
Abstract
Background:
Intraplaque neovascularisation (IPN) is a component of vulnerable atherosclerotic plaque, which is a biomarker of cardiovascular events. However, the identification of patients with high probability of ischaemic events after carotid artery stenting (CAS) is mainly based on vascular risk factors. Prospective studies on the development of plaques are lacking.
Objectives:
The purpose of this study was to investigate whether IPN detected by contrast-enhanced ultrasound is related to the occurrence of ischaemic events after CAS.
Methods:
Sixty consecutive patients receiving CAS were prospectively enrolled in our centre. The patients were evaluated using contrast-enhanced ultrasound before CAS. According to the degree of microbubble enhancement, IPN was graded from 0 to 2. Endpoint events, including ischaemic stroke and other cardiovascular events, were recorded during follow-up. Kaplan–Meier survival curves and Cox proportional-hazards models were used to evaluate the risk factors for endpoint events. At a median follow-up of 30 months, 13 patients (28.9%) experienced endpoint events. Kaplan–Meier survival curves showed that patients with grade 2 IPN had a higher risk of future ischaemic events than those with grade 0 or 1 IPN (p < 0.05). Cox proportional-hazards models showed that grade 2 IPN [adjusted hazard ratio (HR), 4.049; 95% confidence interval (CI), 1.078–15.202] was a significant predictor of endpoint events (p < 0.05).
Conclusion:
Grade 2 IPN evaluated by contrast-enhanced ultrasound has predictive value for ischaemic events in patients after CAS and may help clinicians identify high-risk patients who need close follow-up.
Plain Language Summary
Keywords
Introduction
Carotid atherosclerotic stenosis accounts for 10–25% of the cases of ischaemic stroke. Carotid artery stenting (CAS), one of the main treatments for patients with severe carotid stenosis, aims to reduce the long-term risk of ischaemic events. 1 However, because of systemic atherosclerosis and the shortcomings of interventional therapy, patients may still experience ischaemic events after CAS.2,3 A large number of studies have shown that risk factors, such as age, female sex, smoking and diabetes mellitus, are independent predictors of ischaemic events after carotid artery interventional therapy. 4
Along with the identified risk factors, the relationship between local components of carotid plaque and ischaemic events after interventional therapy has gradually attracted researchers’ attention in recent years.5,6 With the help of carotid endarterectomy, scholars used the obtained carotid plaque specimens for histopathological analysis and found that the histological characteristics of carotid plaque, such as intraplaque neovascularisation (IPN) and intraplaque haemorrhage (IPH), are helpful in predicting the occurrence of cardiovascular events after carotid endarterectomy. 7 In patients undergoing CAS, the characteristics of carotid plaque may be evaluated by imaging to determine the risk of ischaemic events. One study suggested that the ultrasound characteristics of a vulnerable carotid plaque are strongly associated with complications after CAS. 8 Some researchers have pointed out that carotid hypoechoic plaque has predictive value for in-stent restenosis. 9 In addition, another study with a small sample size showed that plaques detected by contrast-enhanced ultrasound (CEUS) were significantly correlated with in-stent intimal hyperplasia. 10 CEUS can observe IPN through the degree of microbubble enhancement and can be used as a screening method to detect plaque vulnerability. However, to our knowledge, the predictive value of carotid plaque characteristics assessed using CEUS for ischaemic events in patients after CAS has not been discussed.
Therefore, in this prospective study, we aimed to explore whether IPN detected by CEUS is related to the occurrence of future ischaemic events in patients after CAS. We hypothesised that the presence of grade 2 IPN assessed by CEUS has a predictive value for future ischaemic events.
Methods
Study population
This prospective study was performed in line with the principles of the World Medical Association’s Declaration of Helsinki and was approved by the ethics committee of our centre (No. 2015-285). All patients provided written informed consent. From April 2016 to February 2018, 60 consecutive patients with carotid artery stenosis who underwent CAS were enrolled in the First Hospital of Jilin University, following the Chinese Guidelines for Intravascular Intervention Diagnosis and Treatment of Ischaemic Cerebrovascular Disease 2015. 11 Neurological symptoms were assessed by neurologists, and symptomatic patients had at least moderate stenosis as assessed by carotid ultrasound. Asymptomatic patients had at least severe stenosis on carotid ultrasound, and wanted surgical treatment. The exclusion criteria included: (1) heavy calcification of carotid plaques, (2) non-atherosclerotic causes of stenosis, (3) loss to follow-up or withdrawal during the study and (4) poor imaging on CEUS.
Clinical data collection
Background factors and laboratory test values were recorded, including: (1) demographic data such as age and sex; (2) risk factors such as smoking, alcohol abuse, hypertension, diabetes mellitus, previous ischaemic stroke (if a patient had an ischaemic stroke in the prior 6 months, then we considered the patient as having a previous ischaemic stroke), coronary heart disease and family history; (3) serological indices such as blood lipids (triglycerides, cholesterol, low-density lipoprotein and high-density lipoprotein), homocysteine, high-sensitivity C-reactive protein, vitamin B12 and folic acid; and (4) whether the patient had symptomatic carotid stenosis at admission. Symptomatic carotid stenosis was defined as an ischaemic stroke with focal neurological symptoms in the distribution area of the carotid artery and confirmed by imaging via magnetic resonance imaging or computed tomography within the previous 1 month. Asymptomatic carotid stenosis was defined as the clinical manifestations of only dizziness or mild headache without a transient ischaemic attack, stroke or other related neurological symptoms in the past 6 months.
Ultrasonography imaging protocol
Carotid ultrasound
Before CAS, all patients underwent routine carotid CEUS. Carotid stenosis was assessed according to the stenosis criteria of the North American Symptomatic Carotid Endarterectomy (NASCET) method and classified as mild (<50%), moderate (50–69%) or severe (⩾70%). 12 Because international criteria for carotid restenosis have not been defined, our institution still uses the NASCET method as a restenosis diagnostic criterion. According to the Gray-Weale visual classification system, plaque echogenicity was graded as follows: uniformly hypoechoic (type I), predominantly hypoechoic (type II), predominantly hyperechoic (type III), uniformly hyperechoic (type IV) or extensively calcified (type V). 13 Type V plaques were excluded because they were accompanied by intense acoustic shadowing precluding IPN analysis. We classified type I and II plaques as hypoechoic and type III and IV as hyperechoic.
The degree of stenosis was identified in the narrowest portion of the carotid artery. The target plaque, defined as the plaque causing luminal stenosis, was visualised in longitudinal and transverse sections. The plaque size, location and echogenicity were recorded. Next, the IPNs were examined using CEUS by the same examiner, and intraplaque contrast enhancement was recorded. Raw images were stored on a proprietary hard disc to facilitate offline analysis. Both examinations were completed by a sonographer with 10 years of experience (Y.C.), and the examination methods have been previously described. 14
IPN assessment
Based on the degree of intraplaque microvesicle enhancement, IPNs were classified into three grades: grade 0, no enhancing microvesicles within plaques; grade 1, enhancing microvesicles localised exclusively to the shoulder and adventitial side of the plaque; and grade 2, extensively enhancing microvesicles observed in the plaque (Figure 1). 15 Offline images were analysed to determine IPN grade by two experienced CEUS sonographers (Y.X. and L.W., each with 10 years of experience), who were blinded to patient information and the results of each other’s analyses. When the results were inconsistent, they jointly decided after discussion.

Typical examples of plaques: left, intraplaque neovascularisation detected by contrast-enhanced ultrasound; right, the target plaque detected by carotid ultrasound. (a) Grade 0: no enhancing microvesicles within the plaque. (b) Grade 1: enhancing microvesicles localised exclusively to the shoulder and adventitial side of the plaque. (c) Grade 2: extensively enhancing microvesicles in the plaque. The arrow represents enhancing microvesicles.
Carotid artery stenting
Patients were administered aspirin (100 mg/day) and clopidogrel (75 mg/day) for at least 3 days before surgery. Heparin (1 mg/kg) was administered at the beginning of the operation to maintain an activated clotting time of approximately twice the baseline value. All operations were performed by experienced surgeons under local anaesthesia using Seldinger’s method via the femoral artery approach, followed by carotid and cerebral angiography to assess the degree of vascular stenosis. All patients used an embolic protective device (EPD). If necessary, pre-dilation was performed after EPD placement. The stent (including Precise, Wallstent or Acculink) was then placed at the carotid stenosis. The selection of the support size was based on the diameter of the common carotid artery and internal carotid artery. If stent expansion was insufficient, post-dilation was performed. The operator determined the selection of the catheter and guidewire. To prevent complications after CAS, if tolerated, the patients were prescribed aspirin and clopidogrel for 3 months, and then aspirin for life. Carotid ultrasound (Aplio500, 4–11 MHz linear probe; Toshiba, Tokyo, Japan) was regularly performed after CAS to evaluate the degree of carotid restenosis. Patients with hyperlipidaemia took lipid-lowering drugs.
Follow-up
The patients were followed up every 6 months, and medication adherence and endpoint events were recorded. Endpoint events included ischaemic stroke or other cardiovascular events, as previously described. 16 Good medication adherence was defined as taking medications for more than 80% of the follow-up days.
Restenosis after CAS was also recorded. Patients were regularly reviewed for carotid stenting after surgery, and the latest re-examination results before the end of the study were used as the basis for decision to perform carotid stent restenosis.
Statistical analysis
SPSS version 26.0 (IBM Corp., Armonk, New York, USA) was used for the statistical analysis. The Shapiro–Wilk test was used to evaluate whether continuous variables conformed to a normal distribution (p > 0.05, normal). Continuous variables with a normal distribution were expressed as mean ± standard deviation, and continuous variables with a non-normal distribution were expressed as median and interquartile range. The parameters between the two groups were compared using Student’s t-test or non-parametric tests. Categorical variables are expressed as frequency and percentage (%), and the parameters between the two groups were compared using the chi-square test or Fisher’s exact test. To compare the effect of IPN grades on endpoint events, the log-rank test was used for analysis, and the Kaplan–Meier method was used to draw the risk curve. Finally, Cox proportional-hazards regression analysis was used to determine the independent risk factors for future ischaemic events in patients with CAS. Variables with p < 0.10 in the univariate analysis were incorporated into the Cox proportional-hazards regression model to obtain the final predictors. Cohen’s kappa coefficient was used to evaluate inter- and intra-observer agreements. All statistical tests were two-tailed (p < 0.05).
Results
Clinical outcome
In this study, 60 patients who underwent CAS were included, of whom 6 could not be analysed due to heavy calcification of carotid plaques, 5 were lost to follow-up, 1 withdrew halfway through the study, 2 had carotid stenosis not due to atherosclerosis and 1 had poor CEUS imaging. In total, 45 patients were analysed (Figure 2). At a median follow-up of 30 months, 13 patients (28.9%) had endpoint events and were classified into the ‘with events’ group, and the remaining 32 patients were assigned to the ‘without events’ group. In the ‘with events’ group, eight patients experienced a cardiovascular event and five patients experienced a cerebrovascular event.

Study flow chart.
Baseline clinical characteristics
The baseline clinical data of the patients are presented in Table 1. The mean age was 65 ± 7.3 years, and 43 patients (95.6%) were men. Compared with the ‘without events’ group, the ‘with events’ group had a significantly larger number of people with diabetes mellitus (p = 0.011). There were more smokers in the ‘with events’ group than in the ‘without events’ group (p = 0.046). However, there were nine patients (69.2%) with clinical symptoms in the ‘with events’ group and 18 patients (56.3%) with clinical symptoms in the ‘without events’ group, which was not significantly different between the two groups. In addition, serological indicators and medication adherence were similar in both groups (p > 0.05).
Baseline characteristics of the patients (N = 45).

HCY, homocysteine; HDL, high-density lipoprotein; hs-CRP, high-sensitivity C-reactive protein; IPN, intraplaque neovascularisation; IQR, interquartile range; LDL, low-density lipoprotein; SD, standard deviation.
Plaque characteristics and restenosis
There were significantly more patients with grade 2 IPN in the ‘with events’ group than in the ‘without events’ group (p = 0.005). The proportion of hypoechoic plaques (types I and II) was higher in the ‘with events’ group than in the ‘without events’ group (p = 0.066), although the difference was not significant (Table 2).
Plaque characteristics and restenosis of the patients (N = 45).

IPN, intraplaque neovascularisation.
At the end of follow-up, only 39 patients were regularly reviewed for carotid stents after surgery. Among the nine patients with restenosis after CAS, five had moderate stenosis, four had mild stenosis and none had severe stenosis. In the ‘with events’ group, four patients developed restenosis, while five patients had restenosis in the ‘without events’ group (p = 0.238), a statistically insignificant difference.
Risk factors for IPN
Patients were allocated into an ‘absence of neovascularisation’ group (grade 0, n = 6 patients) or a ‘presence of neovascularisation’ group (grades 1 and 2, n = 39 patients) according to the grade of IPN detected by CEUS. The proportion of smoking patients in the ‘presence of neovascularisation’ group was higher than that in the ‘absence of neovascularisation’ group (p = 0.049). Patients in the ‘presence of neovascularisation’ group were significantly more likely to have had a previous ischaemic stroke compared with those in the ‘absence of neovascularisation’ group (p = 0.069). There was no significant difference in cardiovascular risk factors between the two groups (p > 0.05; Table 3).
The relationship between IPN and vascular risk factors (N = 45).
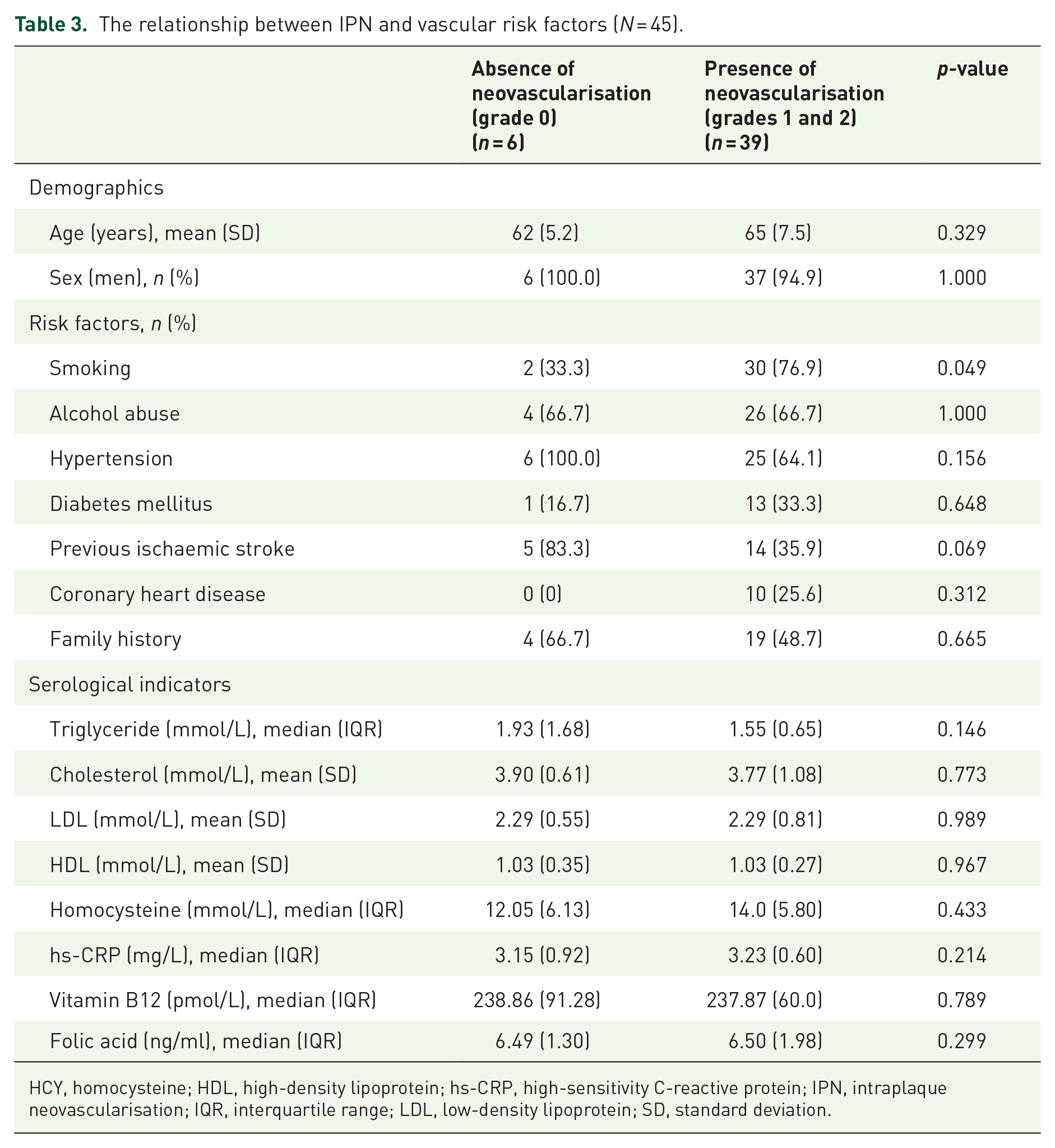
HCY, homocysteine; HDL, high-density lipoprotein; hs-CRP, high-sensitivity C-reactive protein; IPN, intraplaque neovascularisation; IQR, interquartile range; LDL, low-density lipoprotein; SD, standard deviation.
For the assessment of IPN grading, the inter-observer and intra-observer agreements were 0.745 and 0.780, respectively, both showing good reliability.
Independent predictors of endpoint events
To investigate the predictive value of IPN for future vascular events in patients who underwent CAS and to adjust for potential confounding factors, Kaplan–Meier survival curves were plotted (Figure 3), and Cox regression models were fitted (Table 4). Kaplan–Meier survival curves revealed that patients with grade 2 IPN before CAS had an increased risk of future vascular events. Univariate Cox proportional-hazards models showed that grade 2 IPN and diabetes mellitus were significant predictors of endpoint events (p < 0.05). In the multivariable Cox proportional-hazards models, the adjusted hazard ratio (HR) for grade 2 IPN was 4.049 [95% confidence interval (CI), 1.078–15.202], and the adjusted HR for diabetes mellitus was 3.647 (95% CI, 1.153–11.543), indicating that both are independent predictors of future vascular events in patients who underwent CAS.

Kaplan–Meier survival curve. Results show the predictive value of intraplaque neovascularisation grade for endpoint events. The deleted data are represented by a vertical bar.
Predictors of endpoint events.

CI, confidence interval; HCY, homocysteine; HDL, high-density lipoprotein; HR, hazard ratio; hs-CRP, high-sensitivity C-reactive protein; IPN, intraplaque neovascularisation; LDL, low-density lipoprotein.
Discussion
To the best of our knowledge, this is the first study that correlated IPN assessed using CEUS to clinical follow-up outcomes in patients with CAS. In this prospective study, we found that grade 2 IPN could predict the risk of ischaemic events in patients after CAS. Grade 2 IPN is independently associated with the occurrence of endpoint events, and this cannot be explained by traditional risk factors or other potential confounding factors.
The relationship between the carotid plaque components and adverse clinical outcomes has several implications. There remains an urgent need for useful clinical diagnostic tools for risk stratification in patients undergoing interventional therapy. Thus, the epidemiological method for linking cardiovascular risk factors with clinical results still has some limitations in predicting the occurrence of ischaemic events after interventional surgery, which makes it difficult for clinicians to make treatment decisions. Therefore, researchers have attempted to identify effective markers of cardiovascular vulnerability.
Considering that carotid plaque specimens can be obtained by carotid endarterectomy, histopathologic study was done, and it was found that the vulnerable components of carotid plaque (IPN and IPH) can increase the risk of cardiovascular events after interventional therapy.7,17,18 Another study also showed that the number of mast cells in the plaque was positively correlated with the density of neovascularisation, which was an independent risk factor for cardiovascular events. 19 Predicting the risk of ischaemic events after interventional therapy by detecting vulnerable carotid plaque can help identify high-risk patients who may need close follow-up; however, it is difficult to obtain carotid plaque specimens. For patients with CAS, imaging studies are required to verify the impact of plaque vulnerability on ischaemic events after CAS.
In this study, we hypothesised that plaque characteristics, based on the systemic nature of atherosclerosis, may show similarities between vascular regions. Therefore, we studied the relationship between the characteristics of carotid plaques and ischaemic events caused by the progression of atherosclerotic disease. We found that there were significantly more patients with hypoechoic plaque and grade 2 IPN in the ‘with events’ group than in the ‘without events’ group. Hypoechoic plaques are considered to be related to a large lipid core and IPH in plaques. 20 IPN is considered to represent the active progression of atherosclerosis, which is related to plaque inflammation and is one of the main causes of IPH. 21 The underlying mechanism of vulnerable plaque as an independent predictor of future ischaemic events in patients after CAS is still unclear. Previous studies reported that the high lipid core plaque assessed by catheter-based near-infrared spectroscopy is related to the cerebral embolism signal shown by diffusion-weighted imaging (DWI) after CAS. 22 In addition, some scholars further confirmed that the plaque components evaluated using the Hounsfield unit (HU) value of multi-detector computed tomography (HU <0 and HU: 0–60) were related to the number of cerebral embolism signals displayed by DWI after CAS. 23 Recent reports have shown that kurtosis obtained by CT angiography texture feature (density histogram) analysis is an independent predictor of perioperative adverse consequences of CAS in patients with carotid plaque. 24 These findings may partly explain the relationship between plaque vulnerability and ischaemic events in patients after CAS.
This is the first report on the relationship between IPN detected by CEUS and ischaemic events after CAS. In our study, compared with the hypoechoic characteristics of plaques, the final Cox regression model revealed IPN as an independent predictor of future ischaemic events in patients after CAS. For patients with endpoint events, ischaemic stroke (n = 5) and cardiovascular events (n = 8) were reported. One study showed that patients with vulnerable plaques assessed by carotid ultrasound had a significantly increased risk of ischaemic stroke after CAS, suggesting that hypoechoic plaques have clinical value in risk stratification after CAS. 5 Consistent with this, despite a lack of statistical differences that might be attributed to small sample size, our results also showed that the proportion of patients with hypoechoic plaques in the ‘with events’ group was higher than in the ‘without events’ group. Only one study has reported that plaque enhancement detected by CEUS was significantly associated with the occurrence of in-stent intimal hyperplasia. However, this study included only 14 patients and did not explore the clinical outcomes of the patients after CAS. 10
In addition, we recorded post-stent restenosis after CAS, and the degree of carotid restenosis after stenting was mild or moderate. Our findings showed that there was no correlation between carotid restenosis and adverse follow-up outcomes, which could have various explanations. First, the standard carotid ultrasound to evaluate the degree of carotid stenosis is formulated for naturally developing carotid stenosis. Therefore, although carotid ultrasonography is the most used method to evaluate carotid restenosis in patients after stenting, there is still no unified standard for the evaluation of carotid restenosis after stenting. Based on previous studies, two methods define restenosis using carotid ultrasound, categorising the stenosis rate as ⩾50% or ⩾70%.24,25 The restenosis rate was related to the follow-up time and patient background. Second, some studies have suggested that although carotid restenosis after CAS can lead to adverse ischaemic events, most patients with carotid restenosis remain asymptomatic.26,27
IPN can predict ischaemic events in patients after CAS, and this may have various mechanisms. Atherosclerosis is a systemic disease, and local plaques may indicate vulnerable characteristics of other vascular regions. Enomoto et al. 28 showed that 49.1% of patients treated with CAS had comorbid coronary artery disease, whereas Hoffman et al. 29 reported a higher proportion (77.1%). In addition, haemodynamic instability during CAS may lead to myocardial injury.30,31 IPN assessed by CEUS is helpful in identifying patients at high risk after CAS, has prognostic value for the development of future ischaemic events, and allows patients in high-risk subgroups to be followed up regularly and closely. Therefore, the results of this study can provide additional useful information for clinical decision-making.
In this study, we demonstrated that diabetes mellitus is closely related to future vascular events in patients after CAS. It has been reported that the risk of stroke or death after CAS increases significantly after age 75 years. 32 A recent study supported the inclusion of diabetes mellitus in risk score calculators to assess cardiovascular events within 30 days after CAS. 33 Tsujimoto et al. 34 pointed out that increased platelet reactivity in diabetic patients may be associated with poor prognosis after CAS. The abnormal metabolic state of diabetes affects platelet and endothelial function, increases adhesion of endothelial cells with platelet activation and aggregation and ultimately promotes thrombosis. In addition, hyperglycaemia can induce an oxidative stress response, and the release of inflammatory substances further worsens the state of thrombosis. 35 Therefore, the beneficial effect of controlling risk factors in patients after CAS should be emphasised.
This study had some limitations. First, it was a single-centre prospective study with a small sample size. In the future, large-sample and multi-centre studies are needed to further verify these conclusions. Second, there were few female patients in the study; therefore, it is impossible to explore the impact of sex on adverse results after CAS. Third, we excluded patients with heavy plaque calcification because calcification may have biased our results.
Conclusion
In conclusion, this is the first prospective study to explore the relationship between IPN and ischaemic events after CAS. We report that preoperative IPN identified using CEUS is associated with an increased risk of ischaemic events after CAS. These results provide a new clinical marker for predicting secondary events in high-risk patients and a method for clinicians to identify patients who require close follow-up.