
Abstract
Background:
Previous studies have shown a potential beneficial effect of endovascular therapy (EVT) in patients with acute basilar artery occlusion (BAO). It was unclear that whether atrial fibrillation (AF) can affect the clinical outcomes for BAO patients treated with EVT.
Objectives:
To investigate the association between AF and clinical outcomes, and whether AF can modify the efficacy and safety of EVT in patients with BAO.
Design:
We conducted a multicenter, nationwide, retrospective analysis to investigate how the presence of AF affects treatment allocation for BAO patients.
Methods:
The endovascular treatment for acute basilar artery occlusion (ATTENTION) registry was a multicenter, prospective study in China that included acute BAO patients who underwent EVT or received best medical management (BMM) between 2017 and 2021. The outcomes include the distribution of 3-month modified Rankin scale (mRS) score, functional independence (defined as mRS 0–3), symptomatic intracerebral hemorrhage, and mortality.
Results:
2134 patients were included in the study, of which 619 had AF and 1515 did not have AF. The median age was 65 (interquartile range [IQR]: 56–73) years, and 689 (32.3%) patients were female. Multivariate regression analysis indicated no significant association existed between AF and the distribution of mRS (adjusted common odds ratio, 1.05 [95% CI: 0.88, 1.25]; p = 0.564) at 90 days. Similarly, AF was not found to have a significant association with and other measured outcomes, or with the effects of EVT in AF subgroups for at 90 days as measured by ordinal mRS (p for heterogeneity = 0.247). Finally, no significant differences were found for symptomatic intracerebral hemorrhage and mortality within 90 days between the EVT and BMM groups across AF subgroups.
Conclusions:
Our results illustrated that the effect of EVT did not differ statistically in acute ischemic stroke patients with and without AF. Moreover, no significant association between AF and functional or safety outcomes could be detected at 90 days.
Introduction
Basilar artery occlusions (BAOs) constitute about 5%–10% of acute intracranial large vessel occlusions.1,2 Compared with acute large vessel occlusions in the anterior circulation, the functional independence in patients with BAO decreases significantly and mortality rates increase significantly.3,4 Previous RCT studies have showed a potential beneficial effect of endovascular therapy (EVT) in BAO patients. Endovascular treatment versus standard medical treatment for vertebrobasilar artery occlusion (BEST) study was terminated early on account of the high cross-over rate. However, ‘per-protocol’ and ‘as-treated’ population results suggested EVT is a better treatment strategy compared to standard medical therapy. Patients with a National Institutes of Health Stroke Scale (NIHSS) score < 10 were included in the modified protocol due to difficulties of enrolment in the Basilar Artery International Cooperation Study (BASICS), resulting in a negative overall result. However, subgroup analysis of the BASICS trial supported EVT performed better than standard medical treatment in BAO patients with moderate to severe onset symptoms, whereby EVT is often recommended for BAO treatment.
Atrial fibrillation (AF) is an established risk factor for acute ischemic stroke (AIS).5–8 Compared with atherosclerotic occlusion, embolic occlusion is related to worse outcomes for patients with BAO.2,9 Several observation trials showed patients with AF have higher hemorrhagic transformation and poorer clinical prognosis compared to those without AF after the implementation of intravenous thrombolysis (IVT) therapy.10,11 A similar association was found in patients treated with EVT.12–14 However, it should be noted that these investigations mostly focused on the occlusion of anterior circulation and led to conflicting results.
Here, we aim to evaluate the association between treatment allocation and clinical outcomes in patients with and without AF. Our results should aid recommendations of personalized therapy strategies and lower the risk of disability and mortality.
Methods
Study population
The present data were derived from ATTENTION (Endovascular Treatment for acute Basilar Artery Occlusion) registry study. 15 ATTENTION is a multicenter, nationwide, prospective registry to estimate treatment effects of best medical management (BMM) and EVT for patients with acute BAO sampled from across 48 stroke centers and 22 provinces in China (http://www.chictr.org.cn; ChiCTR2000041117). All patients or their legal representatives provided signed, informed consent.
Consecutive acute BAO patients were recruited in this trial if (1) BAO was confirmed by neurovascular imaging angiography (magnetic resonance angiography, computed tomographic angiography, and digital subtraction angiography) within 24 hours of estimated time; and (2) patients had an independent daily living defined by an mRS ⩽ 2 before stroke. Patients with another serious illness, evidences of cerebral hemorrhage on presentation and without records of follow-up information were excluded.
Treatments
According to the treatment received, patients were allocated into the BMM or EVT group. Patients in BMM group received IVT with alteplase, anticoagulation, antiplatelet drugs or a combination of the above therapies. Patients in the EVT group received stent retrievers, thromboaspiration, intra-arterial thrombolysis (rt-PA or urokinase), balloon angioplasty, stent deployment, or various combinations of these approaches as decided by the treating physicians.
Outcomes
The primary outcome was the distribution mRS scores toward a better outcome at 3 months. Secondary efficacy outcomes were the proportions of mRS 0–1, 0–2 and 0–3 at 90 days. Safety outcomes were all cause mortality within 3 months after treatment and symptomatic intracranial hemorrhage (sICH).
Statistical analysis
Data were showed as medians (interquartile ranges [IQRs]) or frequencies (percentages). Univariate analyses of baseline characteristics between non-AF and AF groups were performed using Mann–Whitney U test, χ2 test. The primary outcome parameter was the common odds ratio to shift toward a better outcome of mRS score, estimated by multivariable ordinal logistic regression. In addition, binary logistic regression was employed for secondary outcomes, presenting as odds ratio. Several variables, including age, sex, history of stroke or transient ischemic attack (TIA), diabetes mellitus, the time of onset to admission, IVT, location of occlusion, baseline NIHSS score, hypertension, coronary heart disease, and baseline Posterior Circulation-Alberta Stroke Program Early CT Score (pc-ASPECTS), were controlled in the multivariable analysis. We estimated interactions between the AF status and treatment allocation in primary, secondary and safety outcomes, and used multivariable multiple imputation with five datasets to impute the missing data. All analyses were performed with R (version 4.1.0).
Results
Baseline characteristics
A total of 2134 patients constituted the study population (of whom 462 were allocated into BMM group and 1672 were allocated into EVT group), including 619 and 1515 with and without AF, respectively. The baseline characteristics of patients by AF subgroups were presented in Table 1. Patients with AF were older than non-AF patients (66 [57, 74] vs 65 [55, 73]; p = 0.015), showed a higher proportion stroke or TIA history (167 [27.0%] vs 343 [22.6%]; p = 0.033), had higher baseline NIHSS scores (23 [14, 32] vs 20 [12, 29]; p = 0.001), were more frequently treated with EVT (543 [87.7%] vs 1129 [74.5%]) and presented significant differences in occlusion sites (proximal basilar artery 166 [26.8%] vs 548 [36.2%]; middle basilar artery (235 [38.0%] vs 452 [29.8%]; and distal basilar artery (218 [35.2%] vs 515 [34.0%]; p < 0.001). No statistical differences were detected across remaining baseline characteristics between the two groups.
Baseline characteristics of patients by AF subgroups.

AF, atrial fibrillation; EVT, endovascular treatment; IQR, interquartile range; IVT, intravenous thrombolysis; NIHSS, National Institutes of Health Stroke Scale; pc-ASPECTS, Posterior Circulation-Alberta Stroke Program Early CT Score; TIA, transient ischemic attack.
Association of AF and outcomes at 90 days
Table 2 showed the comparisons of efficacy and safety outcomes between AF patients and non-AF patients. Figure 1 presented the distribution of 90-day mRS scores according to AF status. No significant differences were detected in the distribution of mRS scores at 90 days between the two groups (adjusted common odds ratio [OR]: 1.05 [95% confidence interval [CI]: 0.88, 1.25]). The proportions of mRS 0–1, 0–2, and 0–3 at 90 days were also similar between patients with and without AF. In addition, all secondary efficacy and safety outcomes demonstrated no statistical differences exist between both groups.
Clinical outcomes by AF subgroups.

AF, atrial fibrillation; CI, confidence interval; IQR, interquartile range; IVT, intravenous thrombolysis; NIHSS, National Institutes of Health Stroke Scale; pc-ASPECTS, Posterior Circulation-Alberta Stroke Program Early CT Score; sICH, symptomatic intracranial hemorrhage; TIA, transient ischemic attack.
Adjusted variables included age, sex, diabetes mellitus, IVT, baseline NIHSS score, location of occlusion, onset-to-admission, history of stroke or TIA, hypertension, baseline pc-ASPECTS, coronary heart disease, treatment allocation.
Indicates common odds ratio results toward a better outcome.
The odds ratio was assessed by logistic regression model.

Distribution of 90-day modified Rankin Scale (mRS) by AF subgroups.
Association between AF and treatment allocation on outcomes at 3 months
According to the status of AF and treatment allocation, the distribution of mRS scores was shown in Figure 2. MRS scores were similar in the two groups and between BMM and EVT (p for interaction = 0.247). We also found that the treatment allocation did not significantly interact with AF in other efficacy outcomes (proportions of mRS 0–1, 0–2, and 0–3 points), and show that AF and treatment allocation do not impact the rate of sICH or the 90-day mortality (sICH: adjusted p for interaction = 0.977; mortality: adjusted p for interaction = 0.393, Table 3).
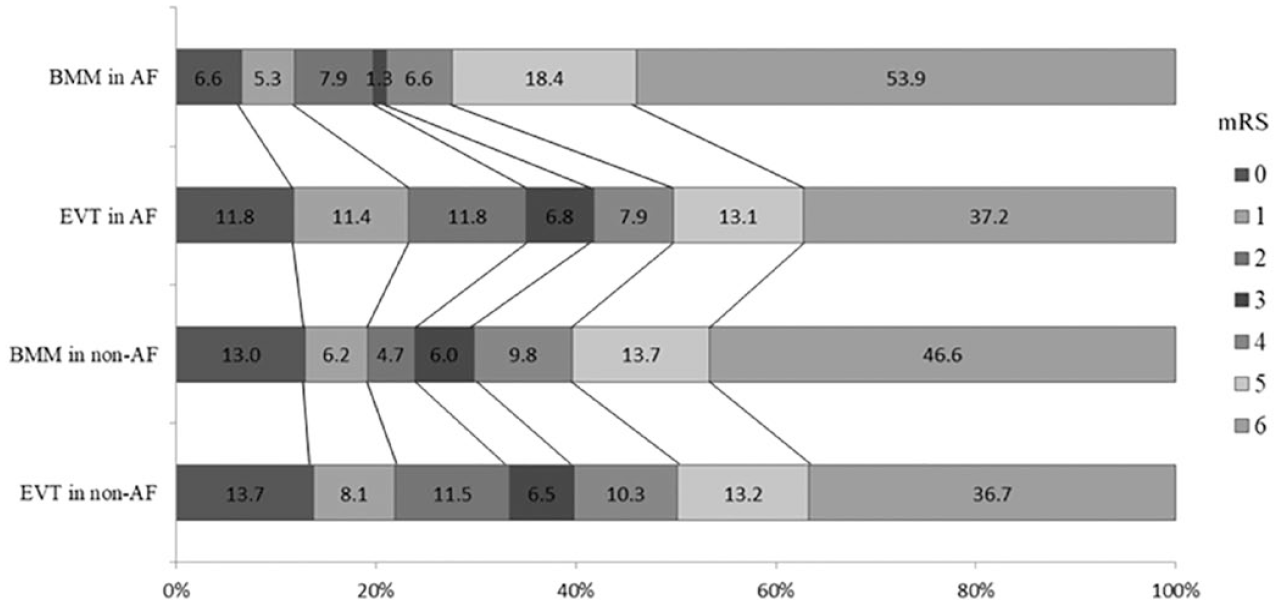
Distribution of 90-day modified Rankin Scale (mRS) by AF subgroups and treatment allocation.
Clinical outcomes by AF subgroups and treatment allocation.

AF, atrial fibrillation; BMM, best medical management; CI, confidence interval; EVT, endovascular treatment; IQR, interquartile range; IVT, intravenous thrombolysis; NIHSS, National Institutes of Health Stroke Scale; pc-ASPECTS, Posterior Circulation-Alberta Stroke Program Early CT Score; sICH, symptomatic intracranial hemorrhage; TIA, transient ischemic attack.
Adjusted variables include: age, sex, diabetes mellitus, IVT, baseline NIHSS score, location of occlusion, onset-to-admission, history of stroke or TIA, hypertension, baseline pc-ASPECTS, coronary heart disease.
The common odds ratio was assessed by ordinal logistic regression model.
The odds ratio was assessed by binary logistic regression model.
Discussion
This subgroup analysis of ATTENTION registry showed a similar effect of EVT on functional outcome, and secondary outcomes (mRS 0-1, 0-2 and 0-3 at 90 days, sICH and mortality at 90 days) in AF and non-AF BAO patients. In addition, AF was not related to efficacy and safety outcomes in acute BAO patients.
Patients with BAO caused by AF appeared to be more likely to receive EVT. The incidence of AF in the BEST trial was 27% in patients who received EVT compared to 15% in patients who received BMM. 16 In BASIC trial, the proportion of AF patients in the EVT group (24%) was also higher than those in the BMM group (15%). 17 The underlying reason for the higher use of EVT among BAO patients with concurrent AF remains unclear but may be related to a more abrupt onset and rapid diagnosis of this condition. However, we observed no significant changes associated with EVT effect of AF and non-AF BAO patients in our trial, suggesting that EVT should be performed regardless of the patients had AF or not.
A subgroup analysis of the MR CLEAN trial which mostly enrolled patients with occlusion of anterior circulation found worse clinical outcomes for AF-caused AIS patients after EVT compared to non-AF patients. 18 However, the sample size of AF patients was small and the interpretation of the results should be made cautious. A subsequent meta-analysis from the HERMES collaboration and the ANGEL-ACT registry trials supported no significant interaction effect between AF and functional outcomes at 90 days after EVT.14,19 Here, our study showed that EVT had similar effects on AF and non-AF patients, whereby AF status should not influence clinical decision to conduct thrombectomy for acute BAO patients.
To consistent with previous reports on EVT in anterior circulation, we found no association between AF and 90-day functional outcomes for patients with acute BAO. Accumulating evidence in patients with anterior circulation occlusions supported the neutral association between AF and long-term functional outcomes after EVT,14,19 and limiting evidence from studies focused on BAO patients also supported this neutral association.20–24
For death at 90 days and symptomatic ICH, the differences between the EVT and BMM versus BMM alone groups were similar between the AF subgroups. No determined association between AF and hemorrhage transformation could be drawn in AIS patients after reperfusion therapy.19,18,25–27 However, the absolute risk of sICH after EVT due to BAO remains low.16,17,28 The ATTENTION registry trial suggests that EVT should not be abandoned for fears of post-treatment hemorrhagic transformation regardless of AF status.
Our analysis contains remarkable statistical power by including 2134 patients with BAO from 48 centers nationwide. The study does have limitations, including the fact that Asians have high rates of intracranial atherosclerotic diseases, which might hamper extending this to other populations. However, we note that the proportion of AF observed in the ATTENTION registry was similar to those of the BASICS trial; in addition, most patients did not receive a 24-hour electrocardiogram after admission, whereby it is possible that patients with paroxysmal AF were not included in the AF group.
The subgroup analysis of the ATTENTION registry demonstrates that the efficacy and safety of EVT does not differ significantly between AF and non-AF BAO patients, and that no significant associations exist between AF and functional outcomes at 90 days in patients with acute BAO.