
Abstract

Keywords
In Parkinson’s disease (PD), the motor symptoms still dominate, not only in diagnosis, but especially in therapy. The non-motor symptoms (NMS), on the other hand, are still an open field, both in recognition and assessment, as well as in diagnosis and, above all, in therapy.
Until the 1990s, NMS were generally regarded as secondary consequences of PD, sometimes as comorbidities. In addition, the medication was also blamed for some of them, although some of the various NMS had long ago been described by James Parkinson before effective therapies were developed. 1 Even today, one can still find NMS listed as side effects in the regulatory approvals for several PD medications, even though these correspond to symptoms of the disease and not medication-derived AEs used. For a long time, there was also a certain skepticism when it came to examining NMS. I (W.H.J.) still remember when I wanted to investigate colonic transit time in PD in the late 1980s, and at the time, my professor shook his head in disbelief and asked what the intestines had to do with PD. 2
Unfortunately, this neglect of NMS still haunts us today. Extensive studies have now been carried out on NMS, providing many valuable insights. The involvement of the gastrointestinal tract in PD is well established and has also generated many new ideas and hypotheses3,4; however, we are still lagging behind in terms of new therapy options. And this particularly affects the challenges of NMS symptoms (Figure 1).
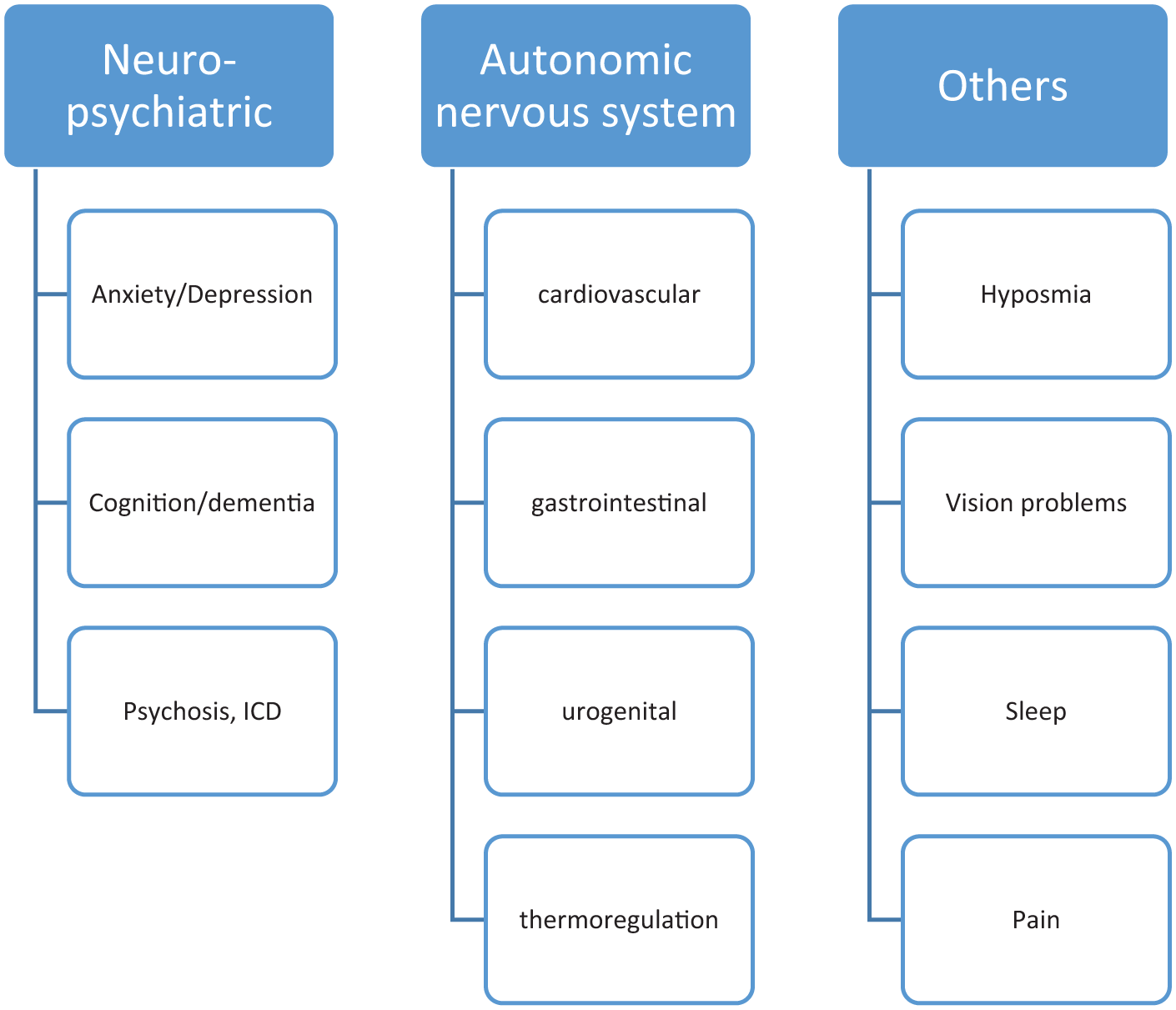
Listing of various domains for non-motor symptoms in PD.
Although various NMS therapies are available, they have mostly been adopted from similar indications for other disorders. This means that medications that are used for bladder disorders are also used for comparable bladder disorders in PD, but have not been formally studied in this regard. For example, there are only specific studies and approvals for sialorrhea and bladder dysfunction,5,6 for example.
To treat NMS, it is necessary first to recognize and diagnose them correctly. Since this usually does not fall into our area of expertise, that is, neurology or movement disorders, we first have to acquire relevant knowledge or inspire and motivate colleagues from other areas of expertise who will then help us. And that is a good number of specialist areas, pars pro toto:
Psychiatry
Ophthalmology
Gastroenterology
Cardiology
Urology
Pain management
We then have to understand the diagnostics and their results. We then need to further understand the therapy and its influence on the other symptoms. It must be clear to us, but also to the specialists consulted, that the various therapy options cannot be transferred 1:1 to other diseases, even if the symptoms are very similar, for example, neuropsychiatric7–9 and cardiovascular symptoms.10,11 Above all, we need specific guidelines. 12 The question arises as to whether we need to change something, and if so, what we need to change.
We all need to become more aware that NMS are not regarded as secondary symptoms but are seen on an equal footing with the motor symptoms of PD. We need to adequately diagnose and classify these symptoms. Specific therapy must then be carried out. As with other diseases, we no longer treat the symptom non-specifically, but rather specifically if we know the cause of the symptom. This Special Collection should and will contribute to this.