
Abstract
Background:
Neurosarcoidosis is a rare manifestation of sarcoidosis with heterogeneous presentations. Patient management is challenging due to the current lack of knowledge about the long-term disease course.
Objective:
To identify specific disease courses of neurosarcoidosis according to the clinical and paraclinical presentations at onset.
Methods:
We conducted an observational multicenter cohort study by retrospectively collecting data from the medical records of 84 patients diagnosed with definite, probable, or possible neurosarcoidosis in three tertiary referral centers in France (Nancy, Strasbourg, and Bordeaux). We collected demographic characteristics, clinical and paraclinical data at the beginning of patient management, and during follow-up under the different treatment lines. Two expert neurologists determined disease course profiles.
Results:
The mean follow-up was 6.6 years. Almost every patient (96.4%) received steroids at some point of their follow-up. Tumor Necrosis Factor-alpha blockers were given in 10.7% as first-line treatment and in 33.3% during follow-up. Every patient presented with a relapsing disease, often monophasic (75%) and sometimes polyphasic with the recurrence of identical manifestations (11.9%). Patients developing new neurological symptoms during follow-up were a minority (13.1%). No patients exhibited a progressive course. Patients with isolated cranial nerves injury or aseptic meningitis always exhibited a monophasic course, and 62.5–75% of them had a full recovery after first-line treatments. This proportion was 15.6% in other forms of the disease. Those with peripheral presentations were more likely to present a polyphasic course than patients with other forms of neurosarcoidosis. Spinal cord presentations were monophasic, but resulted in sequelae and exhibited poor response to first-line treatments despite frequent use of TNF-alpha blockers.
Conclusion:
Identification of these disease course profiles, based on the initial clinical and paraclinical presentation, could guide the clinician to select the optimal therapeutic approach and follow-up modalities for their patients with neurosarcoidosis.
Introduction
Sarcoidosis is a multi-systemic granulomatous inflammatory disease with an estimated prevalence of between 10 and 20 per 100,000.1–3 Neurosarcoidosis (NS) is one of the many forms of the disease and occurs in 5–20% of patients with sarcoidosis. 4 Diagnostic criteria were described by Zajicek et al. in 1998 and have been modified since then. The current version from the Neurosarcoidosis Consortium Consensus Group 5 classifies the diagnosis as ‘definite’ when confirmed by a nervous system biopsy, ‘probable’ when granulomas are present in extraneural tissue, or ‘possible’ in the absence of histological evidence but with a presentation consistent with NS.
Many empirical cohort studies and reviews have addressed the question of the different clinico-radiological patterns of NS, mainly based on the anatomic location of the lesions. Magnetic resonance imaging (MRI) and cerebrospinal fluid (CSF) analysis illustrate central nervous system (CNS) injury which consists of meningeal involvement, cranial neuropathies, brain parenchymal disease, or spinal cord involvement in more than 30% of cases. Other injuries may involve the peripheral nervous system (PNS), the hypothalamic/pituitary axis, and the ventricles (hydrocephaly).
However, these descriptions are based on cross-sectional data, that is, representative of symptoms at a single time-point of a patient’s disease, and few publications describe the longitudinal course of NS. Furthermore, different terms have been used to characterize the patterns of the course of NS, such as ‘improvement/stable disease/progression’, 6 ‘monofocal/relapsing/progressive disease’, 7 or a mix of these different terms.8–10 Finally, these classifications are mainly subjective, often based on short follow-up durations, and in specific subgroups of patients (e.g. patients with spinal cord involvement).
Another important issue is that epidemiological studies must consider the patients’ treatment. Corticosteroids are usually used as first-line treatment for NS,4,11 and unselective immunosuppressive treatments such as methotrexate, azathioprine, or mycophenolate mofetil are used as steroid-sparing treatment or for second-line treatment.4,12,13 However, treatment strategies vary from one region of the world to another, and from one treating physician to another as no official guidelines exist. The earliest publications of NS were small series of cases.14,15 Following articles addressed cohorts of patients mainly receiving steroids or immunosuppressant drugs.4,10,16–20 More recently, a number of studies have reported the effectiveness of tumor necrosis factor-alpha (TNF-alpha) blockers, mainly infliximab.18,21–24
The objective of our study was to identify specific disease courses of NS using the longitudinal data of patients from three French tertiary centers for inflammatory diseases of the nervous system. We describe these patterns according to the clinical and paraclinical presentations at onset, and took into consideration the use of different lines of treatment during follow-up.
Methods
Patients
We retrospectively studied the medical records of 84 patients from three tertiary neurological centers in France: the University Hospitals of Nancy (North-Eastern France), Strasbourg (North-Eastern France), and Bordeaux (South-Western France). All the patients were identified from databases updated by the treating neurologists and had been diagnosed with definite, probable, or possible NS according to the Neurosarcoidosis Consortium Consensus Group. 5 We included every patient seen at least once between 1 January 2000 and 31 December 2019.
Patients with missing data in their medical records, and those who had not authorized the use of their medical data for research purposes, were not included.
We collected data concerning demographics, clinical presentation, and especially neurological examination at onset and throughout available follow-up. Laboratory results were also collected, when available, as were data about patients’ disease modifying treatments (DMTs). Data collection was continued up to January 2021 from the patients’ records on site by a single person.
We present the data as descriptive statistics. Results are expressed as percentages (qualitative data) or mean ± standard deviation (quantitative).
Definitions
We defined seven patterns of onset based on the initial presentation, that is, at the time of the very first symptoms of NS. These patterns were based on data from interrogatory, clinical examination by the neurologist, and CSF and imaging findings. One neurologist (IB) grouped symptoms and findings to define the patterns based on their own choice and knowledge. In case of uncertainty, a second neurologist (GM) adjudicated.
The seven patterns are as follows:
‘Encephalic’: Patients presenting with symptoms and imaging findings compatible with involvement of the encephalon, without involvement of spinal cord or PNS. Cranial nerves could be involved.
‘Spinal cord’: Patients presenting with symptoms and imaging findings compatible with involvement of the spinal cord (intramedullary or leptomeningeal lesions on MRI), without encephalic or PNS involvement.
‘Encephalic and spinal cord’: Patients presenting with symptoms and imaging findings compatible with involvement of both the brain and the spinal cord, as previously described, without involvement of the PNS.
‘Cranial nerves (isolated)’: Patients presenting with involvement of one or several cranial nerves, with no other symptoms, and without encephalic or spinal cord lesions, or PNS involvement. Brain MRI is normal or reveals cranial nerve or leptomeningeal enhancement.
‘Peripheral nervous system’: Patients presenting with symptoms and electroneuromyography compatible with involvement of the PNS (peripheral nerves and/or muscles), isolated: without involvement of encephalon or spinal cord. Patients with cranial nerve involvement were included in this group.
‘Central and peripheral nervous system’: Patients with both PNS (peripheral nerve and/or muscle) and CNS (encephalon or spinal cord) involvement, as previously described.
‘Aseptic meningitis’: Patients in whom a cellular reaction is detected on analysis of the CSF, without an identified germ, and with normal imaging (or isolated leptomeningeal enhancement).
DMTs were categorized as follows:
‘First-line treatment’ corresponds to the first treatment introduced, regardless of its type. It could be corticosteroids alone or corticosteroids in combination with an immunosuppressant treatment started at the same time mainly as a steroid-sparing therapy.
Further lines (‘second-line’, ‘third-line’, etc.) were either add-on therapies or were used after a switch from the previous DMT. In some cases, these treatments could be used as a steroid-sparing strategy when the previous line consisted of corticosteroids alone, but they were generally introduced to escalate efficacy.
After the initial presentation and the introduction of the first-line DMT, the NS course was evaluated by changes in clinical and paraclinical data by one experienced neurologist (IB) who carefully reviewed all the files and took into account all available clinical and imaging data. A second neurologist (GM) adjudicated in case of uncertainty. The choice of tests and the time they were scheduled were not standardized. According to the evaluation scheduling, three different components of the disease course were identified.
The short-term course corresponded to the initial response to treatment, and was categorized as: ‘full recovery, partial improvement, stabilization (no improvement)’, and immediate worsening. These categories were determined a priori. They correspond to the whole spectrum of response to treatment of any medical condition.
After the initial response, the occurrence of a new event months or years after the initial presentation corresponded to the ‘disease course’, that is, mid-/long-term course. This component of the NS course constitutes the most original aspect of our study. The categories were established prospectively according to each patient’s history, without any preconceived ideas. We used all clinical and paraclinical data at our disposal, including imaging data, to classify the patients.
Finally, at the end of follow-up, persistence of neurological symptoms was considered as ‘sequelae’ (classified as ‘present/absent’). This last category was totally based on clinical data.
Results
The patients’ characteristics are provided in Table 1. Of the 84 patients, 46 (55%) were male. The mean follow-up from the onset of neurological symptoms was 6.6 years, with 81% of the patients followed for more than 2 years, and 63% for more than 4 years. Numerous tests were performed to confirm the diagnosis of NS. Chest computed tomography was performed in almost all the patients, and was positive in over three quarters of them. A biopsy of neural tissue was performed in 26 patients, and was contributive for 22. Overall, the mortality rate was 4.8% (4/84 patients). One patient died because of sepsis (while on infliximab for 5 months). Three other patients died of unknown reasons, one while on infliximab for 6 months, one on methotrexate for 36 months, and the last one without precision about his treatment at the time of his death.
Patient characteristics.

Presentation at onset
As shown in Table 2, the most common presentation at onset in this cohort was represented by the ‘encephalic’ group with the most common symptom being encephalopathy (55.6%), followed by focal or generalized epileptic seizures (51.9%). Other symptoms – focal deficit, cerebellar syndrome, cranial nerve palsy – were less frequent. None of the patients had any isolated dural involvement, nor hydrocephalus. Brain MRI showed abnormalities in all the patients. Parenchymal T2 hyperintensities were found in 88.9% of the patients with gadolinium enhancement in 55.6%. Leptomeningeal enhancement was found in 48.2% and a pachymeningitis in two patients (7.4%).
Initial type of presentation, n (%).
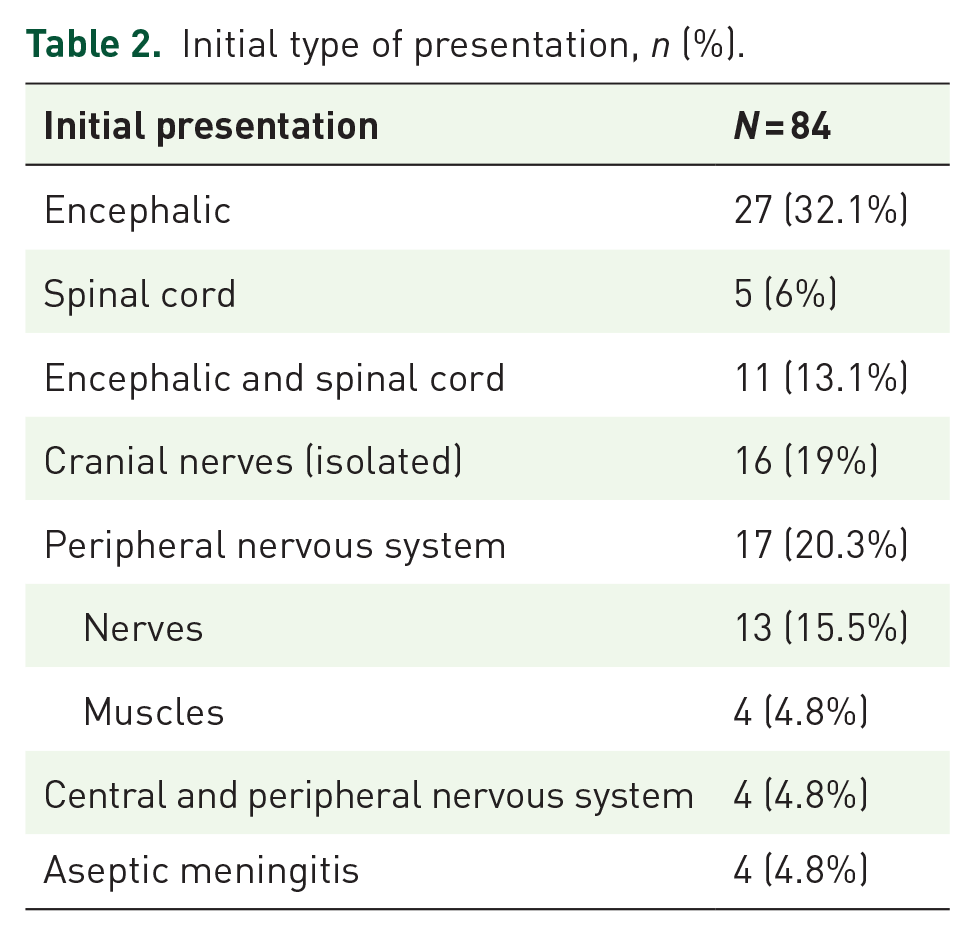
Isolated spinal cord involvement was found in five patients (6.0%). Symptoms included sensory disorders in all of these patients, motor deficit in four, and sphincter impairment in three. In the whole cohort, when not isolated, the spinal cord was involved in 17 patients (20.2%).
Overall, 33.3% of the patients presented with cranial nerve palsy, and this syndrome was clinically isolated in 19.0%. The facial nerve (VII) was the most frequently involved nerve in the ‘cranial nerve’ group (observed in 56.3% of the patients). The optic nerve (II) was affected in only two patients (6.3%).
Four patients belonged to the ‘CNS and PNS’ group. CNS damage consisted of a spinal cord lesion for one patient, and encephalic involvement for the three others. PNS involvement was highlighted by electroneuromyography and consisted of sensory-motor polyneuropathy in two patients: mononeuritis multiplex in one, and polyradiculitis in the other.
Isolated aseptic meningitis was found in four patients (4.8%), with lumbar puncture showing elevated white cell counts in 100% (mean 122/mm3), and elevated protein levels in 60.0% (mean 0.86 g/L).
The presence or absence of extra-neurological symptoms was indicated in the medical file for 72 patients. Twenty-five had such symptoms (34.7%). Asthenia was found in 14 (19.4%), weight loss in 9 (12.5%), dyspnea in 7 (9.7%), dry eyes and/or mouth in 4 (5.6%), lymphadenopathies in 3 (4.2%), uveitis in 3 (4.2%), arthralgia in 2 (2.8%), cutaneous nodules in 2 (2.8%), and parotiditis in 1 (1.4%).
Treatments
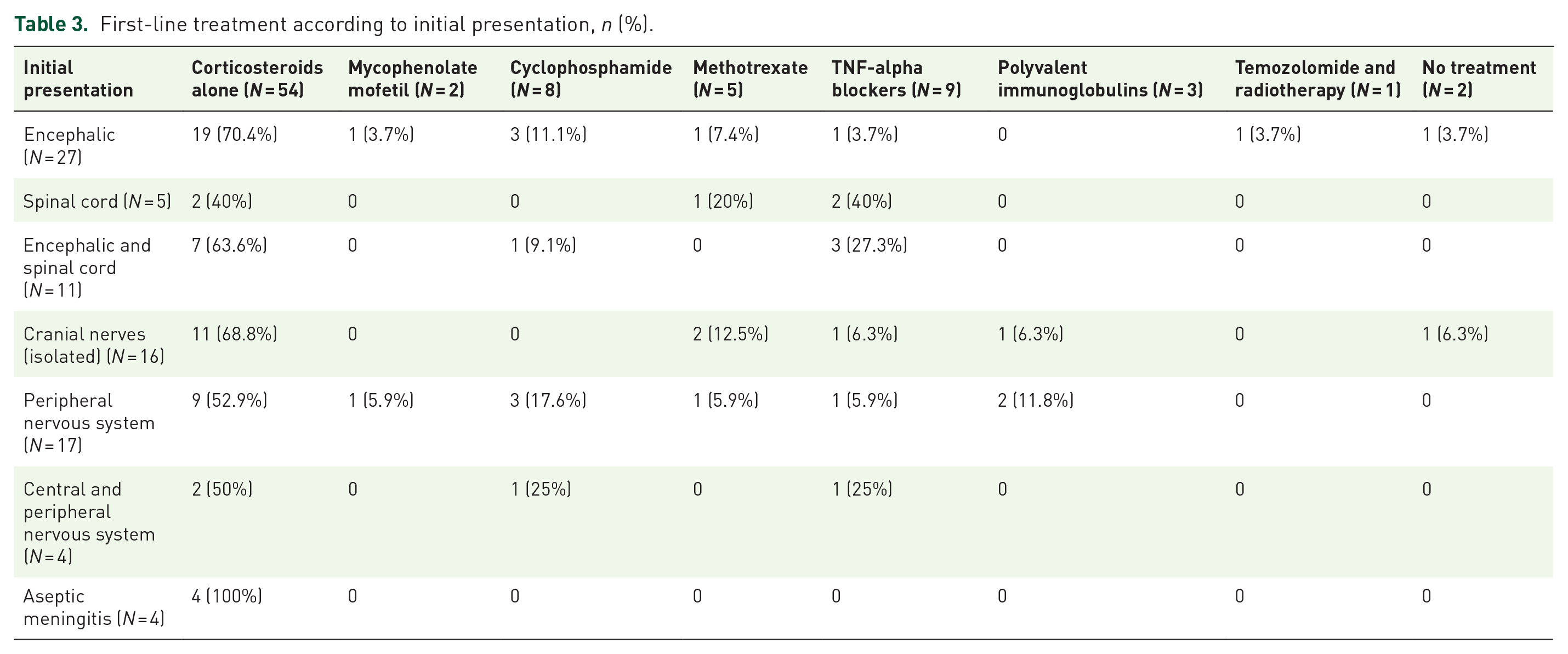
All the patients except two received at least one line of treatment. As shown in Figure 1, the most used first-line treatment was oral corticosteroids, sometimes after intravenous bolus, and used alone in 54 patients (64.3%). Nonetheless, 96.4% of our patients received corticosteroids at some point in their treatment, either alone or combined with other therapies, and in particular when a steroid-sparing strategy was needed. Corticosteroids were usually tapered off gradually, with the maintenance dose determined on a case-by-case basis, and often maintained for months or even years, sometimes for the whole care period. Subsequent dose increase alone was not considered as a new line of treatment. Other types of treatments were possible, even as first-line DMTs, but often combined with corticosteroids. Table 3 presents the type of first-line DMT according to the initial presentation. Corticosteroids alone were used in the majority of cases for any presentation, but the use of immunosuppressant drugs, even TNF-alpha blockers as a first-line treatment was not uncommon: used in nine patients (10.7%). In contrast, all the patients with aseptic meningitis received corticosteroids alone as first-line treatment.

Repartition of first-line disease modifying treatments used in the cohort of 84 patients with neurosarcoidosis.
First-line treatment according to initial presentation, n (%).
Thirty-two patients (38.1%) received a second-line treatment. These patients had a mean duration of follow-up of 6.1 years. Twelve patients (14.3%) also had a third-line treatment (mean duration of follow-up of 7.4 years), seven (8.3%) a fourth-line treatment (mean duration of follow-up of 6.2 years), and three (3.6%) a fifth-line treatment (mean duration of follow-up of 10.2 years). Finally, one patient (1.2%), with a follow-up of 27.5 years, required six lines of treatment. Patients who received only one line of treatment had a mean duration of follow-up of 5.6 years. At the end of follow-up: 57 patients (67.9%) were still on-treatment.
The drugs most frequently used after first-line treatment were TNF-alpha blockers (usually combined with corticosteroids) administered to 33.3% of the patients. Methotrexate was administered to 25% of the patients and mycophenolate mofetil to 23.8%. Cyclophosphamide was used in 9.5% of the cases, and corticosteroids, which was by far the most prescribed treatment in first line, was only given alone in 4.6% of the patients on subsequent lines of treatment. One patient received immunoglobulins, one hydroxychloroquine, and one rituximab.
Disease course
Initial response
After the first clinical event, the early course of the disease was considered as the initial response to first-line DMTs, as 82 patients of the 84 were treated. Twenty-three patients (27.4%) presented full neurological recovery, 24 (28.6%) partial improvement, 13 (15.5%) presented stabilization of their clinic-radiological state, and 24 (28.6%) worsened. Table 4 summarizes these responses according to each disease course. An initial presentation limited to the cranial nerves or aseptic meningitis had the highest proportions of patients with full recovery (62.5% and 75.0%, respectively), while patients with encephalic and/or spinal cord injury had a lower rate of full or partial recovery in comparison with stabilization or worsening after the first treatment. After the exclusion of patients with these two favorable forms of NS, 10 patients out of 64 (15.6%) benefited from full neurological recovery, 22 (34.4%) had partial improvement, 12 (18.8%) stabilization, and 20 (31.3%) worsening.
Response to first-line treatment according to initial presentation, n (%).

Disease course
As illustrated in Figure 2, we identified three different courses during follow-up: monophasic, polyphasic with recurrence of the same symptoms, and polyphasic with different neurological symptoms.
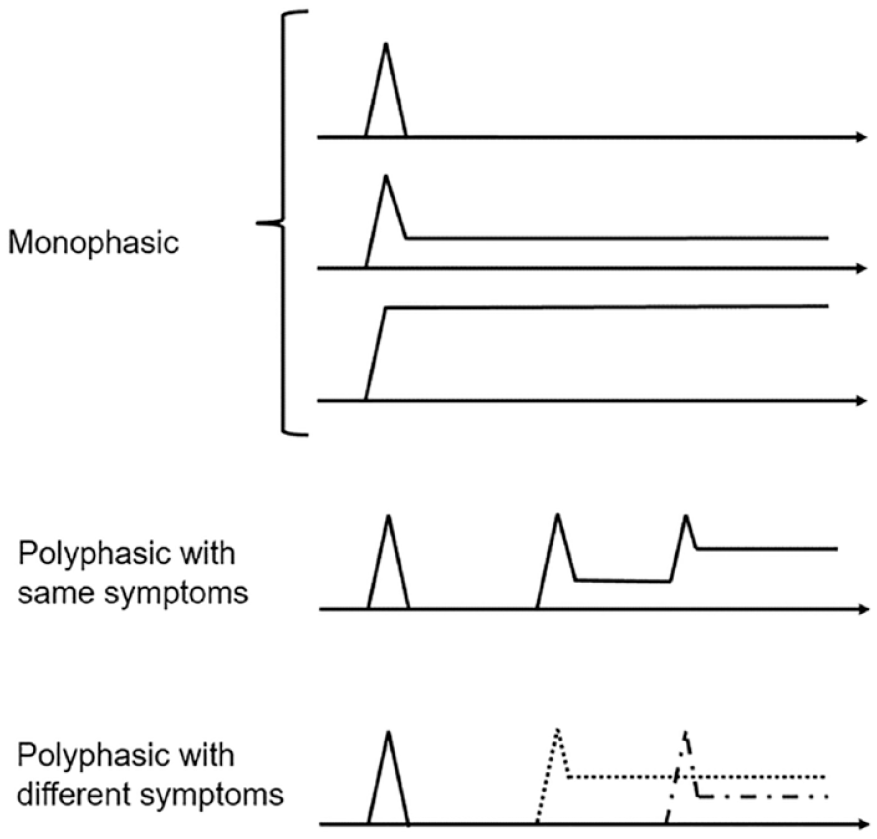
Description of different types of disease courses in the cohort of 84 patients with neurosarcoidosis.
Patients were considered as presenting with a ‘monophasic’ course when they did not present any other symptoms than the initial ones, either with sequelae or not, but without acute recurrence of these symptoms. This pattern of NS might therefore be seen as a single relapse with resolution of the symptoms after a highly variable interval, or without resolution. Most of the patients were in this group (63, 75%), with a duration of follow-up of 5.9 years (SD 5.0).
In contrast, the ‘polyphasic with the same symptoms’ group consisted of patients whose initial symptoms may have improved, totally or partially, but who had further episodes of sustained worsening of these same symptoms, without the appearance of other types of symptoms. Patients improving after treatment initiation and who further worsened during tapering belonged to this group. Ten patients (11.9%) were in this group, with a mean follow-up of 7.4 years (SD 3.8).
Finally, the third group was ‘polyphasic with different neurological symptoms’, consisting of patients who presented with episodes of worsening, either with initial improvement or not, and new neurological symptoms which were different from the initial presentation. These new symptoms may or may not improve afterwards. The 11 patients (13.1%) of this group had a follow-up of 10.5 years (SD 7.0).
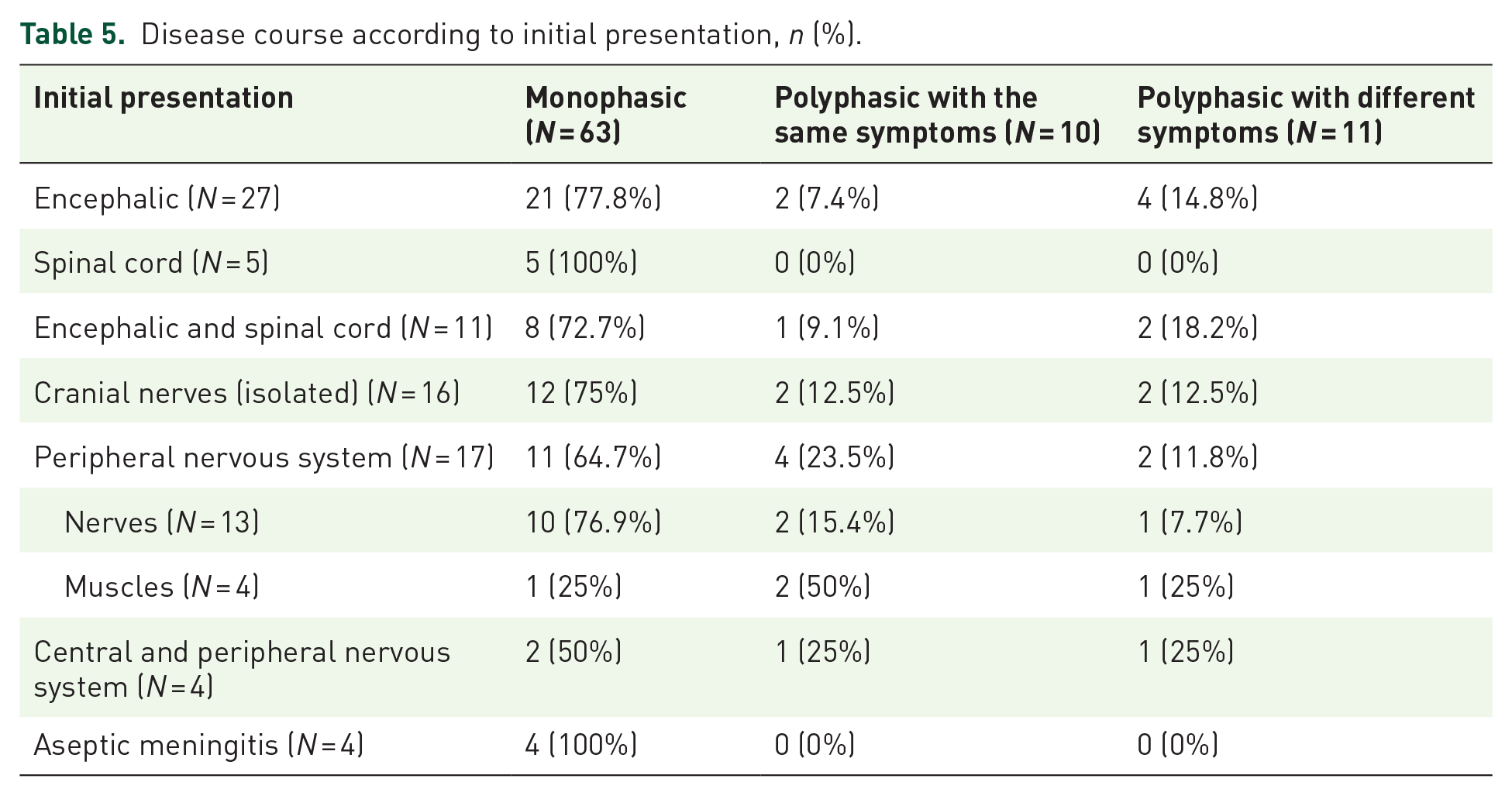
We studied the proportions of these three specific disease courses according to the type of initial presentation (Table 5).
Disease course according to initial presentation, n (%).
Overall, there was a fairly homogenous clinical and paraclinical course (mainly imaging findings) in our patients. A clinical worsening was almost systematically correlated with a paraclinical worsening. However, some patients presented a worsening on imaging findings without clinical impact. In these cases, the course was considered as polyphasic even if the clinical findings were stable.
Sequelae
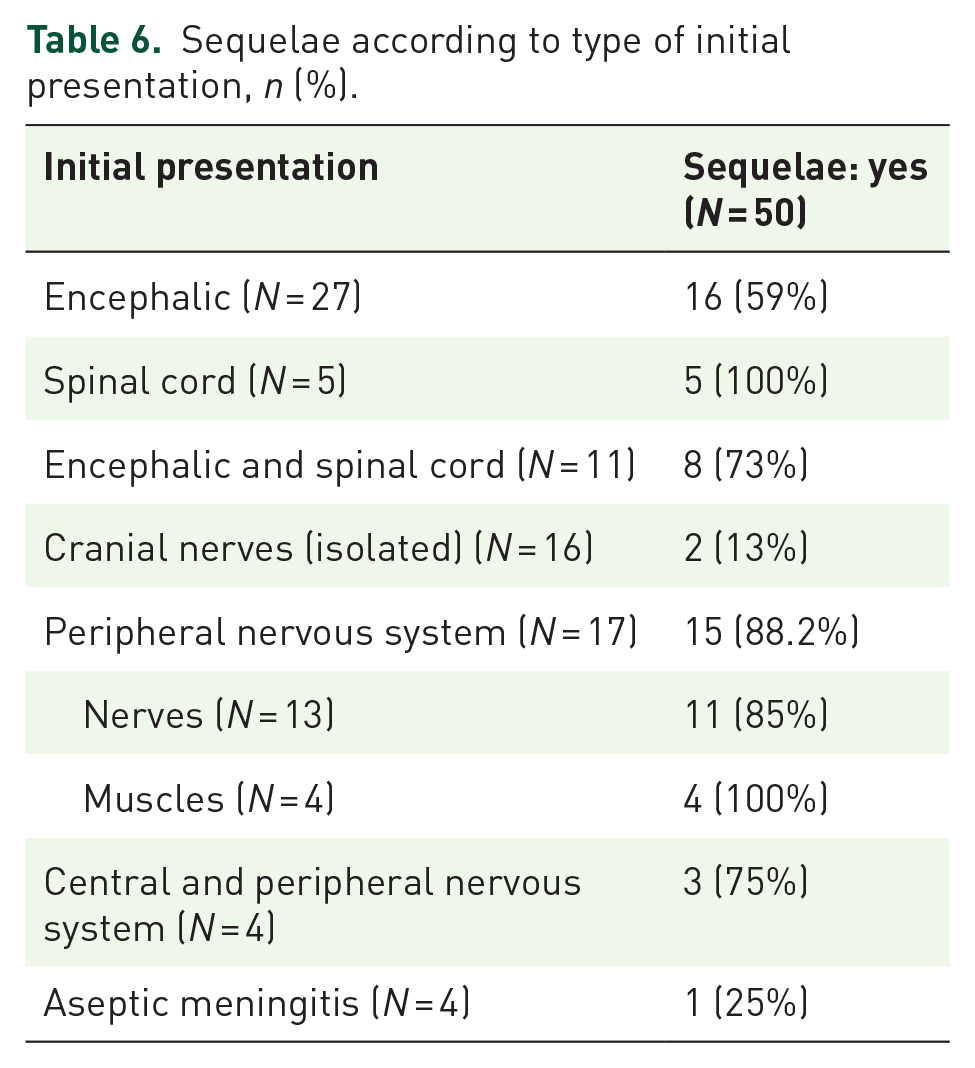
As shown in Table 6, at the end of follow-up, more than half of the patients (59.5%) presented sequelae. All the patients in the ‘isolated spinal cord’ group and the ‘PNS with muscle involvement’ group, had sequelae. The ‘cranial nerve’ and ‘aseptic meningitis’ groups had the fewest sequelae with 13% and 25%, respectively.
Sequelae according to type of initial presentation, n (%).
Discussion
Our analysis of the medical records of 84 patients presenting with NS with a mean follow-up of 6.6 years, identified specific disease courses according to clinical and paraclinical presentation at onset and DMTs. This is one of the biggest cohorts of patients with NS and one of the longest follow-up to be described.6,10,16,25–28 We identified three major points: (1) NS is clearly a relapsing disease. No patient presented with a progressive disease, even after many years of follow-up. (2) Patients had mostly a single episode or a recurrence of episodes with the same symptomatology. Patients developing new symptoms during disease course were a minority. (3) We confirm that patients with aseptic meningitis or isolated cranial nerves involvement not only had a good short-term prognosis with 62–75% of full recovery after the first-line treatments, but also had more frequently a monophasic course and had less sequelae at the end of follow-up in comparison with other forms of NS.
We identified three disease courses: monophasic, polyphasic with recurrence of the same symptoms, and polyphasic with the occurrence of different neurological symptoms. While the definition of these categories might appear subjective, we used terms and definitions widely used in chronic diseases. For example, the multiple sclerosis spectrum contains clinically isolated syndromes (equivalent to monophasic) and relapsing-remitting forms (polyphasic). These categories have also been used to describe acute demyelinating encephalomyelitis and neuromyelitis optica spectrum disorders. 29 We did not identify ‘progressive’ or ‘secondary progressive’ forms in the course of NS in our cohort, even though these terms have been used in other studies, drawing once again an analogy with multiple sclerosis.6,9 In this pathology, progression is defined as a steadily and definitive worsening of disability, independent of attacks, and basically viewed as the consequence of neurodegeneration and chronic demyelination.30,31 We did not observe this pattern in our patients. However, our study did not include cognitive tests, which could have identified progressive cognitive deterioration, as described in multiple sclerosis.32,33 It should be noted that we defined these disease courses exclusively according to neurological symptoms and complementary exams: extra-neurological manifestations and their own course were not taken into account, as it was not part of our objective.
In addition, the definition of the disease courses is not independent of other confounding factors such as DMTs. For example: a patient improving after a full dose of corticosteroids could then worsen when the steroids where tapered. This patient would then be classified in the ‘polyphasic with recurrence of the same symptoms’ profile. The same patient, without treatment could have had a monophasic course, with the same lesion and same symptoms remaining stable over time. We adjudicated this way, because DMTs are supposed to modify the disease course at the physiopathological level. Thus, a recurrence of the initial symptoms after an improvement probably means an immunological flare-up in the nervous system, that is, a new relapse of NS. On the contrary, the onset of new neurological symptoms over follow-up is proof of an expansion of the original lesions, that is, a worsening disease. This was the case for 11 of our 84 patients, a relatively low proportion (13.1%). All the other patients presented with the same symptom during their follow-up, either remitting (monophasic, 63 patients), or with recurrences (polyphasic with the same symptoms, 10 patients). Moreover, we advise caution when drawing conclusions about the proportions of patients with monophasic or polyphasic courses as the mean duration of follow-up was higher for the patients classified as polyphasic (especially in the polyphasic group with different symptoms). It is possible that the follow-up duration of the patients identified as having a monophasic profile was insufficient to identify the polyphasic course (even though these patients were already followed for an average of 5.9 years). On the contrary, this difference could be explained by the fact that patients with a monophasic course of the disease are followed for a shorter period of time because of a more favorable development, therefore not requiring such long follow-up.
While isolated cranial nerve injury and aseptic meningitis responded well to first-line treatment and were more likely presenting a monophasic course and fewer sequelae at the end of follow-up – other presentations, such as encephalic and peripheral presentations, were more often associated with worse prognosis. The latter were more often polyphasic, and often had sequelae at the end of follow-up. Their response to the first-line treatment was also quite heterogeneous, possibly reflecting the variety of types and locations of lesions in these systems, or the wide range of first-line treatments used. This was quite different from spinal presentations. These ones had a poor prognosis in terms of response to treatment and sequelae, but were always monophasic. This homogenous pattern might come from a more aggressive therapeutic strategy with more frequent use of TNF-alpha blockers as first-line treatments. This strategy might induce early disease remission – namely, a monophasic course – but fail to limit sequelae.
Our series was comparable to other published cohorts in terms of demographics. The mean age at onset was 47.8, 55% of the patients were males, which is consistent with previous studies,4,10,34–36 as was the proportion of patients with ‘probable NS’ (66.3%). We decided to categorize patients according to their initial presentation and to use our own definitions of these presentations. Patients with lepto- or pachymeninges involvement were included in the ‘encephalic’ and ‘spinal cord’ groups as it is often difficult to differentiate involvement of the meninges from the spinal or brain parenchyma in real-life conditions. Patients with cranial nerve injury and encephalic lesions were classified in the ‘encephalic’ group rather than in the ‘cranial nerves’ group, as it would seem that their prognosis is more dependent on the parenchymal lesions than on the nerve injury. Patients with hypothalamic and pituitary axis injury were placed in the ‘encephalic’ group for the same reason: we were not able to individualize such patients without encephalic involvement.
Most of the patients (64%) received corticosteroids alone in first-line treatment. To this day, steroids are considered as the cornerstone treatment of NS.4,10,16,28,36–38 Most published works define ‘first line’ as the very first drug administered, regardless of the early use of steroid-sparing DMTs such as methotrexate or azathioprine. Thus, corticosteroids are often described as the initial therapy in almost all patients in these studies. In contrast, we focused on the add-on steroid-sparing DMT in the first-line therapy in our study if initiated at the same time as corticosteroids. Previous studies report that second-line therapy usually consists of methotrexate, followed by mycophenolate mofetil, and azathioprine. 16
TNF-alpha blockers were used at some point in the therapeutic strategy in 33.3% of our patients. This is a higher rate of use compared to other studies, although they are being increasingly used in the management of NS over the past 15 years. Several case reports describe their effectiveness, usually in patients with refractory NS.4,21,22,36,39,40 Infliximab was used in first-line treatment in nine of our patients (10.7%) presenting with severe disease from onset, such as patients with spinal cord involvement, as this type of lesion is known for being aggressive and treatment refractory.7,37,41 The initial response to the first-line DMT is difficult to compare with the literature as the evaluation of the response is highly subjective. Moreover, the first-line treatments used are very different from one study to another, and the variable rate of patients with favorable and more severe forms of the disease deeply influence the outcomes. Fritz et al. 4 reported a review and meta-analysis of 29 articles and 1088 patients with NS, 465 of them having been assessed after DMTs. 4 A total remission was achieved in 27%, a partial remission in 32%, a stabilization in 24%, and a deterioration in 6%. These proportions were of 27%, 29%, 16%, and 29% respectively in our cohort, indicating a more pronounced tendency to worsen in our patients. The reason might be that the assessment of response to treatment in our cohort was limited to first-line DMTs. The only prospective cohort of 32 patients with NS was described in 2003 by Allen et al. 42 Only 59% were treated, all by corticosteroids, and 19% had a full recovery of symptoms, 44% a partial recovery, and 34% a stabilization of symptoms. The remaining 3% (one patient) died from cardiac complications. Of note, 59% of the patients had cranial nerves involvement (isolated or not), which probably indicates a higher proportion of patients with less severe forms of NS. There is no clear consensus to date about what constitutes initial recovery in terms of clinical scales or paraclinical results. We decided to present the initial response according to the initial presentation rather than according to the first-line DMT, because the use of treatments is not independent of the initial prognosis. Thus, low-dose corticosteroids used to treat a favorable form of the disease (e.g. aseptic meningitis) could be viewed as an effective treatment as this form is known to have a good prognosis. On the contrary, TNF-alpha blockers are used for forms of NS with a poor prognosis, such as those with dissemination in the whole CNS. These treatments would therefore be associated with a higher probability of poor response despite a known high efficacy in NS.16,19,20
Our cohort study has some limitations. First, its retrospective design could be responsible for measurement bias and missing data. We minimized measurement bias by limiting the period of inclusion (from 2000 to 2020), as this bias tends to increase with the length of the data collection period. Information bias was limited by systematically referring to medical records, and in case of contentious interpretation of these data, a second neurologist was consulted. As this was a retrospective ‘real-life study’, the initial entry of data into the medical records, patient follow-up, additional examinations, treatment initiation, and follow-up, were not standardized. Obviously, this influences the evaluation of clinical and paraclinical courses. A higher frequency of MRI might have detected more new lesions, thereby reclassifying a disease course as polyphasic. These categories should thus be viewed as mainly clinical, as patients’ complaints and symptoms were more consistently reported. However, any evidence of a new lesion despite stable or improving clinical signs reclassified the patient as polyphasic. Another limitation is that we only included patients who consulted in a neurology department, which could have led to selection bias as patients with NS can also be treated in pulmonology or internal medicine departments, for instance. Furthermore, patients who are treated in tertiary referral centers, as ours, are more likely to present with more severe disease.
Finally, the assessment of the disease courses and the sequelae can be considered as subjective, as it is not based on an overall handicap score. However, to date, no such score has been validated for NS. Although some authors have used the Expanded Disability Status Scale, this tool has not been validated for NS, and does not consider imaging findings and other paraclinical results.
Conclusion
We identified three main specific courses of NS in our patients: monophasic, polyphasic with recurrence of the same symptoms, and polyphasic with expression of different neurological symptoms, this last category being less common. These courses would seem to reflect disease prognosis as evidenced by the response to first-line treatments or in terms of sequalae at the end of follow-up. Patients with isolated injury of the cranial nerves or aseptic meningitis have a better prognosis than other forms of NS involving the parenchyma of the CNS or the PNS. Our study shows that presentation at onset can be a useful tool to help guide the therapeutic strategy and patient management. The disease patterns that we describe here, in one of the largest cohorts reported to date, should be confirmed in further prospective studies.