risk; LR, low risk; MDACC, MD Anderson Cancer Center; MRC, Medical Research Council; NCI, National Cancer Institute; NHT, neoadjuvant hormonal therapy; PROG, Proton Radiation Oncology Group.
Radiation therapy with or without hormonal therapy
Dana Farber Cancer Institute Trial
This trial sought to evaluate the effect of the addition of androgen deprivation therapy to RT on survival, disease-specific mortality, survival free from salvage hormonal therapy, and all-cause mortality. To this end, 206 men with T1b–T2b, N0, M0 adenocarcinoma of the prostate and either a Gleason score of at least 7 (5–10), a serum PSA of at least 10 ng/ml, or, in patients with low-risk cancer, MRI evidence of extra-prostatic disease or seminal vesicle invasion, were randomized to receive 70 Gy via 3DCRT alone or in combination with 6 months of androgen suppression therapy (AST). All patients received an initial 45 Gy to the prostate and seminal vesicles followed by an additional 25.35 Gy boost to the prostate plus a 1.5 cm margin via a four-field 3DCRT technique. Leuprolide or goserelin were used in combination with flutamide to achieve androgen blockade. At a median 4.52 years of follow up, patients randomized to receive combined modality therapy (CMT) had significantly higher survival, lower prostate-cancer-specific mortality, and higher survival free of salvage hormonal therapy. Five-year survival rates favored CMT by 10 percentage points (88% versus 78%). At 7.6 years of follow up, the Kaplan–Meier 8-year survival estimates were 74% and 61% respectively for patients receiving AST versus those receiving RT alone. The increased risk in all-cause mortality was significant only in those patients randomized to RT with or without minimal comorbid pretreatment disease [D’Amico et al. 2004a, 2008].
Radiation Therapy Oncology Group 94-08
This multi-institutional study was conducted to evaluate the effect of the addition of AST to RT on overall survival, freedom from biochemical failure, freedom from clinical progression, and disease-free survival in patients with localized prostate cancer in response to the positive effect on these parameters seen in RTOG 86-10. To this end, 1979 patients with T1b–T2b prostate cancer and PSA less than 20 ng/ml were randomized to receive EBRT alone or in conjunction with 2 months of neoadjuvant and 2 months of concurrent goserelin and flutamide.
Radiation treatment with and without hormonal therapy trials.

ADT, androgen deprivation therapy; HR, high risk; IR, intermediate risk; LR, low risk; NACHT, neo adjuvant concurrent hormonal therapy; NHT, neoadjuvant hormonal therapy; OS, overall survival; RT, radiation therapy; RTOG, Radiation Therapy Oncology Group; TROG, Trans-Tasman Radiation Oncology Group.
All patients received 46.8 Gy in 26 1.8 Gy fractions to the regional lymphatics followed by 19.8 Gy in 1.8 Gy fractions to the prostate alone for a total of 66.6 Gy. At 8 years of follow up, the overall survival rate was 62% with combined therapy and 57% with RT alone. The benefit was most pronounced in patients with intermediate-risk cancer receiving CMT, who had an overall survival rate of 72% (versus 66% in the RT alone arm), disease-specific survival of 98% (versus 92%), a biochemical control rate of 75% (versus 58%), and a number needed to treat of 17. The overall survival rate was 66% versus 58%, favoring CMT in patients with high-risk cancer, and was not statistically significant (76% versus 73%) in patients with low-risk cancer [McGowan et al. 2010].The 10-year death rate excluding deaths from prostate cancer was 35% in the CMT and 37% in the radiation-only arms, supporting the conclusion that the addition of short-course hormonal blockade to RT did not increase the risk of death from comorbid disease [McGowan et al. 2010].
Trans-Tasman Radiation Oncology Group 96.01
This trial sought to evaluate the effect of the addition of androgen deprivation therapy of 0, 3, or 6 months to RT on time to local failure, prostate-cancer-specific survival, distant failure, disease-free survival, and freedom from salvage treatment for patients with locally advanced prostate cancer. A total of 802 evaluable men with T2b, T2c, T3, or T4, N0, M0 prostate cancer were randomized to receive one of three treatment regimens: 66 Gy in 33 fractions to the prostate and seminal vesicles alone; 66 Gy plus 3 months of neoadjuvant and concurrent ADT; or 3. 66 Gy plus 6 months of neoadjuvant and concurrent ADT. ADT was with goserelin and flutamide. At a median follow up of 5.9 years, the results of this trial showed a benefit for 3 or 6 months of neoadjuvant ADT in terms of distant failure-free, prostate-cancer-specific survival, local control, biochemical failure-free survival, disease-free survival, and freedom from salvage treatment versus RT alone. The results were not consistent between the 3- and 6-month groups, and favored 6 months of neoadjuvant and concurrent ADT with RT [Denham et al. 2005].
At 10.6-year median follow up, both CMT arms showed benefit in freedom from biochemical progression, freedom from local failure, and event-free survival compared with RT alone. Greater improvement was again seen for 6 months versus 3 months of CMT for each of these parameters. Six months of CMT additionally conferred improved freedom from distant progression, prostate-cancer-specific mortality, and overall survival while no improvement was seen in these parameters with 3 months of CMT [Denham et al. 2011].
No increase in treatment-related morbidity was seen with CMT.
Hypofractionation, stereotactic body radiation therapy and high-dose rate monotherapy
Hypofractionation for the treatment of prostate cancer has recently experienced renewed interest based on radiobiological properties of tumor cells and resultant theoretical improvements in the therapeutic ratio with increased fraction sizes. While most tumors have α/β ratios around 8, prostate cancer cells are postulated to have an α/β ratio of 2. As the rectum is the major dose-limiting structure for the delivery of radiation to the prostate, and has a higher α/β ratio estimated at 4–6, it follows that hypofractionation should permit greater tumor killing without an attendant increase in the incidence of late toxicity [Brenner et al. 2002; Fowler et al. 2003]. Several randomized and nonrandomized trials have demonstrated the feasibility, tolerability, and noninferiority of hypofractionated regimens [Kupelian et al. 2007; Martin et al. 2007; Norkus et al. 2009a, 2009b; Pollack et al. 2006].
In a representative single institution series from the Cleveland Clinic, 770 patients received 70 Gy over 28 fractions via an IMRT technique. At 45 months of median follow up biochemical control rates were 94% in low-risk, 83% in intermediate-risk, and 72% in high-risk groups. There was no increase in acute or late GI or GU toxicity [Kupelian et al. 2007].
Based on the same radiobiological principles, and in concert with the development of emerging technologies and patient preferences, limited initial single institution experiences with stereotactic body RT (SBRT) and high-dose rate (HDR) monotherapy approaches to extreme hypofractionation have shown promising results but require further evaluation [Aluwini et al. 2010; Boike et al. 2011; Buyyounouski et al. 2010; King et al. 2009; Macías and Biete, 2009; Madsen et al. 2007].
Low-dose rate brachytherapy
Permanent prostatic seed implantation with iodine-125 (I-125) or palladium-103 (Pd-103) sources confers excellent tumor control and survival outcomes with minimal toxicity in the treatment of patients with early and intermediate-risk prostate cancer. Generally, patients with low-risk prostate cancer, prostates less than 50 cm3, and low International Prostate Symptom Score (IPSS) scores are eligible for primary BRT, while patients with intermediate-risk prostate cancer with similar physical characteristics are eligible for a BRT boost following EBRT to the pelvis. Innovations in treatment planning and delivery for BRT including transrectal ultrasound, template-based transperineal implantation, real-time treatment planning, and CT-based postimplant dosimetry evaluation ensure accurate dose delivery and avoidance of dose to normal tissue. Unlike external beam techniques, BRT dosimetry is not subject to intratreatment variability due to movement of the internal anatomy.
In patients with intermediate-risk prostate cancer, prostate BRT is recommended for use only as a boost therapy following EBRT. A standard regimen delivers 45 Gy to the pelvis via an external beam technique and subsequent implantation of I-125 or Pd-103 seed sources into the prostate. The Seattle Prostate Institute reported their long-term experience treating 223 patients with T1–T3 prostate cancer with an I-125 or Pd-103 PPI boost at a median interval of 4 weeks following 45 Gy delivered via EBRT to the prostate gland and seminal vesicles. The Pd-103 boost prescribed 100 Gy and the I-125 boost prescribed 108 Gy. At 15-year follow up, biochemical relapse-free survival for patients with low-risk, intermediate-risk and high-risk cancer was 88%, 80%, and 53% respectively [Sylvester et al. 2003, 2007].
A representative series comparing the effects of dose escalation for localized prostate cancer treatment with IMRT or permanent transperineal BRT versus conventional dose 3DCRT was published by Wong and colleagues from the Mayo Clinic Scottsdale. Of 853 evaluated patients, 270 received conventional dose 3DCRT, 314 received high-dose IMRT, 225 received BRT, and 44 received EBRT plus BRT boost. The median radiation doses were 68.4 Gy for 3DCRT and 75.6 Gy for IMRT. Patients receiving BRT had a prescribed dose of 144 Gy with I-125 or 120 Gy with Pd-103 respectively. Patients treated with EBRT plus BRT received 45 Gy of EBRT plus a boost of 110 Gy with I-125 or 90 Gy with Pd-103. At a median follow up of 58 months, the 5-year biochemical control rates were 74% for 3DCRT, 87% for IMRT, 94% for BRT, and 94% for EBRT plus BRT (p < 0.0001). For the intermediate-risk group, high-dose IMRT, BRT, or EBRT plus BRT achieved significantly better biochemical control rates than 3DCRT (p < 0.0001) [Wong et al. 2009].
The absence of randomized controlled data supporting improvement in outcome versus other available treatment modalities and the high cost of combination therapy are relative arguments against the use of BRT boost.
High-dose rate brachytherapy boost
As discussed above, the low α/β ratio for prostate cancer relative to the dose-limiting rectum confers an improved therapeutic ratio with the higher doses per fraction delivered via HDR. HDR versus LDR brachytherapy allows elimination of radiation exposure to patient contacts, shorter overall treatment times, and the opportunity to optimize dose distribution by varying source dwell times and positions within the target volume. Ten-year outcomes of 22–24 Gy delivered via iridium-192 after loading following 36 Gy EBRT were published by Demanes and colleagues from the California Endocurietherapy Cancer Center. Biochemical progression-free survival was 90%, 87%, and 69% for patients with low-, intermediate-, and high-risk cancer, respectively [Demanes et al. 2005]. Vargas and colleagues reported 5-year results of a prospective trial conducted at William Beaumont Hospital evaluating high-dose versus low-dose HDR boost following 46 Gy of pelvic irradiation for patients with intermediate- and high-risk prostate cancer. The HDR group received more than 268 Gy biologically equivalent dose (BED) boost between 17.5 and 23 Gy in two fractions and the LDR group received less than 268 Gy BED between 16.5 Gy in three fractions and 16.5 Gy in two fractions to the prostate. Five-year biochemical failure favored the high-dose group (68.7% versus 86%, p < 0.001), as did clinical event free survival (75.5% versus 91.7%, p = 0.003), cause-specific survival (95.4% versus 100%, p = 0.02), and overall survival (86.2% versus 97.8%, p = 0.002) [Vargas et al. 2006]. A median 8.2-year follow up of 472 patients from the same institution demonstrated a continued advantage to the HDR group from the perspective of biochemical failure, 43.1% versus 18.9% (p < 0.001), clinical failure, 23.4% versus 7.7% (p < 0.001), and distant metastasis, 12.4% versus 5.7% (p = 0.028) [Martinez et al. 2011].
Toxicity of radiation therapy and hormone therapy
RT is generally well tolerated, with certain prognostic factors such as prior transurethral resection of prostate, pretreatment IPSS score, American Urological Association score, anticoagulant use, inflammatory bowel disease, and radiation technique predicting an increased propensity to develop complications. Commonly reported acute symptoms include urinary frequency, urgency, nocturia, diarrhea, and tenesmus. These symptoms are usually well controlled with supportive care, α blockers, loperamide and steroid suppositories, and resolve shortly after completion of therapy. Urethral strictures, hematuria, hematochezia, proctitis, and incontinence occur infrequently at 1–3 years post treatment. Urethral dilatation, argon plasma laser coagulation, formalin therapy and hyperbaric oxygen have been reported as effective treatments for these late toxicities. Improvements in toxicity profiles have been demonstrated for advances in RT technologies, and are summarized below.
Toxicity of conventional two-dimensional planning
Over 1000 patients treated on RTOG trials 7506 and 7706 were followed for a minimum of 7 years and had a reported incidence of at least grade 3 bowel complications of 3.3% and a reported incidence of grade 3 or greater urinary complications in 7.7% of patients. These trials established 70 Gy as the maximal tolerable dose prior to the advent of conformal planning techniques [Pilepich et al. 1987a, 1987b]
Toxicity of three-dimensional conformal radiotherapy
RTOG 9406 evaluated the development of grade 3 or greater GI or GU toxicity in five dose levels from 68.4 to 79.2 Gy delivered via a 3DCRT technique. Group 1 patients had no elective seminal vesicle irradiation. Group 2 patients received treatment of the prostate and seminal vesicles with 54–55.8 Gy followed by a prostate boost. Rates of grade 2 or greater GI toxicity rates were 9%, 7%, 11%, 10%, and 25% for group 1 and 13%, 9%, 14%, 16%, and 26% for group 2 at 68.4 in 1.8 Gy fractions, 73.8 Gy in 1.8 Gy fractions, 79.2 Gy in 1.8 Gy fractions, 74.0 Gy in 2.0 Gy fractions, and 78.0 Gy in 2.0 Gy fractions respectively. The incidence of grade 2 or greater GU toxicity were 24%, 22%, 18%, 29%, and 23% for group 1 and 19%, 16%, 21%, 21%, and 28% for group 2. This trial demonstrated the reduction in toxicity, particularly in grade 3 or greater toxicity, despite radiation doses that were more than 10 Gy higher when conformal techniques were used [Michalski et al. 2010].
Toxicity of intensity-modulated radiation therapy
Similar to the improvements seen with the advent of 3DCRT versus conventionally planned two-dimensional RT (2DRT), IMRT techniques have allowed the same or higher radiation doses to be delivered with a reduction in grade 2 and grade 3 urinary and rectal complications. As detailed by Zelefsky and colleagues, 561 patients treated with IMRT at Memorial Sloan Kettering Cancer Center to 81 Gy had an 8-year likelihood of developing grade 2 rectal toxicity of 1.6%. Eight-year grade 2 or 3 urinary toxicity rates were 9% and 3% respectively [Zelefsky et al. 2006].
Toxicity of brachytherapy
Urinary obstructive symptoms due to inflammation and irritation of the prostate gland caused by procedure-related trauma and bleeding immediately after, and later due to radiation effect, are the most commonly reported adverse sequelae of brachytherapy. Inflammatory symptoms due to radiation are temporally related to the half life of the implanted isotope. The average onset is 1 month post procedure and symptoms peak between that time and 4 months post treatment. Treatment with α blockers and nonsteroidal anti-inflammatory drugs are sufficient to address symptoms in most patients. Acute urinary retention occurs in the immediate post-procedure period and ranges from 5% to 15% depending on preimplant lower urinary tract symptom scores and prostate volume [Crook et al. 2002]. The incidence of urethral strictures is reported to be between 2% and 12% of patients following prostate BRT [Landis et al. 2002]. Grade 2 rectal toxicity has been reported to be between 2% and 10%. Higher grade urinary or rectal toxicity is less than 2% [Stone and Stock, 2002]. Erectile dysfunction occurs in 40–50% of patients, of whom approximately 80% can be effectively treated with sildenafil citrate [Landis et al. 2002; Merrick et al. 2000, 2003; Stone and Stock, 2002].
Second malignancies
RT is known generally to be associated with an increased risk for the development of second primary cancers within the radiation field. This is particularly true for young patients with long post-treatment survival. For patients with prostate cancer, particularly in the era of modern RT techniques, the increased risk of second primary cancer is not yet known. A matched pair retrospective study comparing 2120 patients receiving RT at a single institution on a 1:1 basis with surgical patients according to age and follow-up time was recently reported. RT techniques consisted of conventional or 2DRT (36%), 3DCRT and IMRT (29%), BRT (16%), and a combination of 2DRT and brachytherapy (BT) (19%).
They found that the overall risk of developing a second primary cancer was not significantly different between the matched pair [hazard ratio (HR) 1.14, 95% confidence interval (CI) 0.94–1.39]. Additionally, they noted that the risk became significant more than 5 years (HR 1.86, 95% CI 1.36–2.55) or more than 10 years after RT (HR 4.94, 95% CI 2.18–11.2). The most significant sites of increased risk were bladder, lymphoproliferative, and sarcoma. Of the different RT techniques, only 2DRT was associated with a significantly higher risk (HR 1.76, 95% CI 1.32–2.35), but not BT boost (HR 0.83, 95% CI 0.50–1.38), 3DCRT/IMRT (HR 0.81, 95% CI 0.55–1.21), or BT (HR 0.53, 95% CI 0.28–1.01) [Huang et al. 2011].
Androgen deprivation therapy
Commonly reported side effects of ADT include fatigue, hot flashes, osteoporosis, weight gain, loss of libido, gynecomastia, erectile dysfunction, and anemia [Sharifi et al. 2005]. Less commonly reported adverse sequelae include loss of muscle mass, hypogonadism, hyperlipidemia, hyperglycemia, cardiac events, deep vein thrombosis, and depression [Bolla et al. 2007]. Supplemental vitamin D and calcium, and a prescribed diet and exercise regimen have been found to be beneficial for these patients. Long-term data from randomized trials have not shown an increase in cardiovascular mortality rates among patients receiving short-term (4–6 months) or long-term (2–3 years) AST with RT [Bolla et al. 2002; Efstathiou et al. 2008, 2009].
Conclusions
Evidence supports that patients with intermediate-risk prostate cancer have an overall survival benefit when treated with NHT and conventional dose RT versus conventional dose radiation therapy, and they have a benefit in biochemical freedom from failure when treated with a dose of 78–81 Gy versus 70 Gy RT. The role of hormonal therapy in the context of dose-escalated RT, including optimal duration of hormonal therapy and optimal dose of radiation when given with hormonal therapy, remain unclear, though studies have been completed or are underway that will help to clarify these questions. HDR and LDR boost may confer similar biochemical freedom from failure with shorter treatment times and fewer side effects, though at significantly higher cost. Hypofractionation may also confer equivalent or improved outcomes, in this case with shorter treatment times and at lower cost, but requires further evaluation. A multitude of modern therapeutic modalities exist that can technically deliver highly conformal radiation to the prostate, but phase III evidence is lacking to demonstrate superiority of one technique compared with another. The use of RT technologies should be based on prospective assessment of quality of life and modeling of cost effectiveness.
Emerging therapeutic modalities such as SBRT and HDR BRT monotherapy are promising areas of future investigation, especially given confirmatory evidence regarding the α/β ratio in prostate cancer. Highly conformal treatment delivery techniques, improved intratreatment evaluation, and improved pretreatment target localization and registration have significantly decreased the incidence of serious toxicity secondary to RT.
Footnotes
The views expressed in this presentation are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States government.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
DG is a military service member (or employee of the US Government). This work was prepared as part of his official duties. Title 17, USC, §105 provides that ‘Copyright protection under this title is not available for any work of the US Government’. Title 17, USC, §101 defines a US Government work as a work prepared by a military service member or employee of the US Government as part of that person’s official duties.