
Abstract
Background:
Magnetic resonance-guided focused ultrasound (MRgFUS) thalamotomy has shown promising results in treating pharmaco-resistant essential tremor (ET). This incisionless, image-guided technique targets the ventralis intermedius nucleus of the thalamus with precision, sparing surrounding eloquent tissue.
Objective: This study aims to assess the efficacy of MRgFUS thalamotomy in improving tremor among ET patients, as objectively measured by a tri-axis accelerometer, and to compare these objective measures with the conventional Clinical Rating Scale for Tremor (CRST).
Design: Prospective observational study.
Methods:
Ten ET patients (aged 68.1 ± 11.8 years) received the MRgFUS treatment. Improvements in tremor severity were assessed using primary (CRST), with additional measurements of kinematic feature obtained from a tri-axis accelerometer. Correlations between accelerometer-derived kinematic features and CRST scores were evaluated.
Results:
Significant improvement in tremor severity was observed in the cohort, as measured by both the accelerometer and CRST (paired Student’s t test, p < 0.05) before and 1 day after the treatment. A moderate-to-strong correlation was found between accelerometer measurements and CRST scores.
Conclusion:
The tri-axis accelerometer provides an effective means of monitoring tremor reduction following MRgFUS and correlated well to the clinical scales like CRST. This study supports the feasibility of accelerometer-based monitoring in clinical practice for MRgFUS assessment.
Keywords
Introduction
Essential tremor (ET), primarily characterized by a rhythmic oscillation of agonist and antagonist muscle groups, is one of the most common neurological disorders.1,2 ET generally involves head, vocal cords, and upper limbs, with a variable frequency of 4–12 Hz.3,4 ET affects people of all ages and has a bimodal distribution of age at onset, respectively, peaking at the second and sixth decades.5,6 It is a considered as a benign tremor; however, it is progressing over life and becomes severely disabling for the majority of the patients. 7
Other types of tremor may also be present in the same patient, including postural tremor of arms, and intentional tremor (below 5 Hz) and rarely resting tremor of the arms. 5 ET tremor or postural/kinetic tremor is associated with abnormal oscillatory activity within the cerebello-thalamo-cortical circuit. 5 Of note, at least 30% of ET patients do not respond to established medications, while a further 30% of ET patients stop taking their medication due to side effects. 8
In the last decade, a new advance treatment for pharmaco-resistant ET has been developed: the magnetic resonance-guided focused ultrasound (MRgFUS) thalamotomy. The treatment is a incisionless technique used to ablate the ventralis intermedius (VIM) nucleus of the thalamus by focus ultrasound under MRI guide, which offers significant precision with preservation of surrounding eloquent tissue.9,10
The measurement of tremor severity is commonly based on clinical rating scales, such as the Clinical Rating Scale for Tremor (CRST), which is a standardized assessment tool used in research and clinical settings to evaluate the severity of tremors and their impact on functional abilities. 11 The CRST consists of three sections, each with distinct objectives and subcategories. Part A is designed to assess the severity of different types of tremor that might coexist in the same patient. Part B evaluates the impact of tremors on specific motor tasks. Part C focuses on disability caused by the tremor (Supplemental Material 1). The inclusion of detailed sub-scores for each part allows for a more granular analysis of tremor characteristics, enabling clinicians to identify specific patterns of impairment and tailor treatment strategies accordingly.
Notably, there are several disadvantages in using this clinical scale. First, it is subjective as it relies on assessors’ judgment; therefore, it introduces variability in evaluations and potential discrepancies in scores between different assessors. Second, the CRST may lack sensitivity, potentially failing to detect subtle changes in tremor severity or functional impairment. This drawback becomes particularly challenging when evaluating outcome posttreatments that might lead to modest improvements.
In recent years, many research groups developed novel sensor technologies to perform clinical assessment of tremor. 11 Particularly, inertial measurement units could provide noninvasive quantified measurement of the kinematics for objective evaluation and analysis in medical practice. 12 The main measurements focus on extracting time-domain and frequency-domain matrices for both action and static tremors, including power spectrum, peak frequency, and the correspond amplitude. 13 These kinematic features are widely applied to the assessment of the rest and postural tremor’s severity, disease progression, and effect of the treatment.14,15
This study aimed to objectively demonstrate the effectiveness of MRgFUS thalamotomy in reducing tremor severity in ET patients using a tri-axis accelerometer. By leveraging the accelerometer’s capacity for precise, quantifiable kinematic measurements, we aimed to provide an alternative to traditional subjective clinical rating scales, such as the CRST.
Materials and methods
This is a single-center, prospective observational analysis of a series of patients suffering from pharmaco-refractory ET who received MRgFUS as part of the standard of care between August 27, 2018, and March 1, 2022. Ten patients were enrolled in this study (Table 1). A diagnosis of ET was confirmed from clinical history and examination by a neurologist specialized in movement disorders. Patients were eligible if they had a moderate-to-severe postural or intention tremor in the hand, indicated by a score of ⩾2 on the CRST and if the tremor was disabling, defined by a score of ⩾2 on any of the eight items in the disability subsection of the CRST. An inadequate medication response was defined as a therapeutic dose of each medication, poor response to drugs, or the development of side effects as the medication dose was titrated. All participants were right-handed with severe symptoms on the right side.
Demographic data of the treated ET patients.
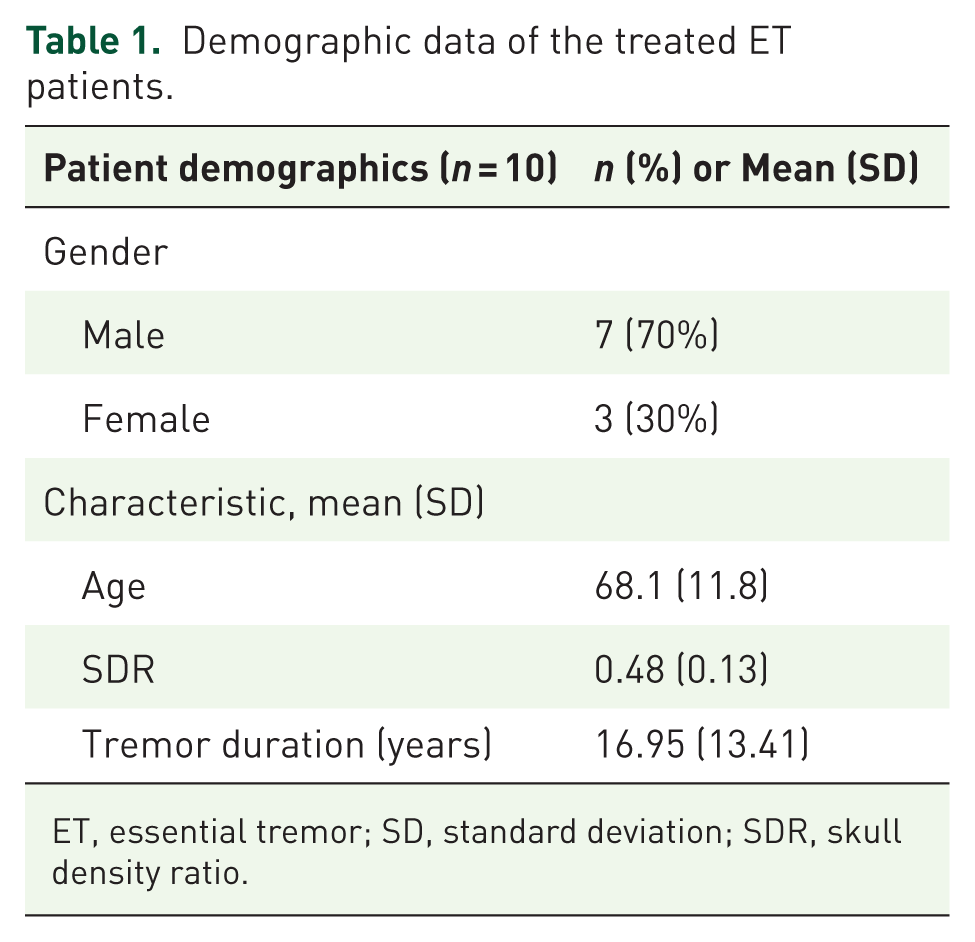
ET, essential tremor; SD, standard deviation; SDR, skull density ratio.
Procedure
All participants performed a 3T MRI scan for target planning 1 day before the MRgFUS therapy. High-quality axial and sagittal T2-weighted images were acquired to identify the location and distance of anterior commissure (AC)-posterior commissure (PC). A 3D fast-spin-echo-based double inversion recovery white matter null image was fused to the above T2W image to visually locate the avoiding regions, including the VIM and internal capsule. All treatment were performed in a 1.5T MR imaging system (GE Optima 450w GEM; GE Healthcare, Milwaukee, WI, USA) using the ExAblate Neuro device (InSightec, Haifa, Israel). VIM contralateral to the most affected limb were planned to acquire the coordinates based on the individual AC-PC line. Standard treatment methods were done according to the previously published protocol.9,10 VIM with 1/4 AC-PC anterior to PC point was selected, 11 mm lateral to the third ventricle wall and 2 mm above the AC-PC line and adjusted accordingly.
Clinical data collection
The primary outcome of the study was the measurement of the tremor severity pre- and postsurgery with the CRST scores. Part A, which assesses action and postural tremor, includes subscores evaluated separately for the treatment side and opposite side. Part B measures tremor severity during functional tasks reflecting its impact on daily activities on both the treatment and opposite sides. Part C evaluates functional disability associated with tremor focusing on several activities. Each subscore was analyzed independently to provide a comprehensive assessment of tremor severity and treatment outcomes (Figure 1).

Schematic overview of the CRST, comprising Part A (tremor localization/severity), Part B (specific motor tasks), and Part C (functional disability). Each part is scored from 0 to 4, with the total CRST score ranging from 0 to 144, where higher scores indicate more severe tremor.
Secondary outcomes were the measurement of nonmotor symptoms present in patients with ET through the use of specific clinical scales such as the Mini-Mental Status Examination (MMSE) for cognitive function, Beck’s Depression Inventory (BDI-II) for depression assessment, and the Tinetti Performance Oriented Mobility Assessment (POMA) for balance and mobility evaluation. Side effects were also systematically recorded. The primary and secondary ET test batteries were conducted at baseline (T0) and 1 day after the procedure (T1). Additionally, brain MRI scans were obtained at baseline and post-MRgFUS to evaluate treatment effects.
Accelerometer
The accelerometer data were recorded by ANT QFN packaged multichip MPU-9250 (InvenSense, San Jose, CA, USA), which integrates a three-axis accelerometer, three-axis gyroscope, and three-axis magnetometer AK8963 (AKM Semiconductor, San Jose, CA, USA) via embedded microcontroller (MSP430). The monitored digital signals were transmitted via Bluetooth protocol (BR-LE4.0-D2). The capacitance on each axis of the accelerometer measures the degree of deviation of the axes, respectively; the host computer of the data acquisition system was used to set the acquisition frequency, calibrate the sensors, visualize the acquisition signal, and store the data. The patients performed 4 postures while seated on the chair and while the accelerometers on the first proximal interphalangeal (PIP) joint of the index finger recorded the tremor data. The assessed postures were raising the hand (P1), raising the hand with wrist extension (P2), wing position (P3), and holding a pen (P4) (Figure 2). Each posture was recorded for 10 s.

Illustrations of the assessed four postures during the tremor recordings. (a) Raising the hand (P1); (b) raising the hand with wrist extension (P2); (c) wing position (P3); (d) holding a pen (P4).
Two signal-preprocessing processes were employed to the raw signals before feature extraction.
16
First, a third-order band-pass Butterworth filter with a cut-off frequency of 5–12 Hz was applied to remove artifacts and noise,
17
including subtle physiological tremor caused by normal muscle activation and random noises. Then, the signal vector magnitude (SVM) of the filtered tri-axial accelerations was calculated. SVM is a simple and effective approach to reduce computational complexity for signal processing, which decreases dependence on sensor placement and the effects of posture variability. The SVM of tri-axial accelerations was calculated as
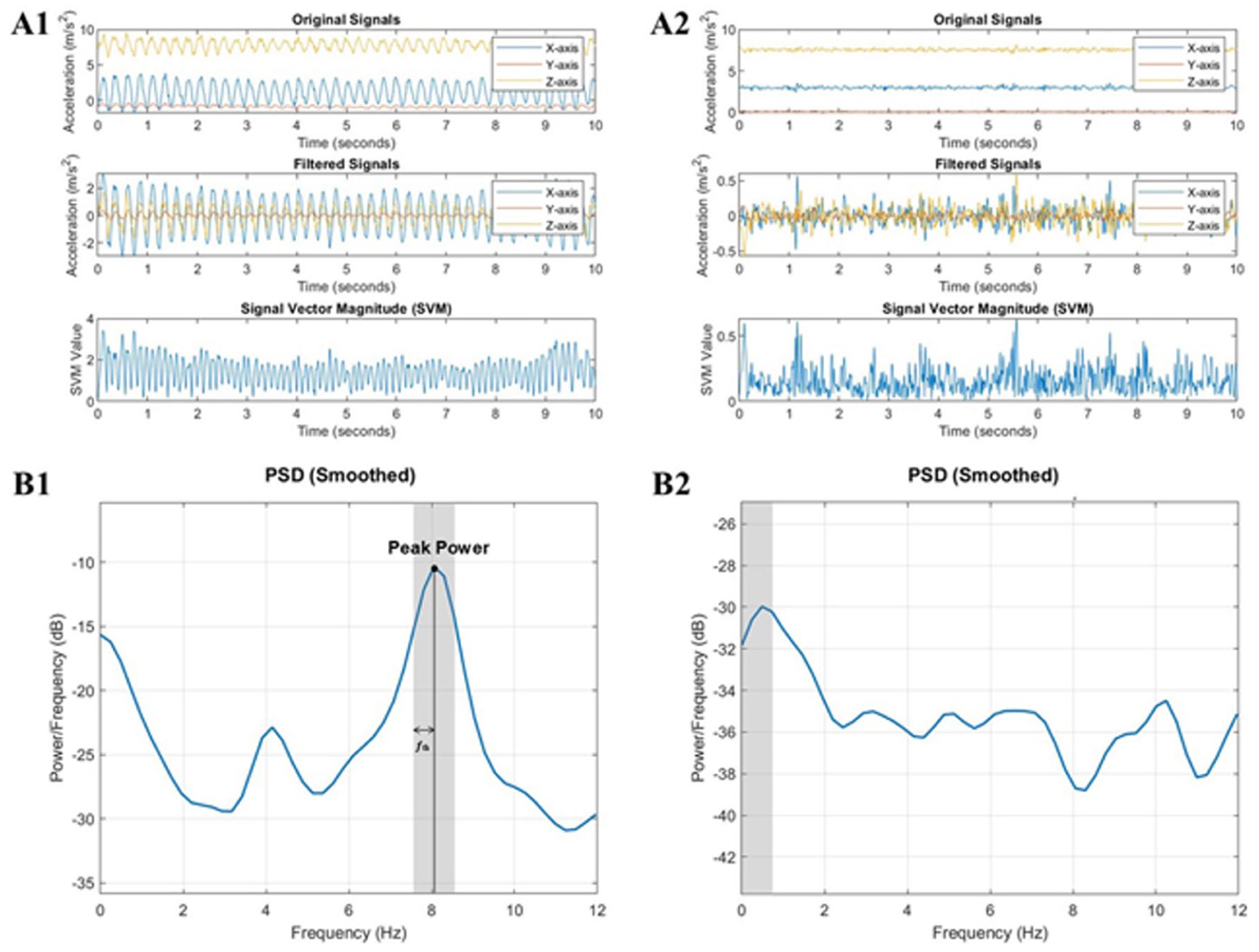
Example data from one subject in a specific posture, comparing pretreatment (a1, b1) and posttreatment (a2, b2) results, with (a1) and (a2) displaying raw acceleration (top), filtered acceleration (middle), and SVM (bottom), and (b1) and (b2) presenting PSD via Welch’s method in the frequency domain.
After signal preprocessing, various kinematic parameters were characterized from the preprocessed series of different tests. The kinematic features were extracted from SVM of the accelerometer for performance analysis. Two feature categories, including time-domain and frequency-domain features, were employed in this work. The usability of these parameters was validated in previous work.17,18 The applied time-domain features are summarized in Supplemental Material 2.
Several critical morphological features were applied to obtain the diverse characters of movement patterns, including shape factor, crest factor, impulse factor, and margin factor. These parameters reflected signal features in the performance of spike, normalized peak, energy, power, and change in time.
In addition to time-domain features, frequency-domain metrics were also calculated to display the characteristics of movement smoothness and stability. Several studies showed that spectral features have the potential to indicate more intuitive characteristics compared to time-domain features in movement analysis. The applied frequency-domain features were introduced as follows (Figure 3(b1, b2)):
Tremor peak power in power spectral density (PSD) was defined as the area under the PSD curve within the main frequency interval providing information about the power of tremor frequencies in the signal.
Peak power ratio was the ratio of the peak power to the total power in the PSD helping to classify whether the signal was exhibiting tremor characteristics.
Principal peak in PSD represents the main frequency component with the maximum signal power in the PSD reflecting the dominant frequency in the signal and providing insights into the frequency distribution of the signal’s power.
While data were collected for all 10 participants across most postures, data loss occurred for posture P4 due to technical issues, including sensor misalignment and interruptions in data transmission. As a result, analyses for P4 were based on data from seven participants.
Statistical analysis
Given the small sample size, statistical analysis of quantitative scores compared with baseline was performed using a paired Student’s t test for normally distributed data. Data are presented as mean ± SD in the text, and a p-value of less than 0.05 was considered statistically significant. For correlation analysis between the CRST subscores (particularly Upper Extremity Posture (UEP)) and accelerometer-derived parameters, Spearman’s rank correlation was employed to account for potential non-linear relationships. Correlation coefficients (r) and corresponding p-values are reported to highlight the strength and significance of these associations.
Results
We reported 10 patients (aged 68.1 ± 11.8 years, 3 woman) with pharmaco-refractory ET (Table 1). No difficulty was experienced by the patients in completing the tasks. The skull density ratio was 0.48 ± 0.13 (range: 0.25–0.72). Maximum sonication power applied to reach final temperatures was 890.40 ± 193.40 watts (W) (range: 486–1156); the actual energy were 18546.1 ± 7713.0 joules (J; range: 9542–36,072) for the procedure.
Primary outcome measures
Our analysis focused on the UEP sub-score of the CRST and four accelerometer posture data: P1, P2, P3, and P4 (Figure 1), with other CRST scores, including Total Score, Part A Treatment Side, Part B Treatment Side, and Part C. Significant improvement was observed in the UEP subscore following MRgFUS treatment, with the mean UEP score reducing from 2.30 ± 0.46 at baseline to 0.50 ± 0.50 1 day posttreatment (t(9) = 7.61, p < 0.01), indicating a substantial reduction in postural tremor severity (Table 2). In addition to the UEP score, significant reductions were also observed in the total CRST score (t(9) = 8.72, p < 0.01), Part A Treatment Side (t(9) = 8.68, p < 0.01), Part B Treatment Side (t(9) = 7.47, p < 0.01), and Part C (t(9) = 7.64, p < 0.01), further confirming the effectiveness of MRgFUS in alleviating tremor symptoms immediately after the treatment.
Clinical outcomes of the treated patients before and after 1-day of the MRgFUS.

BDI-II, Beck’s Depression Inventory; CRST, Clinical Rating Scale for Tremor; MMSE, Mini-Mental Status Examination; MRgFUS, magnetic resonance-guided focused ultrasound; POMA, Performance Oriented Mobility Assessment; UEP, Upper Extremity Posture. **p < 0.01.
Accelerometer-derived features also demonstrated significant changes in different parameters. For Posture P1, significant differences were observed across multiple parameters. The maximum peak value decreased from a baseline (T0) of 1.88 ± 1.39 to a posttreatment (T1) value of 0.54 ± 0.26, t(9) = 3.01, p = 0.02. Similarly, the minimum valley value improved from −0.74 ± 0.63 at T0 to -0.21 ± 0.06 at T1, t(9) = −2.80, p = 0.03. The root mean square (RMS) also showed a significant reduction from 0.38 ± 0.33 at T0 to 0.10 ± 0.03 at T1, t(9) = 2.80, p = 0.02. The peak-to-peak amplitude followed the same trend as the maximum peak value, decreasing from 1.88 ± 1.39 at T0 to 0.54 ± 0.26 at T1, t(9) = 3.01, p = 0.02. Additionally, the margin factor showed a substantial increase, rising from 25.25 ± 20.45 at T0 to 50.33 ± 11.43 at T1, t(9) = −4.09, p < 0.01.
For Posture P2, significant changes were also noted. The minimum valley value improved from −1.01 ± 0.86 at T0 to −0.44 ± 0.19 at T1, t(9) = −2.62, p = 0.03. The average value decreased from 0.05 ± 0.04 at T0 to 0.02 ± 0.02 at T1, t(9) = 3.20, p = 0.01. The RMS showed a marked reduction, declining from 0.49 ± 0.37 at T0 to 0.23 ± 0.13 at T1, t(9) = 3.20, p = 0.01. The margin factor exhibited a significant increase, rising from 17.14 ± 11.39 at T0 to 36.87 ± 16.56 at T1, t(9) = −5.70, p < 0.001. Lastly, the peak power ratio decreased from 0.23 ± 0.09 at T0 to 0.13 ± 0.05 at T1, t(9) = 3.66, p < 0.01.
For posture P3, the peak power ratio showed significant change: T0 0.38 ± 0.20 versus T1 0.21 ± 0.07, t(9) = 2.69, p = 0.03.
For posture P4, significant differences were observed in margin factor (T0: 9.99 ± 28.74 vs T1: 56.56 ± 28.74, t(7) = −4.88, p < 0.01). However, data for P4 were available for only seven participants due to technical issues encountered during the recording process.
These findings indicate that various accelerometer-derived features were significantly different after the treatment, highlighting their potential for tracking tremor severity and treatment effects (Table 3).
The statistics of accelerometer parameters before and after MRgFUS in time domain and frequency domain before and after 1-day of the MRgFUS.
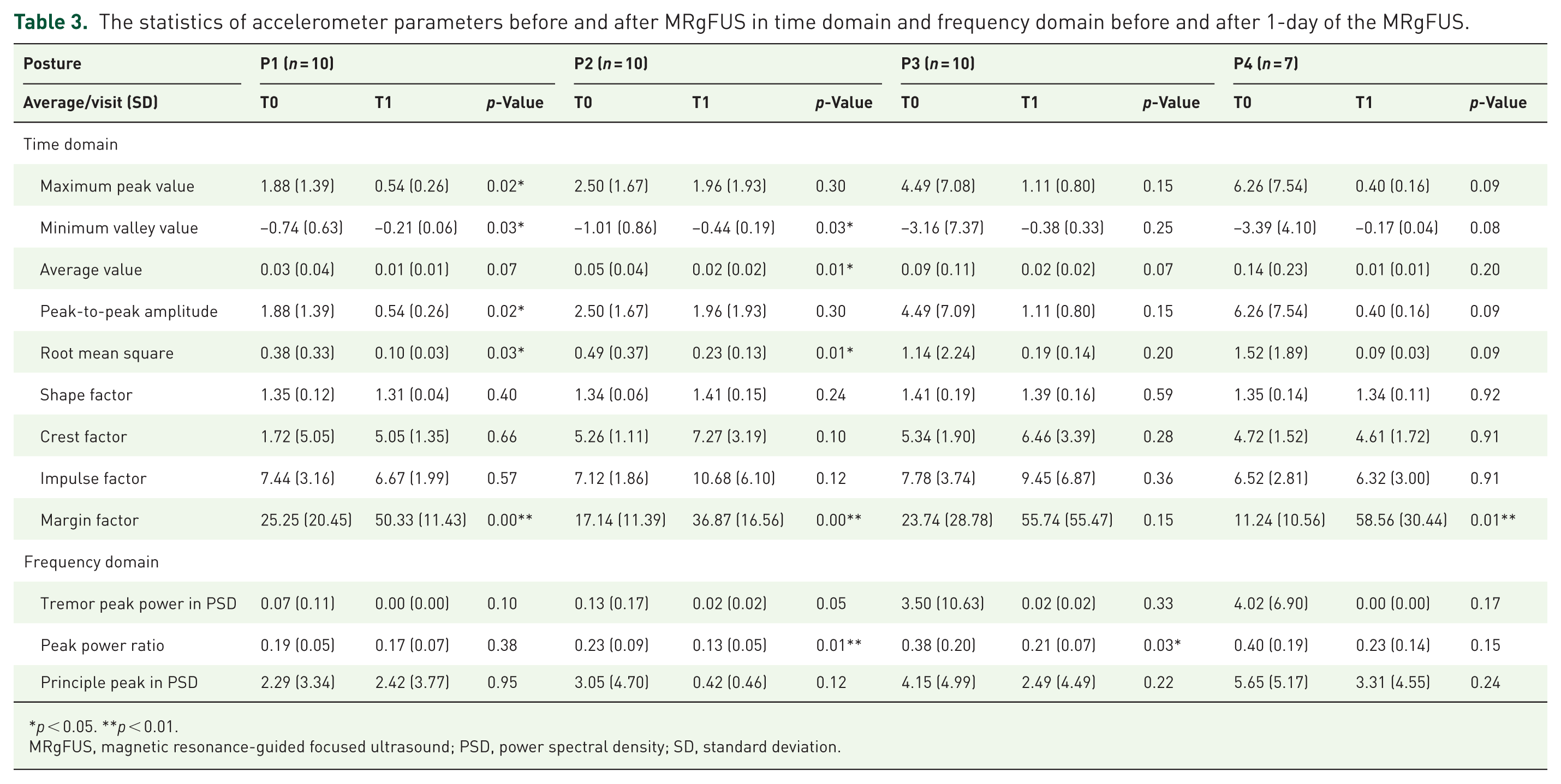
p < 0.05. **p < 0.01.
MRgFUS, magnetic resonance-guided focused ultrasound; PSD, power spectral density; SD, standard deviation.
Secondary outcome measures
No significant differences were noted in MMSE, POMA, and BDI-II 1 day after the treatment (Table 2). The side effect were procedure-related symptoms such as headache, pain, and dizziness during treatment but no severe adverse effects were noted.
Correlations
We observed significant correlations between UEP sub-scores and various accelerometer-derived features, confirming the sensitivity of these metrics to tremor changes. All analyzed features exhibited significant differences before and after the intervention, and strong correlations with UEP were noted using Spearman’s correlation analysis (Table 4). Key findings include:
The Spearman correlation (r) and corresponding p-values between UEP subscores and accelerometer-derived tremor features, all of which showed statistically significant associations (p < 0.05).
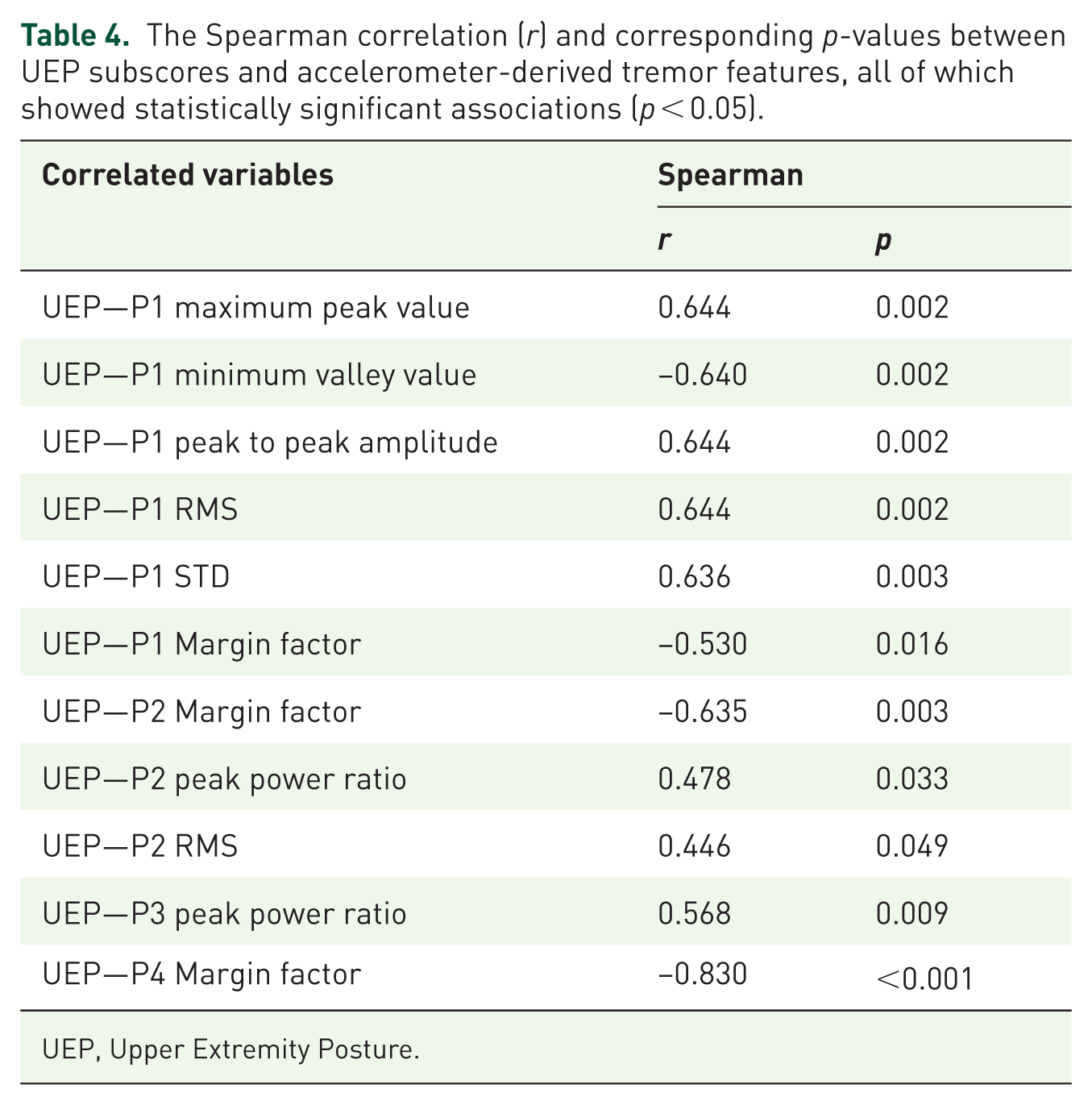
UEP, Upper Extremity Posture.
Posture P1: Significant positive correlations were observed for maximum peak value (r = 0.644, p = 0.002), peak-to-peak amplitude (r = 0.644, p = 0.002), and RMS (r = 0.644, p = 0.002). Minimum valley value showed a negative correlation (r = −0.64, p = 0.002).
Posture P2: Significant positive correlations were observed for RMS (r = 0.644, p = 0.002) and peak power ratio (r = 0.478, p = 0.033). Margin factor exhibited a significant negative correlation (r = −0.635, p = 0.003).
Posture P3: Peak power ratio was positively correlated with UEP (r = 0.568, p = 0.009).
Posture P4: Margin factor demonstrated the strongest negative correlation (r = −0.83, p < 0.001).
These findings suggest that accelerometer-derived features, particularly those related to postures P1 and P4, are closely aligned with UEP scores, providing objective support for the clinical improvements observed. Figure 4 illustrates these correlations through scatter plots with trend lines, highlighting the Spearman correlation coefficients (r) and corresponding p-values.

The Spearman correlations between UEP (CRST) scores and selected features (P1 to P4). Each subplot includes a trend line, Spearman r, and p-value, highlighting significant relationships (p < 0.05) between tremor severity and specific features.
Discussion
This study demonstrates the efficacy of MRgFUS thalamotomy in treating ET through objective tremor quantification using accelerometer-derived features. Significant reductions in tremor severity were observed in CRST scores, particularly in the UEP subscore, which decreased notably from baseline to 1-day posttreatment. These improvements were further supported by accelerometer analysis, which provided quantifiable evidence of reduced tremor severity and enhanced postural stability.
The analysis of time-domain features revealed substantial reductions in tremor severity, particularly in postures P1 and P2. Maximum peak value, minimum valley value, RMS, and peak-to-peak amplitude all showed significant posttreatment decreases, with p-values ranging from 0.02 to 0.03, indicating a reduction in overall tremor amplitude. RMS, a measure of signal energy, 19 significantly decreased posttreatment, further confirming a decline in tremor intensity and improved postural stability.
One of the most notable findings was the significant increase in the margin factor across multiple postures after MRgFUS thalamotomy.
Posture P1 (p < 0.01), P2 (p < 0.01), and P4 (p = 0.01) all showed highly significant increases. Margin factor, which measures peak amplitude relative to the RMS value, exhibited the largest changes among accelerometer-derived features. A higher margin factor typically reflects less rhythmic and more intermittent movement, suggesting that posttreatment tremor episodes became less predictable and less continuous.12,20 From a clinical perspective, this increase in margin factor is particularly relevant because postural tremor is one of the most functionally disabling aspects of ET, affecting activities such as eating, writing, and holding objects. The data suggest that MRgFUS not only reduces tremor amplitude but also disrupts the rhythmic nature of tremor, potentially leading to improved functional outcomes for patients.
The frequency-domain parameters provided additional insights into the effects of MRgFUS on tremor dynamics. The peak power ratio, a key measure of tremor intensity, significantly decreased in postures P2 and P3 (p ⩽ 0.03), reflecting a disruption in the dominant tremor frequency component. Tremor peak power in PSD showed a decreasing trend, although statistical significance was not reached in most postures. The principal peak in PSD exhibited reductions posttreatment, though not consistently significant, suggesting potential shifts in tremor frequency distribution. These findings indicate that while frequency-based measures provide valuable insights, time-domain parameters, particularly RMS and margin factor, may be more robust in detecting immediate posttreatment changes.
To validate the effectiveness of accelerometer-derived features, correlation analyses between objective parameters and clinical tremor severity (CRST sub-scores) were conducted. RMS exhibited a significant positive correlation with UEP in Posture P1 (r = 0.644, p = 0.002), confirming the accelerometer’s ability to capture tremor amplitude changes. Margin factor showed the strongest negative correlation with UEP in posture P4 (r = −0.83, p < 0.001), suggesting that increased margin factor reflects clinically meaningful tremor reductions. Peak power ratio also demonstrated moderate correlation with clinical scores, indicating that frequency-domain measures can complement time-domain parameters in tracking treatment efficacy. However, parameters such as crest factor and impulse factor did not show strong correlations, suggesting they may be less useful for tremor assessment post-MRgFUS. These correlations reinforce the potential of accelerometer-based metrics as objective biomarkers for tremor severity and treatment response, offering an additional layer of precision beyond traditional clinical scales.
The distinct patterns observed in posture-specific metrics highlight the need to evaluate both average tremor characteristics, such as RMS and peak power ratio, and extreme variations, such as margin factor, for a comprehensive understanding of tremor dynamics. Our findings suggest that a combination of RMS, margin factor, and peak power ratio may provide the most sensitive and clinically relevant markers for monitoring MRgFUS outcomes. However, the study’s limitations must be acknowledged. The small sample size, particularly in posture P4 (n = 7), necessitates further validation in larger cohorts. The short follow-up period of 1-day posttreatment limits the ability to assess the long-term effects of MRgFUS. The integration of accelerometer-based monitoring into clinical practice requires standardized protocols to ensure reproducibility and reliability across diverse patient populations.
Limitations and strengths
We are aware of the limitations of our study; first of all, the sample size, which significantly affects the generalizability of the results. However, we are confident that these results can open opportunities for a multicentre study with a larger sample size as a further step. Moreover, although the follow-up period in the present study was relatively short, this did not interfere with the main purpose of establishing feasibility and validity of the method. Both limitations are very likely responsible of the lack of clinical variety of our patients; indeed, none of the participant experienced postprocedural adverse effects but only periprocedural side effects. We acknowledge that weakness may modify tremor characteristics, such as amplitude or frequency, and could also influence the clinical tremor score itself. However, the main purpose of this proof-of-concept study was to demonstrate the correlation between clinical tremor scores and accelerometer parameters. In this context, even if weakness were to occur, both the clinical score and accelerometer-derived measures would likely be affected in parallel, and thus the core objective of validating the correlation would remain intact.
The strength and innovative aspect of the current work compared to previous studies exploring other kinematics techniques to measure the outcome of MRgFUS in patients with ET was the use of a tri-axis accelerometer in the context of this surgical procedure. This type of accelerometer allows to measures postural and action aspects of the tremor with the possibility of filtering the physiological tremor with a single device making significantly cost effective the use of this digital tool. Previously, Baek et al. positioned three accelerometers on the limb being treated with MRgFUS, and found an 80%–95% improvement in tremor amplitude. 21
The SVM of the filtered tri-axial accelerations, the principle calculated parameter by the studied device, reduced the dependence on sensor placement and posture variability and does not directly represent raw physiological signals. Therefore, the kinematic technique adopted in this study allows to have a complete quantification of different aspects of the ET and, thus, guarantee a reliable measure of the outcome of the surgery taking into account the functionality of the treated arm in performing different tasks. Indeed, the accelerometer was also used while the participants were holding a pen providing an objective measure of the impact of the tremor on the writing task.
Conclusion
This study highlights the potential of objective tremor quantification using accelerometer-derived features in evaluating MRgFUS thalamotomy for ET. The significant reductions in RMS and peak power ratio, combined with the substantial increase in margin factor, suggest that MRgFUS not only reduces tremor amplitude but also alters tremor rhythmicity, leading to improved postural control. The strong correlations between clinical tremor scores and accelerometer-derived measures reinforce the value of motion analysis as a quantitative tool for treatment assessment. Future research with larger patient cohorts and longer follow-up periods will be crucial in refining these findings and establishing accelerometer-based metrics as reliable, valid, and, responsive markers for tremor evaluation in clinical practice.
Supplemental Material
sj-docx-1-tan-10.1177_17562864251406534 – Supplemental material for Objective tremor monitoring using tri-axis accelerometer in MRgFUS thalamotomy for essential tremor: a feasibility study
Supplemental material, sj-docx-1-tan-10.1177_17562864251406534 for Objective tremor monitoring using tri-axis accelerometer in MRgFUS thalamotomy for essential tremor: a feasibility study by Kai-Chun Liu, Antonella Macerollo, Hoon-Ming Heng, Pei-Chiang Chen, Ming-Kuei Lu, Chun Ming Chen, Chon-Haw Tsai and Jui-Cheng Chen in Therapeutic Advances in Neurological Disorders
Supplemental Material
sj-docx-2-tan-10.1177_17562864251406534 – Supplemental material for Objective tremor monitoring using tri-axis accelerometer in MRgFUS thalamotomy for essential tremor: a feasibility study
Supplemental material, sj-docx-2-tan-10.1177_17562864251406534 for Objective tremor monitoring using tri-axis accelerometer in MRgFUS thalamotomy for essential tremor: a feasibility study by Kai-Chun Liu, Antonella Macerollo, Hoon-Ming Heng, Pei-Chiang Chen, Ming-Kuei Lu, Chun Ming Chen, Chon-Haw Tsai and Jui-Cheng Chen in Therapeutic Advances in Neurological Disorders
Supplemental Material
sj-docx-3-tan-10.1177_17562864251406534 – Supplemental material for Objective tremor monitoring using tri-axis accelerometer in MRgFUS thalamotomy for essential tremor: a feasibility study
Supplemental material, sj-docx-3-tan-10.1177_17562864251406534 for Objective tremor monitoring using tri-axis accelerometer in MRgFUS thalamotomy for essential tremor: a feasibility study by Kai-Chun Liu, Antonella Macerollo, Hoon-Ming Heng, Pei-Chiang Chen, Ming-Kuei Lu, Chun Ming Chen, Chon-Haw Tsai and Jui-Cheng Chen in Therapeutic Advances in Neurological Disorders
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.