
Abstract
Background:
Inflammatory biomarkers, key predictors of ischemic stroke prognosis, may exhibit sex-specific predictive patterns.
Objectives:
This study investigates sex-based differences in inflammatory biomarkers as predictors of 90-day clinical outcomes in acute ischemic stroke patients undergoing mechanical thrombectomy (MT).
Design:
Multicenter retrospective study.
Methods:
This study included 970 patients consecutively treated with MT for anterior circulation large vessel occlusion between 2016 and 2023. Inflammatory indices, including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio, monocyte-to-lymphocyte ratio (MLR), C-reactive protein (CRP), systemic inflammation response index, and systemic immune-inflammation index, were measured on admission and 24-h post-MT. Inverse probability weighting was used to balance baseline characteristics between male and female patients. Least absolute shrinkage and selection operator regression and logistic regression were used to identify independent predictors of 90-day good functional outcomes (modified Rankin scale (mRS) score 0–2) and death, stratified by sex and age groups (<55 and ⩾55 years).
Results:
In the male weighted population (516 patients), multivariable analysis showed that MLR (odds ratio (OR): 0.37, 95% confidence interval (CI): 0.13–0.95, p = 0.041), 24-h NLR (OR: 0.88, 95% CI: 0.83–0.94, p < 0.001), and 24-h MLR (OR: 0.33, 95% CI: 0.12–0.94, p < 0.001) were independent predictors of 90-day good functional outcome with age-specific differences noted. Twenty-four-hour MLR (OR: 5.05, 95% CI: 1.36–4.28, p = 0.047) and erythrocyte sedimentation rate (OR: 1.02, 95% CI: 1.01–1.04, p = 0.025) were independent predictors of death, respectively, for men <55 and men ⩾55 years. In the weighted female population (454 patients), 24-h NLR (OR: 0.89, 95% CI: 0.81–0.96, p = 0.007) and 24-h CRP (OR: 0.98, 95% CI: 0.97–0.99, p = 0.029) were independent predictors of good functional outcomes. Twenty-four-hour CRP was also an independent predictor of 90-day death (OR: 1.01, 95% CI: 1.00–1.02, p = 0.017) in women with no age-specific differences noted. Interaction analysis revealed significant sex-specific relationships for MLR and CRP but not for NLR.
Conclusion:
This study highlights sex-based differences in the predictive value of widely available inflammatory biomarkers for stroke outcomes. MLR was a distinct predictor in men, while CRP was uniquely associated with outcomes in women. These findings underscore the need for sex-stratified approaches in stroke management and research.
Plain language summary
Why was the study done? Inflammatory markers are important for predicting how well a person will recover from an ischemic stroke. These markers may affect men and women differently. This study looks at how these markers predict recovery in men and women after undergoing mechanical thrombectomy (MT) for an acute ischemic stroke. What did the researchers do? This study included 970 patients treated with MT for large vessel occlusion. Several inflammatory markers were measured when the patients arrived at the hospital and 24 hours after the thrombectomy. The study used a statistical method called inverse probability weighting to adjust for differences between male and female patients. Different statistical models were used to find predictors of good recovery and death, based on gender and age groups (<55 years and over 55 years). What did the researchers find? For men (516 patients), the analysis showed that higher admission MLR (an inflammatory marker based on blood cells) and NLR (another blood-cell-derived marker) 24 hours after the procedure were linked to better recovery. Additionally, higher MLR 24 hours after MT and ESR (a different marker) were linked to a higher risk of death in younger and older men, respectively. For women (454 patients), NLR and CRP (inflammation-related blood protein) 24 hours after MT were linked to better recovery. CRP was also associated with a higher risk of death, but there were no differences based on age in women. What do the findings mean? The study shows that men and women may have different inflammatory markers that can predict stroke recovery. For men, MLR was a key marker, while for women, CRP was more important. These findings suggest that stroke treatment and research should consider sex-based differences to improve patient outcomes.
Introduction
Mechanical thrombectomy (MT) represents the standard of care for eligible patients with acute ischemic stroke caused by large vessel occlusion (LVO). 1 However, despite advances in endovascular therapies, functional outcomes after MT remain variable, influenced by a range of demographic, clinical, radiological, and biological factors. 2 Among these, inflammatory biomarkers have garnered increasing attention for their potential to predict stroke outcomes. 3
Emerging evidence has highlighted the importance of sex differences in stroke pathophysiology, risk factors, response to treatment, and stroke outcomes.4–6 Sex-related differences extend to stroke-induced inflammatory responses, which are integral to stroke pathogenesis and poststroke outcomes, with these responses exhibiting marked sexual dimorphism.7,8 Several inflammatory markers, especially adopted blood sample indices based on leukocyte, neutrophil, lymphocyte, and monocyte counts, are widely used to evaluate the severity and predict the prognosis of stroke in clinical settings.9,10 These inflammatory indices are also available for acute ischemic stroke patients undergoing MT. However, their prognostic value in the context of sex differences has remained unexplored. In this regard, we aimed to investigate sex-based differences in inflammatory predictors of clinical outcomes in a real-world population of patients with acute ischemic stroke patients treated with MT for anterior circulation LVO.
Methods
Study design and patients
This retrospective multicenter cohort study included consecutive acute stroke patients aged 18 years or older treated with MT for anterior circulation LVO in four thrombectomy centers: Charing Cross Hospital, Imperial College Healthcare NHS Trust, London, UK; St George’s University of London, London, UK; Udine University Hospital, Udine, Italy; and Boston Medical Center, Boston, MA, USA; between January 1, 2016 and March 30, 2023 with local stroke registries available.11–13 The study was conducted in accordance with the recommendations of the World Medical Assembly (Helsinki 1964 and later revisions). All patients were managed according to standardized clinical protocols, and relevant clinical and laboratory data were collected prospectively on admission.
Patient inclusion and exclusion criteria for the analysis
The criteria for patient selection were: (1) age ⩾18 years; (2) National Institutes of Health Stroke Scale score 6 or more; (3) Alberta Stroke Program Early CT score 5 or more (17); (4) LVO sites: distal internal carotid artery, middle cerebral artery segments M1 or M2; (5) initiation of the MT had to be possible within 6 h after the stroke onset; (6) pre-stroke modified Rankin Scale (mRS) score of 0–2. Intravenous thrombolysis (IVT) with intravenous tissue plasminogen activator or Tenecteplase was administered in all patients who presented within 4.5 h of stroke symptom onset without contraindications according to the guidelines. 14 For this analysis, we excluded stroke patients with basilar artery occlusion and patients that met DAWN or DEFUSE 3 eligibility criteria.15,16 Moreover, for the purpose of this analysis, we excluded patients with a concomitant condition which could potentially alter the inflammation biomarkers, in particular: (1) ongoing effect of immunomodulatory or immunosuppressive drugs, (2) ongoing infection or infections developed within 48 h after admission, (3) chronic inflammatory diseases, (4) hematological disorders, (5) cancer (active and/or under treatment), (6) major trauma or surgical procedures in the previous 28 days, (7) acute myocardial infarction with or without ST elevation, (8) severe liver or kidney dysfunction (eGFR < 30 ml/min), and (9) recent transfusion (<7 days before admission) or transfusion done within 24 h after admission.
Data collection
Baseline demographics, including age and sex, and pre-stroke risk factors such as hypertension, hypercholesterolemia, diabetes mellitus, alcohol use, smoking status, and history of transient ischemic attack or ischemic stroke, were prospectively documented for each patient. Procedural variables included the method of prehospital care (mothership or drip-and-ship), knowledge of stroke onset time, location of LVO, IVT administration, recanalization time, and type of anesthesia used. Measured biomarkers included C-reactive protein (CRP), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), systemic inflammation response index (SIRI), and systemic immune-inflammation index (SII). Analyses of inflammatory markers—including white blood count (WBC), MPV, neutrophil count (N), platelet count (P), lymphocyte count (L), and monocyte (M)—were conducted in the local laboratory department on admission and after 24 h from the index event. Laboratory measurements were performed 60 min after the onset of blood collection. The NLR was determined as N/L in the respective collection timings; SIRI was defined as N × (M/L) in the respective collection timings; SII was defined as P × [N/L] in the respective collection timings; PLR defined as P/L in the respective collection timings; finally, MLR was defined as M/L in the respective collection timings. Functional outcome was assessed using the mRS score, evaluated by local stroke neurologists. A favorable outcome was defined as an mRS score of 0–2 at 90 days (±14 days). Mortality was evaluated within 90 days poststroke to capture fatal outcomes in both patient groups. See Supplemental Methods for further description of additional outcomes.
Statistical analysis
Categorical variables are presented as count and percentage, continuous variables as mean and standard deviation or median and interquartile range according to normal distribution. We used inverse probability weighting (IPW) to balance the baseline characteristics of the exposed and unexposed cohorts (male vs female groups), aiming to reduce the confounding factors on study outcomes. A detailed methodological explanation of the IPW estimation process is available in the Supplemental Methods. In brief, weights were obtained calculating the probability being in the group of male versus female while controlling for a set of relevant variables that could have influenced the outcome. The weights obtained were then used to balance the baseline covariates, therefore creating a pseudo-population independent of the measured confounders (i.e., pseudo-randomization). 17 Statistical comparisons were performed in the weighted population between patient groups using the χ2 test, Fisher exact test, Student’s t test, and Mann–Whitney U as indicated for dichotomous or continuous variables. To identify stable predictors in multivariate models, we adopted the least absolute shrinkage and selection operator (LASSO) regression. LASSO linear/Gaussian regression allowed the selection of measured biomarkers that are most associated with favorable functional outcomes at 90 days (mRS 0–2) and death stratified by sex (male and female) and age groups (<55 and ⩾55 years) in the weighted population. Further, we conducted a crude logistic regression analysis to examine the unadjusted association of those markers with study outcomes. Variables with a significant association with this study’s outcomes (p ⩽ 0.05) were considered for multivariate logistic regression analysis with statistical significance set at a p < 0.05. Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were obtained. To avoid potential collinearity and enhance interpretability, we conducted separate LASSO and logistic regression models for admission and 24-h blood test variables. Biomarkers measured at the two time points were analyzed independently and not included simultaneously in the same model. OR regression with restricted cubic splines was employed to model the continuous relationship between measured biomarkers of interest and the OR of study outcomes. Knots for the splines were set at the 10th, 50th, and 90th percentiles of the biomarker of interest. The median value of the biomarker was used as the reference, and ORs for varying levels were estimated relative to this reference. Log ORs were computed and exponentiated to yield ORs, with 95% CIs calculated using the standard errors of the log ORs. CIs were derived by adjusting each log OR by ±1.96 times the standard error, then exponentiating the bounds. To identify a clinical cut-off for the measured biomarkers of interest, the OR curve was examined to locate values where the OR approximated 1, indicating no significant increase or decrease in risk. The measured biomarker level closest to OR = 1 was selected as a potential cut-off point for stratification. Lastly, marginal effects analysis was employed to visualize and examine predicted probabilities of favorable outcomes across the range of admission measured biomarkers stratified by sex. Statistical significance was set at a p-value of <0.05. R Studio Posit PBC (version 2024.4) was used for statistical analysis.
Results
Our analysis included 970 patients with acute ischemic stroke due to LVO treated with MT (Supplemental Figure 1). Among the included patients, 516 (53.2%) were males and 454 (46.8%) were females. Table 1 reports unweighted and weighted results for baseline characteristics. Overall, good balance was obtained for all major baseline variables of interest (Supplemental Figures 2 and 3 and Table 1). Supplemental Table 1 reports the outcome distribution in the weighted population.
Baseline characteristics.

SMD < 0.10 indicates that groups are well balanced.
AFDAS, atrial fibrillation newly detected in close temporal proximity to the index stroke; ASPECTS, Alberta Stroke Program Early CT Score; ICA, internal carotid artery; ICH, intracerebral hemorrhage; IS, ischemic stroke; KAF, known atrial fibrillation; mRS, modified Rankin scale; NIHSS, National Institutes of Health Stroke Scale; SMD, standardized means difference; TIA, transient ischemic attack.
Table 2 shows blood tests collected on admission and at 24 h from the index event in the weighted population. On admission, the two groups significantly differed in terms of number of platelets (p < 0.001), erythrocyte sedimentation rate (ESR; p < 0.001), MLR (p = 0.001), and SIRI (p = 0.015). After 24 h from the index event, platelets (p < 0.001) and PLR (p = 0.037) were significantly different between male and female patients. The rest of the blood test on admission and at 24 h from the index event are reported in Supplemental Table 2.
Blood test on admission and after 24 h in the weighted population.
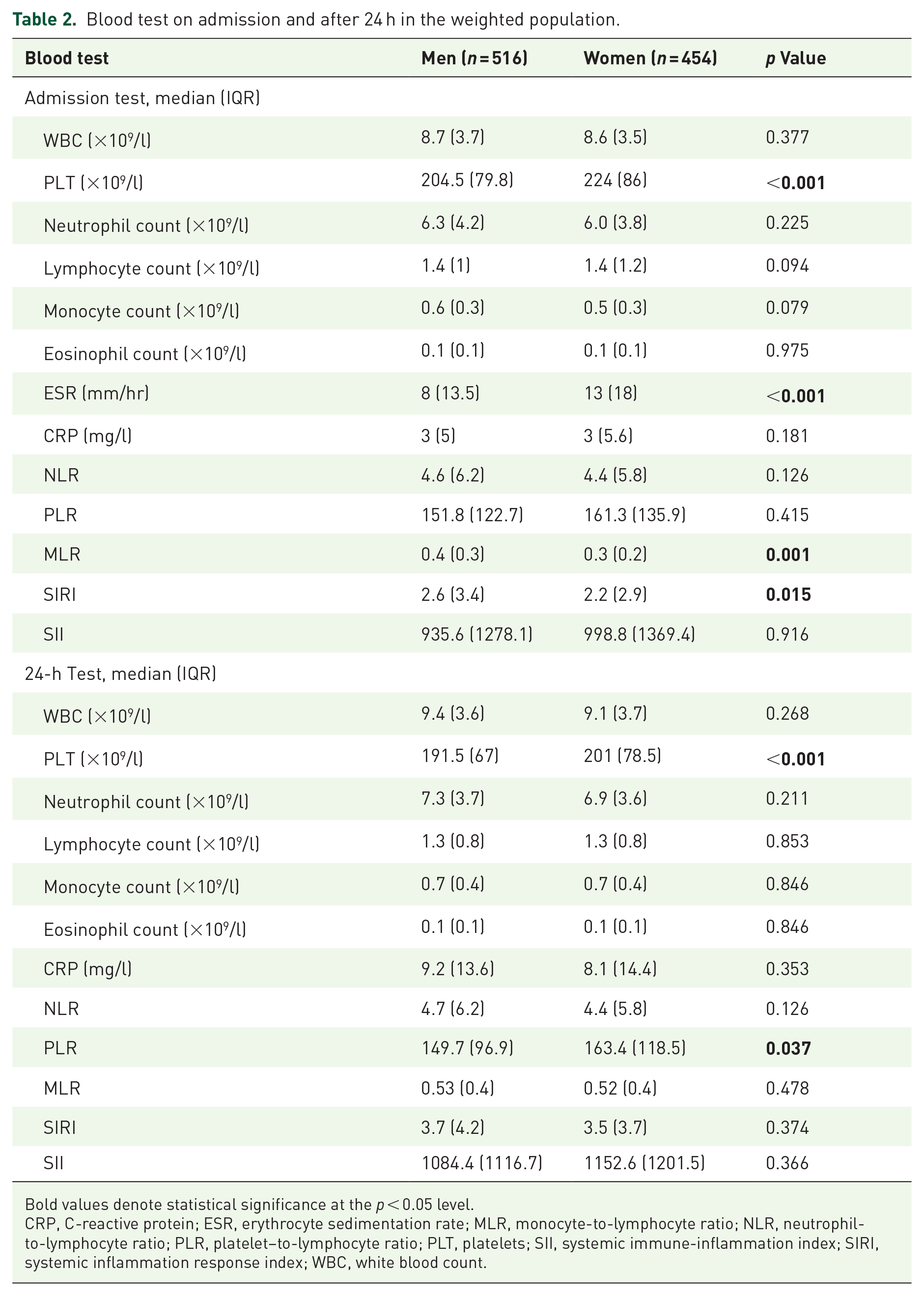
Bold values denote statistical significance at the p < 0.05 level.
CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; MLR, monocyte-to-lymphocyte ratio; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet–to-lymphocyte ratio; PLT, platelets; SII, systemic immune-inflammation index; SIRI, systemic inflammation response index; WBC, white blood count.
LASSO regression analysis to identify predictors of study outcomes
We conducted a LASSO regression analysis to identify the variables most strongly associated with favorable functional outcomes at 90 days, stratified by sex (male and female) and age groups (<55 and ⩾55 years) in the weighted population. The values of the LASSO coefficients for each of the included variables after variation of the regularization parameter lambda are shown in Figure 1 for men and Figure 2 for women. The plot shows how the relative importance of each variable changes at increasing the model size. At optimal model size (best lambda value determined by cross-validation +1 standard error), the variables which were most associated with the favorable functional outcomes at 90 days in male population were admission ESR, NLR, PLR, and MLR and 24-h WBC, platelets, lymphocyte count, eosinophil count, CRP, NLR, and MLR. For men with age <55 years, these were admission PLR, MLR, SII, and 24-h WBC, lymphocytescount, monocyte count, CRP, and MLR. In men with age ⩾55 years, the variables were admission ESR, NLR, and 24-h WBC, platelets, neutrophil count, lymphocyte count, eosinophil count, CRP, NLR, and MLR. In the overall female population, the variables that were most associated with the favorable functional outcomes at 90 days were 24-h platelets, monocyte count, CRP, NLR, neutrophil count, and eosinophil count. For women with age <55 years, these were 24-h lymphocyte count and NLR. In women with age ⩾55 years, the variables were admission platelets, neutrophil count, lymphocyte count, monocyte count, CRP, ESR, and 24-h neutrophil count, eosinophil count, CRP, NLR, MLR, platelets, and WBC. The coefficient estimates relative to the optimal model size are reported in Supplemental Table 3.

LASSO linear regression models for favorable functional outcomes at 90 days in men. Panels show the coefficients of the LASSO linear regression analysis for the prediction of favorable functional outcomes at 90 days in the overall male population and by age subgroups at increasing lambda values. The regularization parameter lambda indicates the selection power of each model, that is, the higher the lambda values, the lower the number of variables of the model. Lambda values at 1 standard error from the optimal one, selected by cross-validation, are displayed as red dashed lines.

LASSO linear regression models for favorable functional outcomes at 90 days in women. Panels show the coefficients of the LASSO linear regression analysis for the prediction of favorable functional outcomes at 90 days in the overall female population and by age subgroups at increasing lambda values. The regularization parameter lambda indicates the selection power of each model, that is, the higher the lambda values, the lower the number of variables of the model. Lambda values at 1 standard error from the optimal one, selected by cross-validation, are displayed as red dashed lines.
We then conducted a similar LASSO regression analysis to identify the variables most strongly associated with 90-day death, stratified by sex (male and female) and age groups (<55 and ⩾55 years) in the weighted population. The values of the LASSO coefficients for each of the included variables after variation of the regularization parameter lambda are shown in Supplemental Figure 4 for men and Supplemental Figure 5 for women. At optimal model size (best lambda value determined by cross-validation +1 standard error), the variables which were most associated with 90-day death in the male population were admission NLR, PLR, MLR, ESR, and 24-h WBC, platelets, lymphocyte count, eosinophil count, CRP, NLR, and MLR. For men with age <55 years, these were admission MLR and SII and 24-h WBC, lymphocyte count, monocyte count, CRP, and MLR. In men with age ⩾55 years, the variables were admission ESR and NLR, and 24-h WBC, platelets, neutrophil count, lymphocyte count, eosinophil count, CRP, NLR, and MLR. In the overall female population, the variables which were most associated with 90-day death were 24-hneutrophil count, CRP, NLR while none of the admission blood tests. For women with age <55 years, the variables associated with 90-day death were 24-h lymphocyte count, CRP and NLR while none of the admission blood tests. In women with age ⩾55 years, the variables were admission monocyte count and PLR, 24-h neutrophil count, CRP, and NLR. The coefficient estimates relative to the optimal model size are reported in Supplemental Table 4.
Predictors of clinical outcomes in men
In the weighted male population, predictors of 90-day good functional outcome (mRS 0–2 at 90 days) were assessed using logistic regression (Table 3).
Logistic regression analysis to predict good 90-day functional outcome (mRS 0–2) in the male weighted population.

Bold values denote statistical significance at the p < 0.05 level.
CI, confidence interval; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; MLR, monocyte-to-lymphocyte ratio; mRS, modified Rankin scale; NLR, neutrophil-to-lymphocyte ratio; OR, odds ratio; PLR, platelet-to-lymphocyte ratio; PLT, platelets; SII, systemic immune-inflammation index; WBC, white blood count.
After multivariate analysis, only MLR (OR: 0.37, 95% CI: 0.13–0.95, p = 0.041) resulted to be an independent predictor of good functional outcome. Regarding the 24-h blood tests, multivariate analysis showed that 24-h NLR (OR: 0.88, 95% CI: 0.83–0.94, p < 0.001) and 24-h MLR (OR: 0.33, 95% CI: 0.12–0.94, p < 0.001) were independent predictors of 90-day good functional outcome after the index event. The logistic regression analysis with restricted cubic splines revealed a nonlinear association between admission MLR, 24-h MLR, 24-h NLR, and the OR of 90-day good functional outcome (Figure 3). At the point where the OR approximated 1, the analysis identified a cut-off of 0.40 for MLR, 0.55 for 24-h MLR, and 5.47 for 24-h NLR. Subgroup analysis by age demonstrated that in men aged <55 years, 24-h MLR was significantly associated with 90-day good functional outcome (OR: 0.08, 95% CI: 0.01–0.69, p = 0.026). Among men aged ⩾55 years, admission NLR (OR: 0.90, 95% CI: 0.86–0.95, p < 0.001), 24-h NLR (OR: 0.82, 95% CI: 0.70–0.95, p = 0.010), and 24-h MLR (OR: 0.42, 95% CI: 0.15–0.93, p = 0.009) were independent predictors of outcome in multivariate models.

Margin plots of MLR, 24-h MLR, 24-h-CRP, and 24-h NLR with probability of favorable functional outcomes at 90 days by sex. Each graph shows the predicted probability (solid line) and 95% confidence interval (shade) of different outcomes.
We also assessed predictors of 90-day death in the weighted male population using logistic regression analysis. In the overall male population, after multivariate analysis, we did not find any independent predictors of death at 90 days. Conversely, in men <55 years, 24-h MLR was significantly associated with 90-day death (OR: 5.05, 95% CI: 1.36–4.28, p = 0.047) while in men aged ⩾55 years, ESR on admission was an independent predictor of outcome (OR: 1.02, 95% CI: 1.01–1.04, p = 0.025) (Supplemental Table 5).
Predictors of clinical outcomes in women
In the weighted female population, multivariate analysis demonstrated that 24-h NLR (OR: 0.89, 95% CI: 0.81–0.96, p = 0.007) and 24-h CRP (OR: 0.98, 95% CI: 0.97–0.99, p = 0.029) (Table 4) were independent predictors of good functional outcomes. The logistic regression analysis with restricted cubic splines revealed a nonlinear association between admission 24-h NLR, 24-h CRP, and the OR of 90-day good functional outcome (Supplemental Figure 7). At the point where the OR approximated 1, the analysis identified a cut-off of 5.74 for 24-h NLR and 10.52 for 24-h CRP. Age-stratified analysis revealed no independent predictors in women <55 years, while in women aged ⩾55 years, 24-h NLR and 24-h CRP were significantly associated with 90-day good functional outcome, respectively (OR: 0.91, 95% CI: 0.84–0.96, p = 0.006) and (OR: 0.98, 95% CI: 0.96–0.99, p = 0.039) in multivariate model (Table 4).
Logistic regression analysis to predict good 90-day functional outcome (mRS 0–2) in the women weighted population.
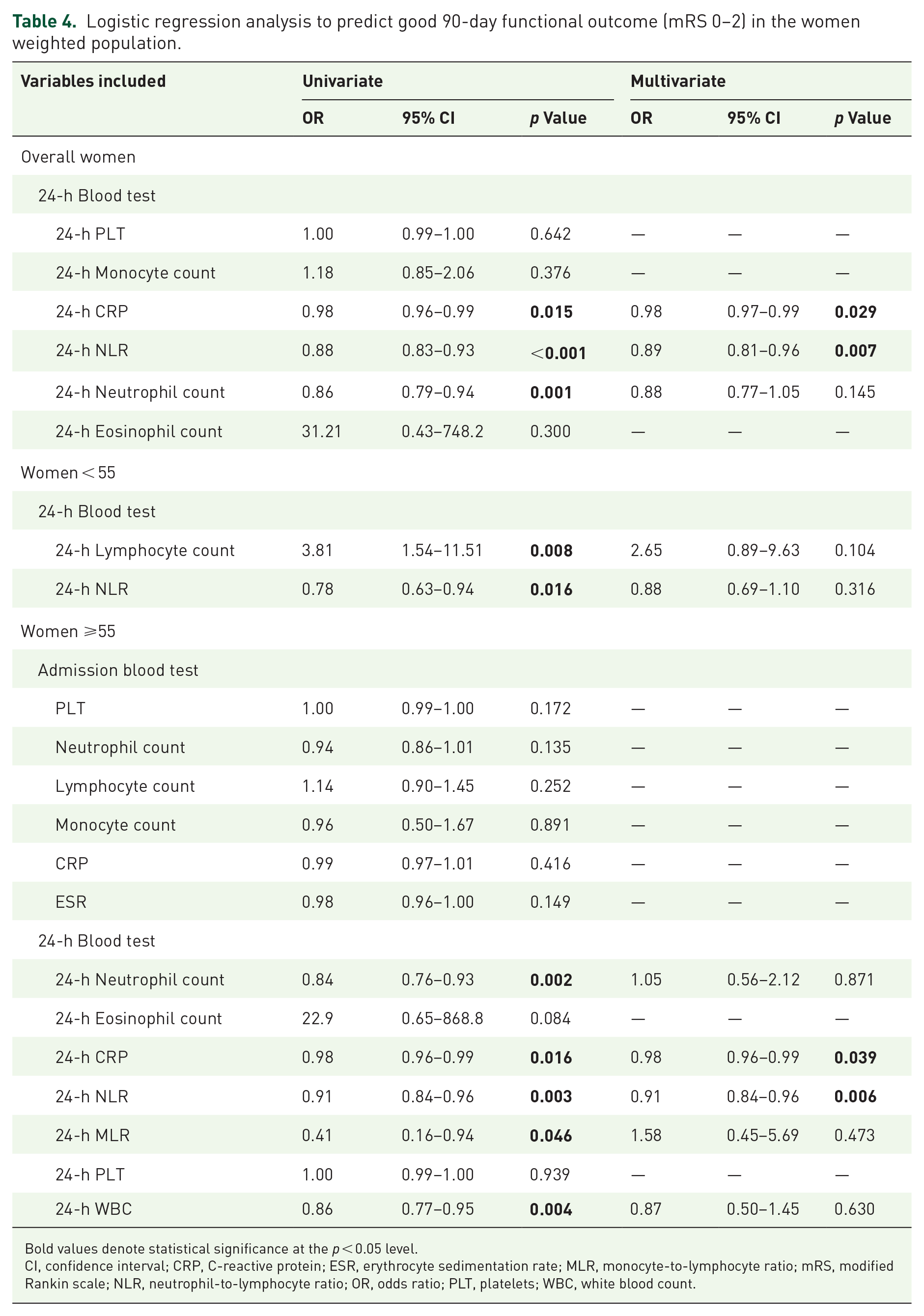
Bold values denote statistical significance at the p < 0.05 level.
CI, confidence interval; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; MLR, monocyte-to-lymphocyte ratio; mRS, modified Rankin scale; NLR, neutrophil-to-lymphocyte ratio; OR, odds ratio; PLT, platelets; WBC, white blood count.
We also assessed predictors of 90-day death in the weighted female population using logistic regression analysis. In the overall female population, after multivariate analysis, 24-h CRP was an independent predictor of death at 90 days (OR: 1.01, 95% CI: 1.00–1.02, p = 0.017) (Supplemental Table 6). In women <55 years, 24-h CRP (OR: 1.01, 95% CI: 1.00–1.03, p = 0.030) and 24-h NLR (OR: 1.14, 95% CI: 1.06–1.23, p < 0.001) were significantly associated with 90-day death. In women aged ⩾55 years, 24-h CRP (OR: 1.01, 95% CI: 1.00–1.03, p = 0.043) and 24-h neutrophil count were independent predictors of outcome (Supplemental Table 6).
Findings on sex interaction with inflammatory biomarkers
Significant interactions were observed between admission MLR, 24-h MLR, and 24-h CRP with sex in predicting a 90-day good functional outcome (p = 0.011, p < 0.001, and p = 0.045, respectively). In contrast, 24-h NLR was associated with the probability of a 90-day good functional outcome irrespective of sex (p = 0.482). Figure 3 illustrates adjusted margin plots highlighting the relationships between inflammatory biomarkers and the probability of 90-day good functional outcome, stratified by sex.
Discussion
This study, based on an IPW analysis, investigated sex-based differences in inflammatory biomarkers as predictors of functional outcomes and mortality in patients with acute ischemic stroke treated with MT. Our findings demonstrated that while NLR serves as a significant predictor of clinical outcomes in both sexes, certain inflammatory indices exhibit sex-specific differences. Specifically, MLR measured at 24 h was uniquely associated with outcomes in men, whereas CRP at 24 h emerged as a predictor exclusively in women. These results underscore a potential sex-based differentiation in the prognostic value of inflammatory biomarkers, suggesting that these indices may reflect distinct sex-specific inflammatory pathways influencing clinical outcomes.
MLR is an inflammatory index that incorporates monocytes, which are critical mediators of the inflammatory response. 18 Monocytes, which arise from the hematopoietic system in the bone marrow, play a pivotal role in poststroke inflammation, contributing to tissue repair and remodeling but also potentially exacerbating injury through excessive pro-inflammatory activity. 19 To execute their functions, they are equipped with a range of sophisticated mechanisms, including scavenger receptors, low-density lipoprotein (LDL) receptors, toll-like receptors, chemokine and cytokine receptors, Fcγ receptors, and adhesion molecules. 18 Transcriptomic analysis showed that in human monocytes, there are 428 differentially expressed genes by sex although the female–male-fold change value was low. 20 Following ischemic injury, monocytes are rapidly recruited to the brain, where they differentiate into macrophages and secrete pro-inflammatory cytokines such as IL-1β and TNF-α.21,22 Previous studies documented a significant association between monocytes and risk of stroke more in men than in women. 23 Moreover, evidence suggests that mononuclear macrophages exhibit sex-specific differences in their response to stroke. 8 In male mice, higher numbers of activated macrophages infiltrate the brain, accompanied by an increased proportion of activated microglia and VLA-4-expressing cells that migrate into the infarcted region. 24 These differences may contribute to the larger infarct sizes observed in males or may reflect secondary effects of the heightened ischemic damage documented in young male animals compared to females. 19 In contrast, female mice exhibit predominantly anti-inflammatory phenotypes in microglia and macrophages, with greater expression of CD206. 25 Additionally, females display more robust anti-inflammatory responses mediated by IL-10-producing CD8+ CD122+ T cells. 25 Furthermore, spleen has been recently identified as an immediate reservoir of monocytes and it seems to exhibit sex differences in stroke outcomes. 8 Male mice exhibit a greater increase in CD4+ T cells and elevated expression of the VLA-4 adhesion molecule in the spleen compared to female mice following experimental stroke.22,25 Dotson et al. investigated the role of the spleen in stroke pathophysiology in both male and female mice. 26 The authors found that, in male mice, splenectomy prior to middle cerebral artery occlusion significantly reduced macrophage/monocyte populations, activated T cells, and ischemic injury, whereas these effects were not observed in female mice. Additionally, splenectomy in males resulted in a reduction in infarct size and activated microglia in the brain, although it did not influence stroke prognosis in females. 26 These findings highlight the sex-specific immune mechanisms that might influence the pathophysiological responses during the postischemic period. Understanding sex differences in poststroke neuroinflammation is particularly significant, highlighting the role of sex-stratified clinical and preclinical investigations. These analyses are essential for identifying and addressing these differences, ultimately facilitating the development of novel, sex-specific therapeutic approaches for both men and women.
Another original finding of our study is that elevated CRP levels were uniquely predictive of outcomes in women undergoing MT for acute ischemic stroke. Elevated serum CRP levels were observed in up to three-quarters of patients with ischemic stroke and may reflect a systemic inflammatory response, the extent of tissue injury, or concurrent infections.27,28 Experimental animal models of focal cerebral ischemia have demonstrated that CRP exacerbates secondary brain damage through activation of the complement system. 29 Several studies have investigated CRP as a prognostic marker in the early phases of stroke.30–32 Hertog et al. reported that stroke patients with CRP levels ⩾7 mg/l had a significantly higher risk of poor outcomes or death at 3 months. 33 Similarly, Meinel et al., in a cohort of 539 stroke patients, demonstrated that a prognostic model incorporating clinical variables (stroke severity, age, active cancer, pre-stroke disability), laboratory markers (CRP, glucose, creatinine), imaging biomarkers (white matter hyperintensities), and onset-to-admission time was strongly associated with the risk of futile recanalization after MT and/or IVT. 34 However, these studies examined the relationship between CRP and clinical outcomes in the general population, without stratifying results by sex. Women were found to have higher CRP concentrations than men, likely attributed to their greater accumulation of subcutaneous fat compared to men 35 and increased CRP levels have been associated with an increased risk of cardiovascular events, including stroke, particularly in women. 36 A recent study underscored the significance of high-sensitivity CRP, LDL cholesterol, and lipoprotein(a) as long-term predictors of cardiovascular risk in women. 37 Over a 30-year analysis, elevated CRP levels were linked to more than a 1.5-fold increase in stroke risk among women. Our study corroborates previous findings that highlight CRP as a significant biomarker in female patients with ischemic stroke. Nonetheless, additional research is necessary to validate its role as a reliable predictor of outcomes following stroke.
Finally, our study reinforces the pivotal role of NLR as a prognostic biomarker in stroke outcomes, aligning with existing evidence that highlights its relevance in acute ischemic stroke.38,39 Our findings regarding the prognostic value of NLR are consistent with previous studies, including that by Goyal et al., which demonstrated that admission NLR was independently associated with poor outcomes in patients with LVO stroke undergoing reperfusion therapy. 40 In line with our findings, recent data also support the predictive role of NLR in patients undergoing MT for posterior circulation LVO, further reinforcing the relevance of NLR as a general prognostic biomarker in stroke. 41 However, the current literature provides limited evidence regarding sex-specific differences in the predictive value of NLR for poststroke outcome. This gap underscores the need for more targeted investigations to determine if sex modifies the relationship between NLR and stroke prognosis. By demonstrating that NLR measured within 24 h is a significant predictor of functional outcomes and mortality across both sexes, our findings validate its broad applicability and underscore its importance in clinical practice.
Our analysis has several strengths: (1) a large patient cohort, (2) a multicenter study design, (3) stringent exclusion criteria ensuring robust patient selection, and (4) the clinical relevance and applicability of the findings. However, there are notable limitations. The retrospective, nonrandomized design is likely to have introduced biases. The reported associations in our nonrandomized study could be influenced by numerous potential confounders, even if statistical models were used to adjust for them. However, in several circumstances in which randomized trials are not available, observational studies are considered a useful tool to understand the effects of a treatment or different clinical services. In addition, if rigorously designed, this type of analysis could help to estimate the effects of interventions, particularly in everyday clinical practice. 42 Additionally, we lacked data on collateral status and stroke etiology, both significant confounders influencing clinical outcome. By focusing on patients undergoing MT for LVO in the anterior circulation, our results may not apply to patients with other types of strokes or those not eligible for MT. Further research in more diverse stroke populations could determine whether MLR, NLR, and CRP retain sex-specific predictive value for clinical outcomes across different treatment modalities. Lastly, we used standard CRP rather than high-sensitivity CRP, which may have reduced the precision in detecting subtle inflammatory responses. Future studies including prospective cohorts and external validation in independent populations will be essential to confirm the robustness and clinical utility of inflammatory biomarkers in stroke patients undergoing MT.
Conclusion
This study highlights the need for sex-stratified clinical and preclinical studies to elucidate the role of inflammation in determining stroke outcomes. Further research is fundamental to advancing the development of sex-specific therapeutic interventions and optimizing clinical outcomes for both men and women affected by ischemic stroke undergoing acute reperfusion therapies.
Supplemental Material
sj-docx-2-tan-10.1177_17562864251345719 – Supplemental material for Sex-based differences in inflammatory predictors of outcomes in patients undergoing mechanical thrombectomy: an inverse probability weighting analysis
Supplemental material, sj-docx-2-tan-10.1177_17562864251345719 for Sex-based differences in inflammatory predictors of outcomes in patients undergoing mechanical thrombectomy: an inverse probability weighting analysis by Gabriele Prandin, Matteo Foschi, Mariarosaria Valente, Liqun Zhang, Paresh Malhotra, Simona Sacco, Raffaele Ornello, Francesco Toraldo, Domenico Maisano, Caterina Del Regno, Filippo Komauli, Adelaida Gartner Jarmillo, Hakam Al-Karadsheh, Hamza Zahid, Piers Klein, Mohamad Abdalkader, Paolo Manganotti, Kyriakos Lobotesis, Thanh N. Nguyen, Gian Luigi Gigli, Soma Banerjee, Giovanni Merlino and Lucio D’Anna in Therapeutic Advances in Neurological Disorders
Supplemental Material
sj-docx-3-tan-10.1177_17562864251345719 – Supplemental material for Sex-based differences in inflammatory predictors of outcomes in patients undergoing mechanical thrombectomy: an inverse probability weighting analysis
Supplemental material, sj-docx-3-tan-10.1177_17562864251345719 for Sex-based differences in inflammatory predictors of outcomes in patients undergoing mechanical thrombectomy: an inverse probability weighting analysis by Gabriele Prandin, Matteo Foschi, Mariarosaria Valente, Liqun Zhang, Paresh Malhotra, Simona Sacco, Raffaele Ornello, Francesco Toraldo, Domenico Maisano, Caterina Del Regno, Filippo Komauli, Adelaida Gartner Jarmillo, Hakam Al-Karadsheh, Hamza Zahid, Piers Klein, Mohamad Abdalkader, Paolo Manganotti, Kyriakos Lobotesis, Thanh N. Nguyen, Gian Luigi Gigli, Soma Banerjee, Giovanni Merlino and Lucio D’Anna in Therapeutic Advances in Neurological Disorders
Supplemental Material
sj-docx-4-tan-10.1177_17562864251345719 – Supplemental material for Sex-based differences in inflammatory predictors of outcomes in patients undergoing mechanical thrombectomy: an inverse probability weighting analysis
Supplemental material, sj-docx-4-tan-10.1177_17562864251345719 for Sex-based differences in inflammatory predictors of outcomes in patients undergoing mechanical thrombectomy: an inverse probability weighting analysis by Gabriele Prandin, Matteo Foschi, Mariarosaria Valente, Liqun Zhang, Paresh Malhotra, Simona Sacco, Raffaele Ornello, Francesco Toraldo, Domenico Maisano, Caterina Del Regno, Filippo Komauli, Adelaida Gartner Jarmillo, Hakam Al-Karadsheh, Hamza Zahid, Piers Klein, Mohamad Abdalkader, Paolo Manganotti, Kyriakos Lobotesis, Thanh N. Nguyen, Gian Luigi Gigli, Soma Banerjee, Giovanni Merlino and Lucio D’Anna in Therapeutic Advances in Neurological Disorders
Supplemental Material
sj-docx-5-tan-10.1177_17562864251345719 – Supplemental material for Sex-based differences in inflammatory predictors of outcomes in patients undergoing mechanical thrombectomy: an inverse probability weighting analysis
Supplemental material, sj-docx-5-tan-10.1177_17562864251345719 for Sex-based differences in inflammatory predictors of outcomes in patients undergoing mechanical thrombectomy: an inverse probability weighting analysis by Gabriele Prandin, Matteo Foschi, Mariarosaria Valente, Liqun Zhang, Paresh Malhotra, Simona Sacco, Raffaele Ornello, Francesco Toraldo, Domenico Maisano, Caterina Del Regno, Filippo Komauli, Adelaida Gartner Jarmillo, Hakam Al-Karadsheh, Hamza Zahid, Piers Klein, Mohamad Abdalkader, Paolo Manganotti, Kyriakos Lobotesis, Thanh N. Nguyen, Gian Luigi Gigli, Soma Banerjee, Giovanni Merlino and Lucio D’Anna in Therapeutic Advances in Neurological Disorders
Supplemental Material
sj-pdf-1-tan-10.1177_17562864251345719 – Supplemental material for Sex-based differences in inflammatory predictors of outcomes in patients undergoing mechanical thrombectomy: an inverse probability weighting analysis
Supplemental material, sj-pdf-1-tan-10.1177_17562864251345719 for Sex-based differences in inflammatory predictors of outcomes in patients undergoing mechanical thrombectomy: an inverse probability weighting analysis by Gabriele Prandin, Matteo Foschi, Mariarosaria Valente, Liqun Zhang, Paresh Malhotra, Simona Sacco, Raffaele Ornello, Francesco Toraldo, Domenico Maisano, Caterina Del Regno, Filippo Komauli, Adelaida Gartner Jarmillo, Hakam Al-Karadsheh, Hamza Zahid, Piers Klein, Mohamad Abdalkader, Paolo Manganotti, Kyriakos Lobotesis, Thanh N. Nguyen, Gian Luigi Gigli, Soma Banerjee, Giovanni Merlino and Lucio D’Anna in Therapeutic Advances in Neurological Disorders
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.