
Abstract
Background:
Current guidelines consider mechanical thrombectomy (MT) reasonable for M2 segment middle cerebral artery (MCA) occlusions within 6 h of symptom onset, yet the impact of delayed intervention in this population remains unclear.
Objectives:
This study compared effectiveness and safety outcomes of MT performed in late (>6 h) versus early (⩽6 h) treatment windows in patients with acute primary embolic M2 occlusions.
Design:
We retrospectively analyzed patients with primary embolic M2 occlusions treated with MT within 24 h of onset from the ARTISTA (A Registry for Thrombectomy In Stroke Therapy from Andalusia) registry (2017–2024) in Seville-Huelva, Spain.
Methods:
Outcomes compared between late and early treatment groups included good outcome (90-day modified Rankin Scale (mRS) 0–2 or return to prestroke mRS), futile recanalization (FR; 90-day mRS >2 despite successful recanalization), successful recanalization (modified Thrombolysis in Cerebral Infarction ⩾2b), and symptomatic intracranial hemorrhage (sICH). Multivariable logistic regression and inverse probability of treatment weighting (IPTW) analyses were performed to evaluate associations between treatment window and MT outcomes.
Results:
Among 524 patients (median age 76, 48.3% women), 207 (39.5%) underwent MT in the late window. Late treatment showed numerically lower rates of good outcome (58.9% vs 64.4%) and higher rates of FR (37.8% vs 32.5%) and sICH (3.4% vs 3.2%), though none were statistically significant (all p ⩾0.211). Successful recanalization rates were nearly identical between the late and early windows (95.7% vs 95.6%; p = 0.970). IPTW-adjusted analyses also found no significant differences in good outcome (adjusted odds ratio (aOR), 0.82; 95% confidence interval (CI), 0.39–1.73; p = 0.600) or FR (aOR, 1.19; 95% CI, 0.56–2.50; p = 0.653) at 90 days.
Conclusion:
In this multicenter real-world cohort, MT performed beyond 6 h showed effectiveness and safety outcomes comparable to early-window intervention in patients with primary embolic MCA M2 occlusions.
Plain language summary
When a blood vessel in the brain becomes blocked, restoring blood flow quickly is essential. Mechanical thrombectomy—a procedure in which doctors remove the clot directly—is commonly used for large-vessel strokes. However, for blockages in a smaller vessel called the M2 segment of the middle cerebral artery, current guidelines mainly support treatment within the first 6 hours after symptoms begin. Whether patients who arrive later can still benefit has remained uncertain. In this study, we examined real-world data from more than 500 patients in Spain who had an M2 stroke caused by an embolus. All patients received thrombectomy within 24 hours of symptom onset. We compared those treated early (within 6 hours) with those treated later (after 6 hours) to understand whether timing affected recovery or safety. We found that patients treated after 6 hours did not have worse outcomes than those treated earlier. Their chances of returning to independence were similar, as were the rates of successful restoration of blood flow. Importantly, the risk of complications—such as bleeding in the brain—was also comparable. Even after adjusting for age, stroke severity, and other medical factors, delayed treatment did not appear to reduce the potential benefit of thrombectomy. These findings suggest that, for carefully selected patients with M2 occlusions, performing thrombectomy after 6 hours may still be effective and safe. While more prospective research is needed, this study provides encouraging real-world evidence that could help guide clinical decisions and support broader treatment options for patients who arrive beyond the traditional time window.
Keywords
Introduction
Middle cerebral artery (MCA) M2 segment occlusions account for approximately 4% of acute ischemic stroke (AIS) admissions, 1 with 45%–60% of patients failing to achieve functional independence and 20%–24% dying within 6 months.2,3 Although intravenous tissue plasminogen activator yields higher recanalization rates in M2 occlusions than in proximal occlusions,4,5 over half of patients do not achieve partial or complete recanalization.6,7 Mechanical thrombectomy (MT) is being increasingly performed for M2 occlusions, 8 reflecting growing recognition of its potential to improve procedural efficacy and clinical outcomes.
Previous studies suggest that earlier treatment is associated with improved thrombectomy outcomes in patients with M2 occlusions treated within the early window.9–12 A meta-analysis 9 of randomized clinical trials (RCTs) demonstrated the superior efficacy of endovascular treatment (EVT) over best medical treatment (BMT) in achieving 90-day functional independence for acute M2 occlusions treated within 6 h, with some cases extending up to 8 or 12 h. Similarly, a multicenter retrospective cohort study revealed that EVT-treated patients presenting within 8 h of last known normal achieved better outcomes compared to those receiving BMT, while comparable safety profiles. 10 Additionally, patients undergoing MT within this timeframe had reperfusion rates and functional outcomes similar to those with M1 occlusions. 11 Current guidelines from the American Stroke Association, 13 European Stroke Organisation, 14 and Japan Stroke Society 15 also consider MT as a reasonable treatment for MCA M2 occlusions within 6 h of symptom onset.
However, the impact of delayed treatment beyond 6 h in patients with M2 occlusions remains poorly characterized. Two recent RCTs, ESCAPE-MeVO 16 and DISTAL, 17 reported findings on extended-window thrombectomy. ESCAPE-MeVO assessed EVT in patients with medium-vessel occlusions treated within 12 h of symptom onset, while DISTAL extended the treatment window to 24 h for occlusions in medium or distal vessels. Both trials showed that EVT did not improve 90-day outcomes compared to medical therapy alone. This contrasts with earlier retrospective studies, which reported similar recanalization and functional outcomes, along with lower rates of symptomatic intracranial hemorrhage (sICH), between late-window M2 and M1 occlusion cohorts.18,19 These discrepancies emphasize the uncertainty of MT outcomes for medium vessel occlusions in extended treatment windows. Furthermore, the temporal differences in hemorrhagic transformation (HT) risk between late and early windows for M2 occlusions remain uncharacterized.
In addition, patients with embolic strokes present with more severe neurological deficits compared to nonembolic strokes. 20 However, studies have showed that EVT achieves higher complete recanalization rates in embolic occlusions than in intracranial atherosclerosis-related occlusions, 21 with comparable22,23 or even better 24 functional outcomes. Moreover, in the management of acute embolic stroke, aspiration thrombectomy was associated with good functional outcomes compared to stent retriever thrombectomy. 25 Further research on embolic stroke is needed to improve patient’s outcomes.
Therefore, we aimed to investigate the effectiveness and safety outcomes of MT in a real-world cohort of acute stroke patients with primary embolic MCA M2 occlusions in late (>6 h) versus early (⩽6 h) treatment windows. Additionally, we evaluated the relationship between time to treatment and functional outcome in MCA-M2 occlusion patients treated within 24 h.
Methods
This study adheres to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for observational studies. Data were collected from the ARTISTA (A Registry for Thrombectomy in Stroke Therapy from Andalusia) registry. This multicenter registry prospectively and consecutively included stroke patients undergoing MT from 2017 in Seville-Huelva node, Spain. The registry study protocol and the consent forms were approved by the institutional review board of the University Hospital Virgen Macarena (ID 0609-N-22), which conformed to the recommendations of the Declaration of Helsinki. All patients or relatives signed informed consent forms.
Study population
In this retrospective analysis, we collected patients who met the following inclusion criteria from January 1, 2017 to June 30, 2024: (1) had a clinical diagnosis of AIS; (2) presented as primary M2 segment MCA occlusion confirmed by digital subtraction angiography (DSA), which was defined as de novo occlusions beyond the bifurcation of the M1 artery and extending to the apex of the circular sulcus, not resulting from large vessel occlusions due to clot migration or fragmentation, whether spontaneous or following IVT or EVT11,26; (3) treated with MT alone or combined with IVT, with an onset-to-puncture (OTP) time ⩽24 h; (4) had an embolic etiology, as evidenced by no residual severe stenosis in the culprit artery on postthrombectomy DSA, without the need for angioplasty or stenting.20,24 Onset time was measured as the time when the patient was last seen normal for wake-up strokes. We excluded patients who (1) were aged <18 years; (2) were lost to follow-up at 90 days after stroke onset; or (3) had missing covariate data.
Procedural and technical details
For patients presenting within the early treatment window, eligibility for MT was determined in accordance with contemporary clinical practice guidelines.13,14 Specifically, patients were required to be younger than 90 years, have a prestroke mRS score of 0–1, and demonstrate an Alberta Stroke Program Early Computed Tomography Score (ASPECTS) ⩾6 on noncontrast computed tomography (CT). Following the publication of low-ASPECTS trials, patients with a minimum ASPECTS of 3 were also considered eligible under selected conditions. 27 In addition, patients were required to have an National Institutes of Health Stroke Scale (NIHSS) score ⩾6, or an NIHSS score <6 in the presence of a clearly disabling neurological deficit, such as aphasia, hemianopsia, or functionally significant motor weakness. For patients presenting within the late treatment window, CT perfusion imaging was additionally required according to the unit’s predefined protocol. Eligibility in this time window was based on fulfillment of the perfusion mismatch criteria established in the DAWN trial. 28 MT was performed using second-generation devices, with aspiration preferentially adopted as the primary reperfusion strategy.
Data collection
Data were collected in the ARTISTA registry, which was maintained jointly by interventional neuroradiologists and vascular neurologists. We recorded the details of patient demographics, vascular risk factors, medical history, clinical features, medications prior to admission, and radiological characteristics, as previously described. 29 The NIHSS score was used to assess stroke severity. Stroke etiology was classified according to Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria. The ASPECTS was employed to detect the extent of early ischemic changes on the baseline noncontrasted CT scan. Angiographic collateral grade was evaluated using the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology Collateral Flow Grading System on baseline angiography. Pial collateral circulation was considered present when the score was >1 on pre-MT angiography. Data on acute reperfusion therapy, including door-to-treatment time interval, procedure duration, first-line thrombectomy technique, number of thrombectomy passes, anesthesia method, and thrombus type, were also collected. Follow-up head images were obtained 24 h after MT to assess the presence of HT and cerebral edema.
Study outcomes
The main clinical outcomes included (1) the 90-day ordinal modified Rankin Scale (mRS) score shift distribution; (2) 90-day good outcome, defined as mRS scores 0–2 or return to baseline mRS score in patients with prestroke mRS score >2; (3) futile recanalization (FR), defined as successful recanalization (modified Thrombolysis in Cerebral Infarction (mTICI) 2b-3) following MT but with an mRS >2 at 90 days. 30
The main adverse events included (1) sICH, defined as any intracranial hemorrhage detected on CT within 24 h of treatment, leading to an increase of ⩾4 points in the NIHSS score according to the European Cooperative Acute Stroke Study criteria; (2) subarachnoid hemorrhage (SAH) within 24 h of MT; (3) cerebral edema, identified as focal edema or edema with midline shift on follow-up imaging; (4) in-hospital mortality; and (5) 90-day mortality.
The main technical outcomes were (1) successful recanalization, defined as an mTICI 2b-3; (2) first-pass effect (FPE), defined as near-complete or complete revascularization (mTICI 2c/3) of the target occlusion and its downstream territory with a single device pass, without requiring rescue therapy 31 ; and (3) procedural complications, including vasospasm, vessel dissection or perforation, and new clots in a different vascular territory. 12
Statistical analysis
Categorical variables are expressed as counts with percentages, while continuous data are presented as medians accompanied by their interquartile ranges (IQRs) as appropriate. Patients were categorized into early (OTP time ⩽6 h) and late treatment windows (OTP time >6 and ⩽24 h). The Chi-square (χ2) test or Fisher’s exact test were used for discrete data, and Mann–Whitney U test for continuous data. For the ordinal mRS score shift, a multivariable ordinal logistic regression model was used to predict a 1-point shift toward the lower ordered value with the cumulative logit link function and ordinal distribution. Adjusted common odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Multivariable binary logistic regression models with a logit link function and binomial distribution specifications were used for good outcome and FR, and adjusted ORs with a 95% CI were also computed. The following covariates were included a priori in the multivariable models: age, hypertension, atrial fibrillation, wake-up stroke, baseline NIHSS, TOAST, ASPECTS, hyperdense MCA sign, IVT, and door-to-puncture time.
To further account for confounding, we used the propensity score-based inverse probability of treatment weighting (IPTW) method, which estimated the average treatment effect. Standardized mean differences (SMDs) were estimated in both the unweighted and IPTW-weighted populations to ensure a balance between the late and early MT for all potential confounders. The positivity assumption was assessed visually through overlap in kernel density and box plots for propensity scores in the late- and early-treated groups. The same set of variables used in the multivariable models was used to generate IPTW estimates. In addition, a marginal effect plot was used to illustrate the relationship between continuous OTP time and the predicted probability of a good outcome. All statistical analyses were performed using R (R Foundation for Statistical Computing, version 4.4). All p values were two-tailed tests with a statistical significance level of 0.05.
Results
Baseline patient characteristics
During the study period from January 1, 2017, to June 30, 2024, 2879 stroke patients who received MT were identified from the ARTISTA registry. Finally, 524 patients with primary embolic MCA M2 occlusions treated with MT were included (Figure 1). Of these patients, the median age was 76 years, 253 (48.3%) were women, the median presenting NIHSS was 12, and the median ASPECTS was 9. Among them, 317 patients (60.5%) underwent MT within the first 6 h after symptom onset, while 207 patients (39.5%) received the treatment in the late time window. Late MT-treated patients were younger (median (IQR), 75 (64–81) vs 76 (65–83) years; p = 0.001), had a lower median prestroke mRS score (0 (0–1) vs 0 (0–1); p = 0.033), exhibited a lower prevalence of hypertension (69.1% vs 79.2%; p = 0.009) and atrial fibrillation (45.9% vs 58.4%; p = 0.005), had lower median NIHSS (11 (7–16) vs 12 (8–18); p < 0.001) and ASPECTS (9 (8–10) vs 10 (8–10); p = 0.001) scores at presentation, and experienced more wake-up strokes (76.3% vs 9.1%; p < 0.001) compared to early-treated patients (Table 1). Additionally, patients in the late treatment window were less likely to receive IVT (9.2% vs 53.0%; p < 0.001), had lower rates of cardioembolic etiology (52.7% vs 65.0%; p = 0.005) and hyperdense MCA signs (46.9% vs 57.4%; p = 0.018), experienced longer door-to-puncture times (146 (100–220) vs 115 (75–161) min; p < 0.001), and were more likely to receive local anesthesia (90.3% vs 89.6%; p < 0.001).

Selection of the study cohort.
Characteristics of patients who underwent mechanical thrombectomy presenting with M2 occlusion, overall and in different onset-to-puncture time groups.

Data available for 521 of 524 patients.
505 of 524 patients.
476 of 524 patients.
Door-to-needle time was recorded only for patients who received intravenous thrombolysis.
Onset time was recorded as the time when the patient was last seen normal for wake-up strokes.
522 of 524 patients.
486 of 524 patients.
ASPECTS, Alberta Stroke Program Early Computed Tomography Score; IQR, interquartile range; MCA, middle cerebral artery; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; TOAST, Trial of Org 10172 in Acute Stroke Treatment.
Clinical outcomes
At 90 days after stroke onset, 62.2% (326/524) of patients had good outcome. Of the 501 patients with successful recanalization following MT, 34.5% (173/501) failed to achieve 90-day good outcomes, showing FR (Table 2). The distribution of mRS scores at 90 days between the late- and early-treated groups is shown in Figure 2. Patients treated in the late window had similar 90-day mRS scores (2 (IQR, 1–4) vs 2 (IQR, 1–3); p = 0.394) compared to those treated in the early window. Late treatment was tended to be associated with slightly lower good outcomes (58.9% vs 64.4%; OR 0.80, 95% CI 0.56–1.14; p = 0.211) and higher FR rates (37.8% vs 32.5%; OR 1.26, 95% CI 0.87–1.84; p = 0.224).
Main clinical outcomes, adverse events, and technical outcomes of patients with M2 occlusions after mechanical thrombectomy, overall and in different onset-to-puncture time groups.

Analysis of 501 patients with successful recanalization.
CI, confidence interval; DSA, digital subtraction angiography; IQR, interquartile range; mRS, modified Rankin Scale; NA, not available; OR, odds ratio.

Distribution of 90-day mRS scores between late and early treatment windows.
Multivariable logistic regression and IPTW analysis
The late and early treatment groups were well matched after IPTW, with SMDs ⩽10% for most covariates, except for atrial fibrillation, TOAST classification, IVT, and door-to-puncture time (Supplemental Table 1). After adjusting for age, hypertension, atrial fibrillation, wake-up stroke, baseline NIHSS, TOAST, ASPECTS, hyperdense MCA sign, IVT, and door-to-puncture time, the absence of difference between late- and early-treated groups persisted in the multivariable logistic regression analysis of 90-day ordinal mRS score shift (adjusted common OR 0.98, 95% CI 0.58–1.66; p = 0.941). A similar result was observed in the IPTW analysis (adjusted common OR 0.52, 95% CI 0.19–1.43; p = 0.203; Table 3). Also, no significant differences were found in the multivariable adjusted analyses for good outcome (adjusted OR (aOR) 0.74, 95% CI 0.38–1.44; p = 0.377) or FR (aOR 1.30, 95% CI 0.67–2.55; p = 0.432). The IPTW analysis corroborated the adjusted analyses (good outcome (aOR 0.82, 95% CI 0.39–1.73; p = 0.600) or FR (aOR 1.19, 95% CI 0.56–2.50; p = 0.653)). Moreover, longer OTP times were not significantly associated with a lower probability of a good 90-day outcome (OR 0.94, 95% CI 0.78–1.13; p = 0.498; Supplemental Figure 1).
Multivariable logistic regression and IPTW evaluation of clinical outcomes at 90 days in late versus early treatment time windows.
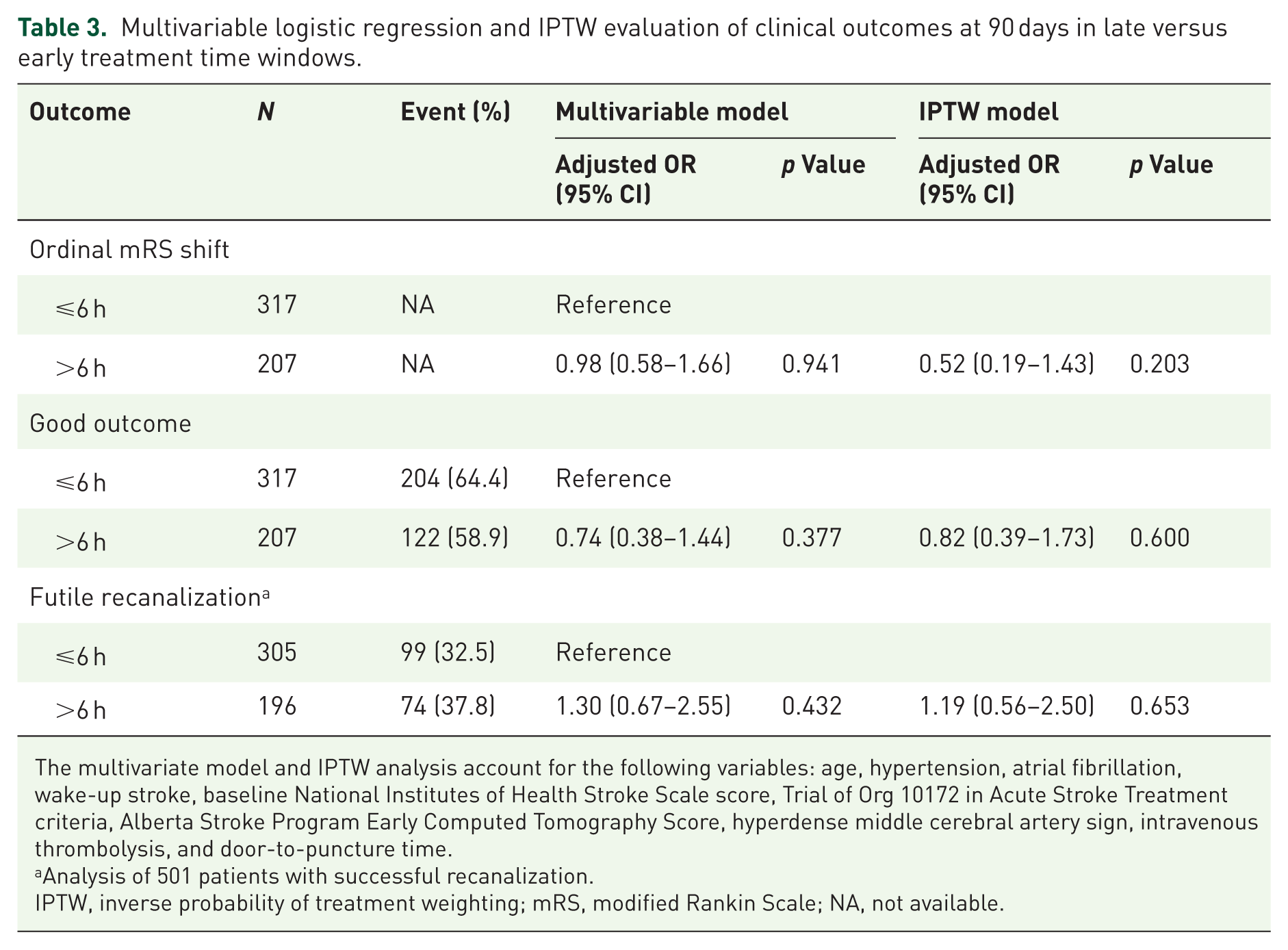
The multivariate model and IPTW analysis account for the following variables: age, hypertension, atrial fibrillation, wake-up stroke, baseline National Institutes of Health Stroke Scale score, Trial of Org 10172 in Acute Stroke Treatment criteria, Alberta Stroke Program Early Computed Tomography Score, hyperdense middle cerebral artery sign, intravenous thrombolysis, and door-to-puncture time.
Analysis of 501 patients with successful recanalization.
IPTW, inverse probability of treatment weighting; mRS, modified Rankin Scale; NA, not available.
Adverse events
Compared to the early-treatment group, patients treated in the late window showed numerically higher rates of sICH (3.4% vs 3.2%; OR 1.08, 95% CI 0.40–2.87; p = 0.886) and SAH (5.3% vs 4.4%; OR 1.22, 95% CI 0.54–2.73; p = 0.637), alongside slightly lower rates of in-hospital mortality (5.3% vs 7.6%; OR 0.69, 95% CI 0.33–1.43; p = 0.312), and 90-day mortality (10.6% vs 11.4%; OR 0.93, 95% CI 0.53–1.63; p = 0.795; Table 2). The proportion of cerebral edema was low and comparable between groups (0.5% vs 0.6%; OR 0.77, 95% CI 0.07–8.49; p = 1.000).
Technical outcomes
Rates of successful recanalization were nearly identical between the late- and early-treatment groups (95.7% vs 95.6%; OR 1.02, 95% CI 0.43–2.39; p = 0.970), as were rates of FPE (61.8% vs 61.2%; OR 1.03, 95% CI 0.72–1.47; p = 0.884; Table 2). Procedural complications were infrequent and did not differ significantly between groups (all p > 0.539), with new thrombus formation in a different vascular territory being the most common (1.4% vs 2.5%), followed by vasospasm (0.5% vs 0.6%) and vessel dissection or perforation (0.5% vs 0.3%).
Discussion
In this multicenter cohort of patients with acute primary embolic MCA M2 occlusions, late-window MT was performed in approximately 40% of cases. Clinical outcomes in the late-treatment group were comparable to those in the early-treatment group, with no significant differences in the ordinal mRS score shift, rates of good outcome, or FR at 90 days. Safety outcomes, including sICH, 90-day mortality, successful recanalization, and procedural complications, were also similar between groups. These findings suggest that MT for M2 occlusions may be similarly effective and safe in the late treatment window, though interpretation should consider patient selection and baseline heterogeneity.
Currently, the impact of MT in patients with M2 occlusions, particularly in the late treatment window, remains a major point of debate. 14 While several randomized trials are ongoing to evaluate the efficacy of thrombectomy for M2 and more distal occlusions in the extended time window, our study offers real-world evidence from a large, multicenter registry that helps inform clinical practice in the absence of definitive trial data. In the late treatment window, the good outcome rate for M2 occlusions in our study was 58.9%, closely matching the 59.6% reported by the SOLSTICE consortium in a comparative analysis of late-window EVT outcomes between M2 and M1 occlusions. 19 However, this rate seems higher than the 46.7% observed in patients with M2 occlusions who underwent MT in the delayed window in the STAR registry. 18 This difference may be attributable to the shorter OTP time (475 (410–579) vs 754.3 ± 497.4 min) and the higher use of direct aspiration technique (84.1% vs 57.2%) observed in our cohort. Our slightly higher rate of successful recanalization (95.7% vs 90.5%) may also contribute to this difference. Moreover, we found that the rates of good outcomes were similar between the late and early treatment window cohorts (58.9% vs 64.4%), consistent with findings from previous meta-analyses on early-window thrombectomy for M2 occlusions (58.2% and 59.0%).9,32 Additionally, we reported FR rates of 37.8% in the late treatment group and 32.5% in the early treatment group, both notably lower than the 51.4% reported in the German Stroke Registry. 33 That study included M2 occlusions and had a shorter median time from symptom onset or last seen well to admission (2.5 h, IQR: 1.2–5.9 h). One possible explanation for this discrepancy is that our study excluded patients with nonembolic M2 occlusions. Previous studies have shown that nonembolic strokes are associated with lower reperfusion rates when treated with thrombectomy alone and are more likely to experience poor functional outcomes.24,33,34 Alternatively, the lower rates of procedural complications during our treatment (0.4%–2.1% vs 2.4%–5.9%) may also explain the difference.
Adverse event rates were comparable between the two treatment groups. The sICH rate in the late treatment cohort (3.4%) was consistent with those reported in prior studies of late-window thrombectomy for M2 occlusions, including the STAR registry (2.2%) and SOLSTICE consortium (4.3%). Moreover, this rate was either similar to or slightly lower than those observed in early-window M2 occlusion patients from the STRATIS (4.0%) and MR CLEAN (6.6%) registries.11,12 This difference may be attributed to the preferential use of direct aspiration as the initial treatment strategy in our study. As noted in the STRATIS and MR CLEAN registries, the use of stent-retriever in the distal branches may increase rate of sICH and SAH.11,12 Additionally, the 90-day mortality rate in patients with M2 occlusions treated in the late window in our study (10.6%) was similar to that found in the STAR registry (13.9%) and the SOLSTICE consortium (11.2%).
In this study, the successful recanalization rate in the late-window group was 95.7%, higher than those described in the STAR registry (90.5%) and SOLSTICE consortium (82.9%). This rate was nearly identical to that observed in our early-window cohort (95.6%) and notably above the 60%–90% range previously documented for early-window thrombectomy.9,11,12,32,35 Endovascular thrombectomy for M2 occlusions remains technically challenging due to the smaller vessel size, tortuous course, and distal location. However, continued improvements in device technology36,37 and growing operator experience 38 may partly explain the high rate of successful recanalization observed in our study. Moreover, the frequency of procedural complications was similar in our late and early MT patients with M2 occlusions (0.5%–1.4% vs 0.3%–2.5%). Current data on procedural complications in late thrombectomy are scarce and primarily focus on patients with anterior circulation large vessel occlusions, with reported rates ranging from 2.2% to 5.6%.28,39 Additionally, one study found no difference in procedure complication rates between early and late EVT in AISs (12.8% vs 11.4%). 40
Our results differ from recent studies evaluating EVT for distal or medium vessel occlusion strokes, which have generally reported no functional or survival benefit of thrombectomy over medical therapy and an increased risk of hemorrhagic complications.41,42 Similarly, evidence in patients with minor M2 occlusion has supported an initial conservative strategy rather than immediate intervention.43–45 In contrast, in our cohort of primary embolic M2 occlusions, we observed comparable effectiveness and safety outcomes between early- and late-window treatment groups. This discrepancy is likely due to differences in study populations: our analysis excluded more distal vessels and included patients with higher baseline neurological severity. Additionally, selection criteria and the observational design may contribute to differences from prior studies. These findings underscore the need for future studies to better define patient subgroups most likely to benefit from thrombectomy, particularly in the late time window.
This study has several limitations. First, the observational nature of this study introduces inherent selection bias and limits causal inference, which may affect generalizability. Although multivariable adjustment and IPTW were applied to balance baseline characteristics, residual imbalances between treatment groups remained. In addition, unmeasured imaging-related factors, such as infarct core volume and collateral status, may have influenced the observed outcomes. Second, as a multicenter study, the lack of clustering analysis may have impacted our results to some extent, considering the variability in operational techniques and thrombectomy devices used across centers. Third, the primary inclusion criterion was the presence of primary embolic M2 occlusions; however, the definition of M2 was not standardized by vessel anatomy or diameter and included multiple subtypes, including proximal, distal, dominant, and nondominant segments. Future studies with more detailed subclassification would be preferable to better account for potential outcome differences. Finally, although the overall cohort size was relatively large, the number of infrequent but clinically important safety events, such as sICH and procedural complications, was relatively low. This limits the statistical power to detect potentially meaningful differences in complication rates between early- and late-window treatment groups. Thereby, these findings should be interpreted cautiously, and larger studies or pooled analyses are warranted to more precisely assess the safety profile of MT across different time windows.
Conclusion
In this European cohort of patients with acute primary embolic M2 occlusions, MT demonstrated comparable effectiveness and safety outcomes between early and late treatment windows. These results should be interpreted in the context of patient selection, M2 heterogeneity, and limited numbers of rare safety events, and they highlight the need for future studies to define subgroups most likely to benefit from reperfusion strategies.
Supplemental Material
sj-docx-1-tan-10.1177_17562864261434562 – Supplemental material for Outcomes of mechanical thrombectomy in acute stroke due to primary embolic middle cerebral artery M2 occlusions: a comparison of late versus early windows
Supplemental material, sj-docx-1-tan-10.1177_17562864261434562 for Outcomes of mechanical thrombectomy in acute stroke due to primary embolic middle cerebral artery M2 occlusions: a comparison of late versus early windows by Huan Wang, Deren Wang, Elena Zapata-Arriaza, Marta Aguilar-Pérez, Asier de Albóniga-Chindurza, Henry Antonio Andrade Ruiz, Joan Montaner and Alejandro González García in Therapeutic Advances in Neurological Disorders
Supplemental Material
sj-docx-2-tan-10.1177_17562864261434562 – Supplemental material for Outcomes of mechanical thrombectomy in acute stroke due to primary embolic middle cerebral artery M2 occlusions: a comparison of late versus early windows
Supplemental material, sj-docx-2-tan-10.1177_17562864261434562 for Outcomes of mechanical thrombectomy in acute stroke due to primary embolic middle cerebral artery M2 occlusions: a comparison of late versus early windows by Huan Wang, Deren Wang, Elena Zapata-Arriaza, Marta Aguilar-Pérez, Asier de Albóniga-Chindurza, Henry Antonio Andrade Ruiz, Joan Montaner and Alejandro González García in Therapeutic Advances in Neurological Disorders