
Abstract
Background:
Good outcomes in stroke care require swift diagnostics, for which magnetic resonance imaging (MRI) as first-line brain imaging is superior to computed tomography scans. Reduced length of stay (LOS) in hospital and emergency departments (ED) may optimize resource use. Fast-track stroke MRI was implemented as the primary imaging technique for suspected stroke, in the ED at Copenhagen University Hospital—Herlev and Gentofte in 2020.
Objectives:
We aimed to describe and compare LOS, MRI utilization, and the rate of strokes versus stroke-mimicking conditions on the stroke ward, before and after the implementation of fast-track MRI.
Design and method:
In this cross-sectional study, we used data from admissions to the neurologic ED and associated non-comprehensive stroke unit. We compared two time periods, that is, January 1–December 31, 2019, and January 1–December 31, 2020, before and after the implementation of fast-track stroke MRI.
Results:
There were 6650 admissions before and 7201 after implementation of fast-track stroke MRI. After implementation, we observed reductions in average LOS in hospitals from 56.0 to 38.6 h (p < 0.001), and LOS in ED from 9.17 to 8.63 h (p < 0.001). The use of inpatient MRI increased significantly, and the rate of acute ischemic stroke patients on the ward increased yet the rate of non-strokes remained unchanged. The association between shorter admissions and access to MRI remained (odds ratio 1.81, p < 0.001), after adjusting for sex, age, weekend admissions, and lockdown periods.
Conclusion:
Fast-track stroke MRI in ED associated with reduced LOS in hospital.
Plain language summary
Why was the study done? Swift diagnostics is essential, as stroke treatment is time sensitive. Brain imaging is a substantial part of stroke workups, as it allows doctors to distinguish blood clots from brain hemorrhages. Occasionally, imaging is a bottle neck ahead of treatment. Traditionally, CT (computed tomography) has been used in stroke care, but MRI (magnetic resonance imaging) is diagnostically superior, as it helps visualize brain tissue affected by a clot, even very early on. However, MRI is more time consuming than CT. I.e., for stroke imaging, not only the type of scan is of interest, but also associated logistics. What did the researchers do? We evaluated the change in hospital logistics, associated with a change in our first-line imaging technique for stroke - from CT in 2019 to MRI in 2020. We measured lengths of stay, both in hospital overall, and in the emergency department, rates of readmissions, and what diagnoses our patients had, when they were discharged after a full workup on the stroke ward (i.e., either a stroke, or something that mimics a stroke). What did the researchers find? Out of 13851 admissions, 6550 were admitted in 2019, when CT was the initial imaging technique, and 7201 in 2020, after MRI-first had been implemented. We observed a reduction in the average length of stay in hospital, from 56 hours before MRI-first and 38 hours after. The average length of stay in the emergency department also changed from 9.1 to 8.6 hours, after MRI implementation. The rate of readmission to the emergency department remained unchanged. Additionally, the rate of patients with strokes admitted to the stroke ward increased, indicating that we could identify stroke-mimicking conditions prior to admission. What do the findings mean? Implementing an MRI-first approach for suspected stroke, allowed us to improve our logistics, both on the stroke-ward, but also in the emergency department, whilst maintaining diagnostic accuracy.
Keywords
Background
Stroke is a clinical diagnosis, 1 yet brain imaging is an essential part of stroke workups, allowing distinction between ischemic and hemorrhagic causes of stroke. 1 However, these neuroimaging procedures can be a potential bottleneck ahead of medical treatment.2–4 Traditionally, computed tomography (CT) has been used for brain ischemia, despite the known diagnostic superiority of magnetic resonance imaging (MRI).2–5 MRI allows a more precise distinction between ischemic strokes and their mimics, estimation of duration of ischemia, improved treatment outcomes, and provides more etiologic insight, than CT.2–5 In addition, MRI can increase stroke clinicians’ confidence in their decision-making. 6 However, MRI is more resource-demanding and time-consuming per scan2,7 and inaccessible to some patients, for example, due to implanted electronic devices or claustrophobia. 8 This is potentially consequential, as stroke treatment is time-sensitive regardless of whether revascularization is attempted or not.7,9 Nevertheless, MRI is increasingly utilized for acute stroke diagnostics and is often procurable within 10 min of scan time.6,9
In comprehensive stroke centers and their associated emergency departments (EDs), where revascularization is available, MRI as the first-choice imaging technique for suspected stroke has been evaluated. It is associated with reduced length of stay (LOS) in hospitals,5,10–14 fewer stroke mimics admitted to the ward,10,12 and fewer patients diagnosed with a stroke, potentially due to a more apt identification of mimics. 12 Yet, also with increased MRI use. 10
Despite reductions in overall lengths of hospitalizations, previous attempts at implementing an MRI-first approach have increased LOS in ED.10,11 Crowding of EDs is problematic and can cause reduced quality of care and poorer treatment outcomes,10,15 which also applies in acute stroke care.10,16 In addition, prolonged admissions are associated with risks such as nosocomial infections and side effects of medications.4,17,18
Revascularization is not done on-site in our non-comprehensive stroke unit at Copenhagen University Hospital—Herlev and Gentofte in Denmark. However, a fast-track MRI-first approach was implemented in our ED, for patients with suspected stroke ineligible for revascularization, with the intent of limiting the rate of inappropriate admission, while protecting ED resources, diagnostic accuracy, and quality of treatment. The logistics of an MRI-first approach, in a non-hyperacute stroke treatment center, is yet to be evaluated; hence we aimed to test whether this implemented change in workflow yielded the intended results.
Methods
Patient population
At Copenhagen University Hospital—Herlev and Gentofte in Denmark, our neurologic ED, which is used by our non-comprehensive stroke unit, is staffed by neurologists, neurology residents, interns, and emergency nurses. All admissions have suspected acute neurological illness, both neurovascular disease and other conditions such as seizures and migraines. Thrombolysis and thrombectomy are not carried out in-house, but at the local tertiary center, and candidates of revascularization are identified prehospitally. Since January 1, 2020, we used a 12-min stroke-MRI protocol as the primary imaging technique for suspected strokes during the daytime, which included T2-fluid-attenuated inversion recovery, diffusion-weighted with apparent diffusion coefficient, and susceptibility-weighted sequences. Scans were obtained with a Philips Achieva machine with a field strength of 3.0 Tesla. MRI scans were only procurable between 8:00 AM and 6:00 PM. Simultaneously, during weekdays only, the neurologic ED staff was supplemented by a specialist stroke neurologist, with the primary task of screening suspected stroke patients and ordering their MRI when indicated. Between 6:00 PM and 8:00 AM, stroke patients were evaluated with CT, supplemented by MRI the following morning. When evaluated with MRI, transitory ischemic attack (TIA) patients with an ABCD2-score 19 ⩽3 were discharged from the ED, with outpatient follow-up, as opposed to in 2019, where they were admitted to the stroke ward (Figure 1). Only patients with suspected stroke or TIA upon admission and after a brief bedside evaluation were eligible for fast-track MRI in the ED. The logistics and referral practices related to other neurological conditions in need of inpatient MRI remained unchanged during the study period.
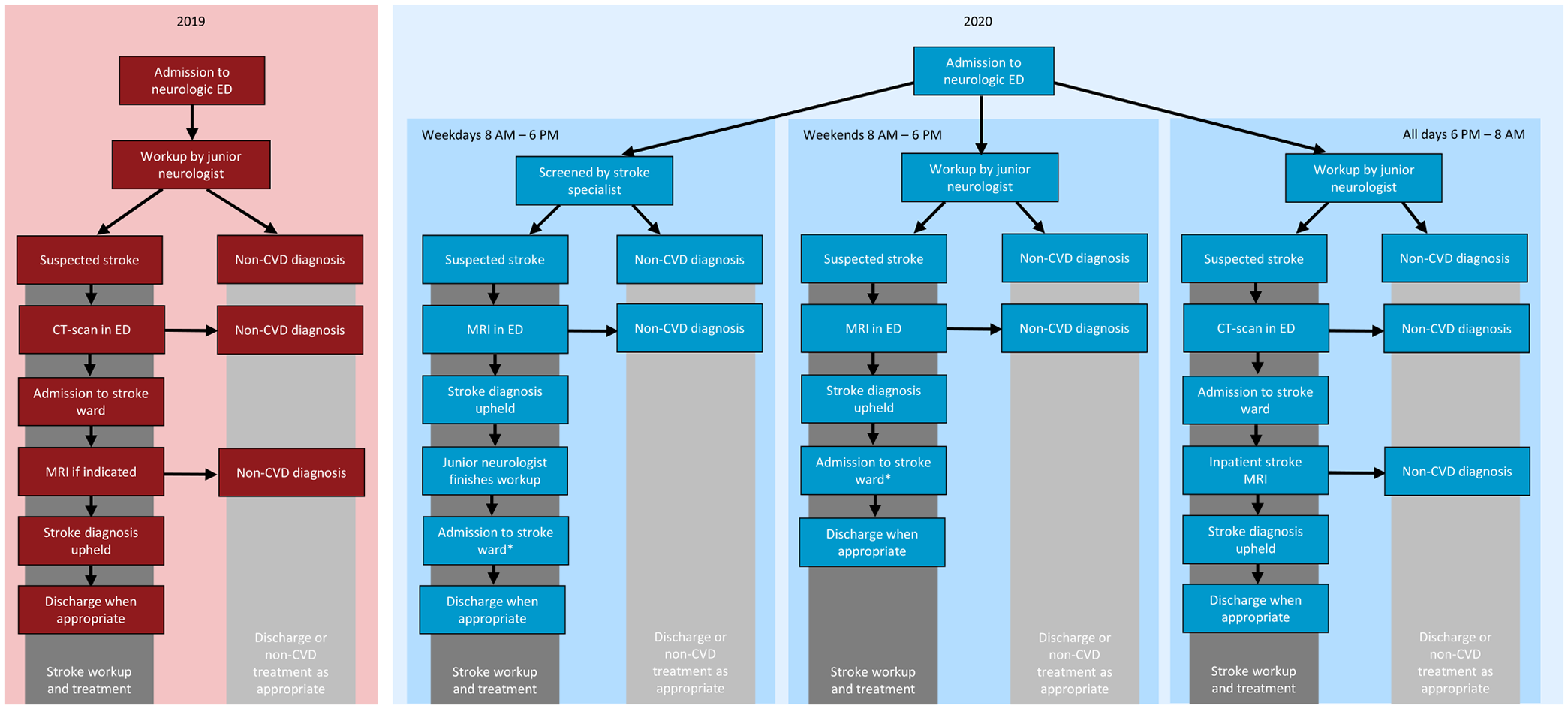
ED workflow in 2019 and 2020 at Copenhagen University Hospital—Herlev and Gentofte in Denmark. In 2019, all neurologic admissions were handled by junior neurologists, that is, interns and junior neurology residents, where patients with suspected strokes were evaluated with computed tomography upon admission, prior to transfer to the stroke ward. In 2020, during daytime, patients were screened by a frontline stroke specialist and subsequently referred to MRI in the ED if stroke was suspected. Thereafter, admitted to the stroke ward or discharged or treated for mimicking conditions, if necessary, *or discharged with outpatient workup in cases of TIA with ABCD2 ⩽3.
We included all admissions to our neurologic ED from January 1, 2020, to December 31, 2020, that is, after implementation of fast-track MRI. The time period of January 1, 2019–December 31, 2019, was used for comparison. All patients were ⩾18 years of age. Readmissions to the neurologic ED were processed as individual admissions.
Patients <18 years of age, and patients within the hospital’s catchment area who received acute initial treatment at other hospitals, were transferred directly to the wards after acute treatment, that is, not admitted via our ED. This also applies to patients who were clinically eligible for revascularization, where initial workups were carried out at the local tertiary center. Hence, candidates for revascularization were not represented in this cohort.
Outcome variables
The primary outcome was LOS in the hospital overall. Secondary outcome variables were LOS in ED, the use of inpatient MRI, rates of ED readmission, and the relative rates of strokes versus stroke mimics on the stroke ward.
Data acquisition
Initial data were automatically extracted from the local electronic health record (EHR), EPIC, and included the date and time of admission, discharge, in-hospital transfers, and MRI scan (if applicable). In addition, date of birth, sex, point of discharge (ED, stroke ward, or other), diagnosis upon discharge (ICD-10 code), and prior illnesses (ICD-10 and ATC codes). Diagnoses upon discharge were subcategorized into the following: acute ischemic stroke (AIS), TIA, intracerebral hemorrhage (ICH), other cerebrovascular disease (such as central retinal artery occlusion and spontaneous subarachnoid hemorrhage), non-cerebrovascular disease, and undetermined. Occasional patients were discharged with ambiguous diagnoses, such as “suspected stroke,” “unspecified stroke,” or “rehabilitation during admission.” Local guidelines stipulated that the latter diagnosis was used when stroke patients needed extensive inpatient physical or occupational therapy. Records with ambiguous diagnoses were reviewed and subclassified into the aforementioned categories. “Undetermined” was used in a few cases, where records were unattainable, as patients had opted out of direct access to their medical records, or if a diagnosis could not be determined (Figure 2).
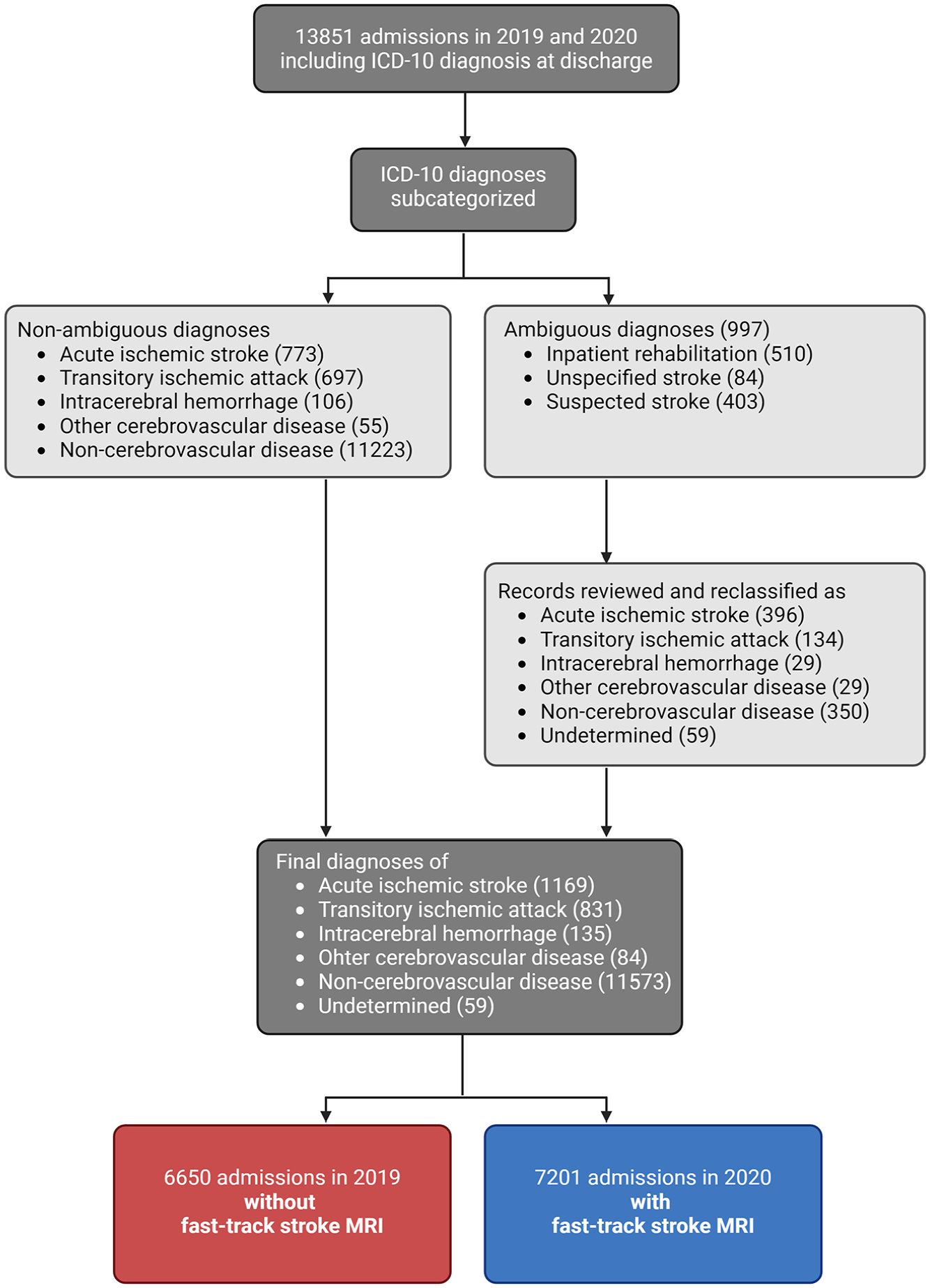
Data flow of neurologic admissions at Copenhagen University Hospital—Herlev and Gentofte in Denmark in 2019 and 2020. Diagnostic categories were acute ischemic stroke, transitory ischemic attack, intracerebral hemorrhage, other cerebrovascular disease, non-cerebrovascular disease, or undetermined.
Statistics
Continuous variables were summarized as arithmetic means with 95% confidence intervals, median with interquartile ranges, and compared with an unpaired Welch’s t-test. Categorical variables were summarized as counts with percentages and compared with Chi-square tests. In addition, we generated two subgroups. One group where TIA patients were excluded due to a change in local treatment guidelines allowing outpatient workups and one included only patients admitted within the time window, where the MRI machine was available. We used multiple logistic regression to test a dichotomized outcome variable; discharge from the hospital within 24 h, while adjusting for sex, age ⩾65 years, admissions during weekends, TIA diagnosis, comorbidities, and COVID-19 lockdown periods, that is, March 11–April 20 and December 25 to the end of the year in 2020. Comorbidities were expressed as Charlson Comorbidity Index20,21 which is described in-depth in Appendix 1. A two-sided p-value of 0.05 indicated significance. Data were managed in R version 4.4.2 (R Foundation for Statistical Computing, Vienna, Austria, https://www.r-project.org/) using packages tidyverse, dplyr, fmsb, and ggplot2.
Results
There was a total of 13,581 admissions to the neurologic ED during the study period whereof 7675 (55.4%) were women, and the average age was 61 years. Of these, 7201 were admitted in 2020 and 6550 in 2019, that is, with and without fast-track stroke MRI, respectively (Table 1, Figure 2). After the implementation of fast-track stroke MRI in ED, the mean LOS changed from 56.0 to 38.6 h in the hospital (Table 1, Figure 3). The reduction in LOS was driven by an increased rate of short admissions, as the rate of discharge within 24 h increased from 51.4% to 64.0% of ED admissions (Table 1, Figure 3). The significant difference in LOS persisted when TIA patients were excluded. There was a slight yet significant reduction in mean LOS in ED after implementation of fast-track MRI, from 9.17 to 8.63 h (Table 1), which persisted also among patients admitted between 8:00 AM and 6:00 PM, where the MRI machine was accessible.
Cohort characteristics of neurologic admissions in 2019 and 2020, at Copenhagen University Hospital—Herlev and Gentofte in Denmark.

Admissions in 2019 were without access to fast-track MRI and in 2020 with fast-track MRI in the ED. A subgroup where patients with transitory ischemic attacks are excluded is shown, as local treatment guidelines changed during the study period. A subgroup including only admissions within the time window where the MRI machine was accessible* is also shown. Diagnoses were based on ICD-10 codes and subcategorized into acute ischemic stroke, transitory ischemic attach, ICH, other cerebrovascular disease, non-cerebrovascular disease, and undetermined.
CI, confidence interval; ED, emergency department; ICH, intracerebral hemorrhage; IQR, interquartile range; MRI, magnetic resonance imaging.

Histogram shows the distribution of hospitalization lengths of neurologic admissions at Copenhagen University Hospital—Herlev and Gentofte in Denmark in 2019 and 2020. Fast-track MRI was accessible in 2020, and 2019 was used as a control.
There was a small, albeit significant reduction in the rate of ED admissions that were transferred to the stroke ward, from 23.3% to 20.9% (Table 1). The rate of stroke mimics on the ward did not change significantly. However, the rate of patients with ischemic strokes increased slightly but significantly, increasingly so in the subgroup where only daytime admissions, where MRIs were procurable, were included (Table 1). Typical stroke mimics were dizziness, migraines or other headaches, relapse or worsening of chronic neurologic deficits (e.g., due to infection), altered mental state, or other unspecified neurologic symptoms.
The number of ICH diagnoses in the ED decreased from 80 in 2019 to 55 in 2020. However, the ICD-10 code of “unspecified intracerebral hematoma” was used for both traumatic hemorrhages and hemorrhagic strokes. Only the latter were admitted to the stroke ward, where the rate of ICH remained unchanged.
The use of inpatient stroke MRI increased significantly, from 23.8% to 39.6% of all neurologic ED admissions, after MRI access was fast-tracked. The 30-day readmission rate to the general ED remained unchanged. There was no significant change in the relative rates of AIS and TIA diagnoses among ED admissions overall, apart from ICH which increased, as mentioned previously (Table 1).
After adjusting for sex, age, weekend admissions, pandemic lockdown periods, and TIA diagnosis, the odds of discharge within 24 h were significantly greater after the implementation of fast-track MRI in ED. Faster discharge was also seen for females and younger individuals. Weekend admissions (which excludes frontline stroke specialists) and lockdown periods did not significantly associate with discharge within 24 h (Table 2).
Estimates from adjusted analysis of discharge from hospital within 24 h of neurologic admissions at Copenhagen University Hospital—Herlev and Gentofte in Denmark, in 2019 and 2020.

Multiple logistic regression plotting association of MRI accessibility, sex, age, admission during weekends, pandemic lockdown periods, and TIA diagnoses with discharge from hospital within 24 h. Includes all neurologic ED admissions. Fast-track MRI was accessible in 2020 and was not yet implemented in 2019.
Frontline stroke specialists were unavailable during weekends.
CI, confidence interval; ED, emergency department; MRI, magnetic resonance imaging; TIA, transitory ischemic attack.
Discussion
This retrospective study indicates an association between the implementation of fast-track MRI in a neurologic ED for suspected strokes and reduced LOS, both in-hospital and ED. The use of inpatient MRI increased as expected, 10 whereas the rate of admissions to the stroke ward decreased. To our knowledge, this is the first evaluation of the interplay of MRI-first and hospital logistics, in a non-comprehensive stroke center where hyperacute treatment such as thrombolysis is not carried out.
A strength of this study is the large original cohort. The cohort is consecutive which should reduce the risk of inherent bias. We have adjusted for known potential confounders, such as comorbidities, altered treatment guidelines for TIA patients, 19 and lockdown periods.22,23 In addition, the bulk of data was recorded real time during admissions and extracted automatically from the local EHR, with a low risk of reporting bias. Although MRI-first was reserved for suspected stroke, we opted to include all admissions to the neurologic ED in the cohort. This also includes conditions where brain MRI was irrelevant. In addition, reasons for referral to ED were often nonspecific, such as “weakness” as opposed to “suspected stroke.” Ultimately, the suspicion of stroke, thus the need for MRI, was determined by the on-call physician in the neurologic ED, during admission. Hence, the exclusion of conditions where brain MRI was unnecessary would entail a risk of selection bias.
A limitation of this study is its retrospective design, in which the risk of residual confounding cannot be eliminated, although statistical adjustment was done. Notwithstanding, reduced hospital resources 24 and the local absence of frontline stroke specialists during weekends, weekend admissions did not associate with altered LOS. Despite the simultaneous implementation of both frontline stroke specialists and MRI-first (Figure 1), the association between fast-track MRI and short admissions remained after adjusting for these staff-related variations.
The COVID-19 pandemic is another potential confounder, present only after the implementation of fast-track MRI, where the strain on EDs and hospitals increased. 23 Yet, the association between short admissions and MRI access remained after adjustment for Danish lockdown periods. In general, Danish stroke admission rates remained unchanged during the pandemic besides a small decrease during the first lockdown period 25 for which we have adjusted. However, we do not expect that this adjustment is sufficient to account for all pandemic-related influences on this study.
Our results could also be influenced by the TIA-related change in local treatment guidelines, where low ABCD2 scores19,26 entailed outpatient workups. However, the association between fast-track MRI and short admissions remained, after both the exclusion of (Table 1) and adjusting for TIA patients (Table 2).
The diagnostic categories used in our study were primarily based on ICD-10 codes assigned by the treating physician at discharge, which is deemed reliable. 27 However, in 997 (7.2%) of cases the ICD-10 codes were potentially ambiguous and were reviewed for clarification, whereof a mere 59 of these could not be reclassified. Reporting bias cannot be eliminated during this process.
Additional factors that could have been accounted for include incompletion of MRI, for example, due to claustrophobia 8 and stroke severity. Unfortunately, these data were unavailable.
The observed reduction in LOS in hospitals after the implementation of fast-track MRI in ED is in concordance with previous studies.10–14 Although there are well-documented advantages of short hospitalizations, when possible,17,18 we have not tested whether the patients in our cohort have reaped this type of benefits. Nor can we fully establish whether the shortened admissions potentially cause adversity. 28 However, the rate of readmission within 30 days remained unchanged at 1 in 10 patients. Contrary to previous studies, where the time spent in the ED increased, 10 we observed a slight but significantly decreased LOS in ED after implementation of MRI-first for suspected stroke, also when only including patients admitted during daytime, when the MRI machine was accessible. This was potentially attributable to the fast-tracked logistics of the implemented approach.
The rate of mimics admitted to the stroke ward was unchanged. This differed from previous studies, in which rates of admitted stroke mimic decreased when MRI in ED became available.10,11 Our result is potentially attributable to the clinical nature of stroke diagnostics, a bedside process.29,30 Contrarily, in cases of atypical symptoms of stroke, early MRI may facilitate stroke identification 31 causing an increased rate of true strokes on the ward. However, previous studies indicate mimic rates of 30%–50% among admissions with suspected stroke,29,32 analogous to our rate of 44.6%.
Globally, ICH makes up approximately 13% of all strokes. 1 The rate of ICH in our cohort was lower (approximately 7.5%), in both 2019 and 2020. This could be attributed to the national guidelines and the local setup. Eligibility for potential revascularization is identified by emergency medical services prehospitally based on symptom reporting, clinical examination, and stroke severity, prior to imaging. Patients with hemorrhagic strokes often have more severe symptoms with higher National Institutes of Health Stroke Scale at onset, than patients with ischemia. 33 Workups preceding potential revascularization were carried out at the local tertiary center. After thrombolysis or thrombectomy, or in cases where the workup at the comprehensive center reveals a contraindication thereof (such as ICH), these stroke patients within our hospital’s catchment area, would be transferred directly to our stroke ward, hence bypassing our ED. Due to the latter, they are not represented in our cohort, which potentially explains our relatively low rate of hemorrhagic stroke.
The use of inpatient MRI expectedly increased when access was facilitated in the ED. 10 We did not measure whether this augmented the rate of outpatient MRI scans. Nevertheless, although MRI-first has been shown to increase physicians’ confidence during clinical reasoning, 6 thresholds for referral to MRI could potentially be lowered, when access to imaging is facilitated.34,35 Incidental findings on brain MRI are not uncommon, 36 rendering potential defensive decision-making behind referral practices relevant, 35 yet out of scope for this study.
After completion of this study, MRI-first is now permanently implemented in a collaborative effort between clinical neurology and neuroradiology, to facilitate stroke diagnostics in the ED at our hospital. The findings of this study indicate improved ED workflow and diagnostic precision, which resonates with the real-life experiences of the on-call staff in both clinical neurology and neuroradiology, warranting the permanency of MR-first.
Conclusion
Implementation of fast-track MRI for suspected stroke in a non-comprehensive setting is associated with reduced lengths of hospitalizations overall. Our results demonstrate that a diagnostically superior MRI-first approach for suspected stroke is feasible as a fast-track concept in the ED.
Footnotes
Appendix 1. Charlson Comorbidity Index
Categories based on Glasheen et al. 21

| Condition number | Condition | ICD-10 code | ATC code |
|---|---|---|---|
|
|
Myocardial infarction | DI21 DI22a,1 DI23a,1 DI24a,1 DI25a,1 |
B01AC06
a
B01AC24 a B01AC07 a |
|
|
Congestive heart failure | DI50 DI110 DI130 DI132 DI255 DI42 DP29 |
|
|
|
Peripheral vascular disease | DI70 |
|
|
|
Cerebrovascular disease | DG45 (excluding DG4542,b) |
|
|
|
Dementia | DF00 |
|
|
|
Chronic pulmonary disease | DJ40–DJ47 |
R03 a |
|
|
Rheumatic disease | DM05 |
|
|
|
Peptic ulcer disease | DK25 |
|
|
|
Liver disease, mild | DB18 |
|
|
|
Diabetes without chronic complications | DE10 |
|
|
|
Renal disease, mild to moderate | DI129 |
|
|
|
Diabetes with chronic complications | DE100–DE108 |
|
|
|
Hemiplegia or paraplegia | DG81 |
|
|
|
Any malignancy | DC00–DC99 | |
|
|
Liver disease, moderate to severe | DK704 |
|
|
|
Renal disease, severe | DN185 |
|
|
|
HIV infection, no AIDS | DB20 |
|
|
|
Metastatic solid tumor | DC77 |
|
|
|
AIDS | DB24 |
Weight categories based on Charlson et al. 20
Added due to local practices, with the use of synonymous ICD-10 codes.
Excluded due to benign and non-stroke nature of transitory global amnesia. 37
Additions to category.
Removals from category.
Acknowledgements
We are grateful to Line Lunde Larsen for support and commitment during the implementation of fast-track stroke MRI, and our dedicated co-workers who cared for the patients in our study.