
Abstract
The clinical manifestations of proximal (extracranial) internal carotid artery occlusions (pICAOs) may range from asymptomatic to acute, large, and devastating ischemic strokes. The etiology and pathophysiology of the occlusion, intracranial collateral status and patient’s premorbid status are among the factors determining the clinical presentation and outcome of pICAOs. Rapid and accurate diagnosis is crucial and may be assisted by the combination of carotid and transcranial duplex sonography, or a computed tomography/magnetic resonance angiography (CTA/MRA). It should be noted that with either imaging modalities, the discrimination of a pseudo-occlusion of the extracranial internal carotid artery (ICA) from a true pICAO may not be straightforward. In the absence of randomized data, the management of acute, symptomatic pICAOs remains individualized and relies largely on expert opinion. Administration of intravenous thrombolysis is reasonable and probably beneficial in the settings of acute ischemic stroke with early presentation. Unfortunately, rates of recanalization are rather low and acute interventional reperfusion therapies emerge as a potentially powerful therapeutic option for patients with persistent and severe symptoms. However, none of the pivotal clinical trials on mechanical thrombectomy for acute ischemic stroke randomized patients with isolated extracranial large vessel occlusions. On the contrary, several lines of evidence from non-randomized studies have shown that acute carotid endarterectomy, or endovascular thrombectomy/stenting of the ICA are feasible and safe, and pοtentially beneficial. The heterogeneity in the pathophysiology and clinical presentation of acute pICAOs renders patient selection for an acute interventional treatment a complicated decision-making process. The present narrative review will outline the pathophysiology, clinical presentation, diagnostic challenges, and possible treatment options for pICAOs.
Keywords
Introduction
Isolated acute and symptomatic proximal (extracranial) internal carotid artery occlusions (pICAOs) are not rare among acute ischemic stroke (AIS) patient cohorts. In a comprehensive analysis of more than 4,000 consecutive AIS patients, Weimar et al. found symptomatic occlusion of the extracranial carotid arteries in 366 patients (8.8%). Of those, 19 patients (0.5%) had occlusion of the common carotid artery, 269 patients (6.5%) of the proximal internal carotid artery (ICA), and 116 patients (2.8%) of the distal ICA. A concurrent middle cerebral artery (MCA) occlusion, hence tandem occlusion, was present in 52 (14.2%) of 366 patients with extracranial carotid artery occlusion. 1 Ιn the Perugia Stroke Registry 182 patients (11% out of 1,598 consecutive AIS patients) were diagnosed with pICAO. Ten patients had coexisting contralateral ICA occlusion and 15 high grade contralateral ICA stenosis of >70%. 2 A more recent study of 4,942 consecutive patients with anterior circulation AIS documented isolated pICAOs in 146 cases (3%). 3
The clinical presentation of acute pICAOs varies substantially and may range from a totally asymptomatic discovery to large and fatal hemispheric infarcts. 4 Several factors, discussed in detail below, may determine the clinical presentation and course of acute pICAOs. On the contrary, tandem occlusions, defined as the simultaneous presence of pICAO with occlusion of the intracranial ICA or MCA, are always symptomatic and constitute 10%–20% of all large vessel occlusion attributed AIS. 5 Therefore, accurate and prompt diagnosis of pICAOs, including the exclusion of distal coexisting occlusions or isolated intracranial large vessel occlusion (LVO), is important and can be accomplished with the aid of neurosonology, computed tomography angiography (CTA) or magnetic resonance angiography (MRA).6–8
Treatment strategies for the management of acute pICAOs vary substantially across stroke centers. The lack of unambiguous treatment protocols reflects the absence of randomized data, since none of the pivotal randomized-controlled clinical trials (RCTs) of mechanical thrombectomy (MT) for LVO-related AIS included patients with isolated extracranial LVO. 9 On the contrary, approximately 9% of the participants in RCTs of MT for LVO-attributed AIS harbored tandem occlusions, which did not result in any treatment effect heterogeneity. 10 Treatment options for acute pICAOs include conservative treatment (no acute reperfusion treatment) focusing on secondary prevention and hemodynamic stability, intravenous thrombolysis (IVT), and urgent endovascular recanalization or endarterectomy. 11 The latter is supported only by observational data, hence the low level of evidence.
In the present narrative review, we highlight aspects concerning the clinical presentation, diagnosis, pathophysiology, and treatment options for acute symptomatic isolated pICAOs. We also present a diagnostic and treatment algorithm that may prove useful to stroke physicians and interventionalists in the acute stroke setting.
Clinical presentation and natural course
The clinical presentation of acute pICAOs may vary from asymptomatic to acute, large, and devastating ischemic strokes. Rates of asymptomatic pICAO are not easy to estimate but may be as high as 50% of cases. 4 Neurological manifestations originate in critically hypoperfused brain regions irrigated by the MCA, the anterior cerebral artery (ACA), the anterior choroidal artery, or the posterior cerebral artery (PCA) in cases with fetal-type P1 segment of the ipsilateral PCA. 12 An intriguing clinical manifestation, observed typically in severe steno-occlusive ICA disease, is the limb shaking syndrome. It is characterized by rhythmic involuntary movements of a single or both limbs contralateral to the diseased ICA. The abnormal movements typically occur while walking, standing, or during neck hyperextension and resolve when patients are put in the supine position. 13 Hypoperfusion of the ophthalmic artery, the first branch of the ICA, causes transient monocular vision loss (amaurosis fugax), progressive vision loss, or retinal claudication, the latter characterized by episodes of unilateral visual loss in bright light. 14
In all, 8%–33% of patients with acute pICAOs present with single or recurrent transient ischemic attacks (TIAs).1,4 TIAs may precede an AIS in more than half of cases. 15 Luckily, among all patients admitted with symptomatic pICAO, 52%–63% experience either TIAs or suffer minor strokes at presentation.3,4 Moderate to severe strokes, with National Institutes of Health Stroke Scale (NIHSS) scores of more than 5 points, occur in 40%–50% of patients and are associated with poor outcome. 3 Notably, blood pressure-depended clinical fluctuations, reflecting hemodynamic insufficiency, are common during the acute phase heralding unfavorable outcomes. 16
Recurrence rates due to acute pICAOs, both on early or late times after initial presentation, are high. In the study by Weimar et al., among 366 patients with common carotid artery (CCA)/ICA occlusion recurrent cerebral ischemia within 72 h occurred in 7.4% of cases. Similarly, stroke within 1 year follow-up was reported in 10% of patients. Mortality rates 1 year after diagnosis were at 26.5%, similar to those in patients diagnosed with MCA occlusion (note that the study was published in the pre-MT era), but higher than the 1-year mortality rates observed in patients with CCA/ICA or other intracranial vessel symptomatic stenosis. 1
Etiology and pathophysiology
The leading cause of ICA occlusion is atherosclerotic vascular disease, responsible for the 47%–65% of cases.1,2 Other causes include cardioembolism, arterial dissection, carotid web, vasculitis, and irradiation, the latter two conditions being the most uncommon. 17 In the Internal Carotid ARtery Occlusion studies (ICARO and ICARO-3) 55.5% of the recruited patients had an atherosclerotic etiology, 16.6% a cardioembolic, and in 14.2% an arterial dissection was diagnosed.18,19 Among the uncommon causes giant cell arteritis may very rarely cause acute extracranial ICA occlusion, but its prompt diagnosis is critical. 20 The clinical manifestations following acute pICAOs are attributed either to distal embolization of thromboembolic fragments originating in the occluded ICA, or to hemodynamic failure. 12
The presentation and outcome of pICAOs depends on several factors including the speed of progression to complete vessel occlusion, the presence or absence of significant pre-occlusion stenosis, the patency of the contralateral ICA, and the intracranial collateral status. 21 Four different infarct patterns may occur as a result of acute ICA occlusions: territorial infarcts related to embolization of distal MCA or anterior cerebral artery (ACA) branches, subcortical infarcts resulting from either embolization of deep perforating MCA branches or occlusion of the MCA with efficient leptomeningeal collaterals, disseminated lesions in distal cortical regions, and watershed infarcts at the internal MCA or cortical [between MCA and ACA or MCA and posterior cerebral artery (PCA)] borderzone territories. 22 In a study comprising 101 patients with total symptomatic ICA occlusion, watershed infarcts and patent posterior communicating cerebral artery (PCoA) were associated with more favorable prognosis. 15 Similarly, collateral flow via the PCoA was associated with a low prevalence of border zone infarcts. 21
In acute ICA occlusions, without clinically significant distal embolization, the outcome depends largely on the collateral status. Both primary and secondary collaterals, via anastomoses, are recruited to augment blood flow into the ipsilateral to the occlusion MCA territory. Primary collaterals consist of blood flow reversal in the ipsilateral ophthalmic artery, PCoA and the A1 segment of the ACA through a patent anterior communicating artery (ACoA), the latter being probably the most efficient collateral pathway. 23 However, hypoplasia or aplasia of the ACoA is present in 25% of cases, whereas a complete circle of Willis exists in only 20% of individuals. 24 Coexistent stenosis of the contralateral ICA is not uncommon and may further compromise blood supply into the affected cerebral hemisphere. 6 In addition, severe stenosis of the ipsilateral external carotid artery (ECA) has been recognized as a risk factor of AIS occurrence and death following ICA occlusion.4,25
Diagnosis
Diagnosis of acute pICAO is accomplished by means of duplex sonography, CTA, MRA, or digital subtraction angiography (DSA). The accuracy of carotid duplex ultrasonography in diagnosing total carotid occlusion is reported as high as 97%, with a positive predictive value of 96%, a negative predictive value of 98%, a sensitivity of 91%, and a specificity of 99%.26,27 The direct sonographic signs of cervical artery ultrasound to diagnose ICA occlusion include absence of color and flow in proximal ICA in the duplex and spectral modes, respectively, whereas indirect signs are increased resistivity index in the ispilateral CCA and spectral ‘internalization’ with reduced resistivity index in the ipsilateral ECA. 28 In addition, the sonographer may obtain important information about the origin of the occlusion and differentiate between a floating and hypoechoic thrombus, an underlying atheromatous plaque, or a dissection. 6 The latter can be diagnosed by the direct visualization of intimal flap, pseudolumen, or hypoechoic vessel wall thickening, especially when contralateral atherosclerosis is absent. 29 The distinction between total carotid artery occlusion and near-occlusion is often challenging and highly operator depended. A recent study comprising 548 patients that underwent carotid artery ultrasound and CTA showed that ultrasound had a specificity of 99% (95% confidence interval [CI]: 99%–100%) but a sensitivity of only 22% (95% CI: 14%–30%) for detecting near-occlusions. Importantly, 13 (13%) cases of near-occlusions were interpreted as total occlusions. 30
Transcranial ultrasound examination will in turn detect and characterize the type and adequacy of collateral circulation through the circle of Willis and the ophthalmic artery. 31 A recent study evaluated the collateral status in 113 acute stroke patients with unilateral ICA occlusions. Among the different collateral pathways activated, the ACoA was the most frequent in 81% of cases, followed by the ophthalmic artery in 63%, the PCoA in 53%, and the leptomeningeal collaterals of the PCA in 22% of cases. Efficient collateralization was dependent on the presence of primary collaterals, the ACoA and to a lesser extend the PCoA. Antegrade flow in the ophthalmic artery was indicative of a good collateral status through the circle of Wills. 32 Notably, transcranial ultrasound examination in patients with ICA occlusions allows for an indirect detection of leptomeningeal collaterals through the PCA toward the MCA territory. In these cases, a high-velocity and low-resistance flow in the ipsilateral PCA, in the absence of ipsilateral PCoA or distally to a functional ipsilateral PCoA, is indicative of leptomeningeal collateral network recruitment. 33 More recently, transcranial ultrasound perfusion imaging has emerged as a potential diagnostic tool to assess cerebral perfusion in cases with severe ICA stenosis or occlusion. The ultrasounds are performed with phase-inversion-harmonic-imaging and bolus application of contrast media with subsequent semiquantitative analysis of time-intensity curves. Time-to-peak intensity values are the main parameter to be assessed. 34
For patients capable of performing apnea test, calculation of the vasomotor reactivity (VMR) with the Breath Holding Index can provide useful information about the cerebrovascular reserve (CVR).35,36 Indeed, impaired CVR has been associated to increased risk of ischemic stroke in patients with severe ICA disease. 37 A previous transcranial Doppler ultrasonography study of patients with ICA occlusion found that impaired VMR significantly increased the probability of AIS to an annual risk of 32.7%. Notably, patients with 1 major collateral pathway had a much higher risk of AIS of 17.5% compared with 2.7% for those with 2 collateral pathways. 38
An even more severe manifestation of impaired VMR is the reversed Robin Hood syndrome, described in patients with acute MCA or ICA occlusions. It is characterized by a blood flow velocity reduction in the ipsilateral to the occlusion intracranial arteries at the time of a blood flow velocity increase in the contralateral arteries. The steal phenomenon can be transient, spontaneous, or induced by vasodilatory stimuli such as breath holding. 39 Apart from being a mechanism responsible for early neurological deterioration in AIS patients, reversed Robin Hood syndrome has also been independently associated with a higher stroke recurrence risk within 6 months after AIS or TIA.40,41
Other imaging modalities for the identification of cerebrovascular reserve in patients with ICA occlusion include the (99) technetium(m)-hexamethyl propylene amine oxime single photon emission computed tomography (HMPAO-SPECT) with acetazolamide challenge and the magnetic resonance spectrometry (MRS). 42 In cases with insufficient collaterals, the MRS shows decreased N-acetylaspartate/choline, and increased lactate/N-acetylaspartate in the affected brain regions. 43
Another important consideration regarding the urgent imaging of AIS patients is the accurate differentiation by means of CTA between a pICAO and an ICA pseudo-occlusion due to a distal (intracranial) ICA occlusion, the latter rendering the patients candidates for MT. This distinction is also important for the definition of the revascularization technique that might be employed. Indeed, a retrospective review by different experts of CTAs from 37 patients found sensitivity and specificity for detecting ICA pseudo-occlusions of 68% and 75%, respectively, with a poor interobserver agreement (κ = 0.32; 95% CI: 0.16–0.47). 44 A similar retrospective analysis of 46 cases by two readers showed a sensitivity for detecting pseudo-occlusions on CTA of 82% (95% CI: 57–96) for both readers, and specificities of 76% (95% CI: 56–90) and 86% (95% CI: 68–96), respectively, with satisfactory interobserver agreement (κ value of .77). Pseudo-occlusion was suspected when a gradual contrast decline above the level of the carotid bulb was detected, especially coupled with a terminal ICA occlusion. 45 Therefore, characteristic imaging features to look for include a delayed filling of the ICA and/or a beak filling pattern in the proximal ICA both indicative of pseudo-occlusions, and a flat pattern present in cases of true pICAOs (Figure 1).7,46 Moreover, in our experience, absence of filling of the ipsilateral to the occlusion ophthalmic artery when the ipsilateral common carotid artery is injected with contrast might also serve as a potential indirect sign for the presence of intracranial ICA occlusion.

Digital subtraction angiography: Pseudo versus true occlusion of the proximal ICA. A beak filling pattern (arrow) of the proximal ICA after the carotid bulb (a) in a patient with intracranial thromboembolic ICA occlusion that underwent MT with thromboaspiration alone. The absence of filling of the ipsilateral to the occlusion ophthalmic artery (arrow) when the ipsilateral common carotid artery is injected with contrast (b) might also serve as a potential indirect sign for the presence of an intracranial ICA (arrow) occlusion (proximal ICA pseudo-occlusion) (c). Contrarily, a flat filling pattern is observed in a case of true proximal ICA occlusion of atherosclerotic origin (arrow) (d). Note that after injection of contrast in the ipsilateral to the occlusion CCA, there is a retrograde filling of the ipsilateral ophthalmic artery (arrow) irrigating partially the ipsilateral carotid siphon (arrowheads) (e). This patient was treated with urgent balloon angioplasty and stenting (arrow) (f). A beak filling pattern might also be observed in cases with dissection-related occlusion of the mid/distal extracranial ICA (arrow) (g). In this case, despite the absence of an intracranial ICA occlusion, there is no retrograde filling of the ipsilateral ophthalmic artery when the ipsilateral CCA is injected with contrast, instead the ophthalmic artery shows an antegrade filling (arrow) (h) from the contralateral ICA which irrigates partially the ipsilateral carotid siphon (arrow) (i) through the anterior communicating artery.
Treatment
IVT
The management of acute pICAOs may vary according to the specific characteristics of each case but also the expertise of each center. The only evidence-based treatment is IVT, administrated according to the current eligibility and exclusion criteria in acute AIS. In other words, complete pICAO is not a contraindication for IVT, irrespective of its cause (for instance, dissection). 47 However, low recanalization rates of 5%–13% constitute an important limitation of IVT.48,49 Moreover, a subanalysis of the EPITHET clinical trial showed worse outcomes by IVT given within 3–6 h after symptom onset in patients with ICA occlusions compared with controls (modified Rankin Scale [mRS] score, 5–6 at 3 months: OR, 11.2; 95% CI: 1.1–120.4; p = 0.04). 50 The limitation of this study relates primarily to the delayed time window of IVT.
Subsequently, the case–control multicenter prospective Internal Carotid ARtery Occlusion study (ICARO) investigated the efficacy and safety of IVT in AIS patients, with ICA occlusion, administrated within 4.5 h of symptom onset. The probability of a favorable outcome defined as an mRS score of 0–2 was significantly higher with IVT compared with controls (adjusted odds ratio [OR], 1.80; 95% CI: 1.03–3.15; p = 0.037). However, any intracranial hemorrhage (ICH) and death were more common with IVT (adjusted OR, 1.80; 95% CI: 1.03–3.15; p = 0.037 for ICH; adjusted OR, 2.28; 95% CI: 1.36–3.22; p = 0.001 for death) due to higher rates of cerebral edema in patients treated with systemic thrombolysis. 18 A recent systematic review of 7 studies comparing the reperfusion strategies for AIS due to isolated pICAO found that the 28% of cases achieved a favorable functional outcome (mRS 0–2). Rates of symptomatic ICH and death were 6.1% and 25.1%, respectively. Successful recanalization was calculated at surprisingly high rates of 14.6%. 51 However, only 5 of the 7 studies reported rates of successful recanalization, the definition of successful recanalization differed between studies, whereas in the largest study that reported rates of successful recanalization these were at 24 h post-treatment and at rates of 54%, suggesting probably an overestimation of the effect of systemic thrombolysis. 52 Collectively, although IVT for pICAOs appears to be beneficial and should be offered to all eligible patients, the rates of successful recanalization are low, while the rates of sICH are not neglectable.
Endovascular therapy
MT is a powerful and highly efficient treatment for LVO-attributed AIS, which has revolutionized stroke management.53,54 However, the benefits from acute intravascular treatment for isolated pICAOs are less well established, since these cases are rare compared with intracranial LVOs, and since patients with isolated pICAOs were not included in RCTs of MT. In the literature, treatment options for the off-label endovascular reperfusion of pICAOs include intra-arterial thrombolysis (IAT), microwire clot disruption with stenting, balloon angioplasty with or without stenting, and thrombectomy via stent retriever or aspiration. 55
The efficacy and safety of emergent endovascular revascularization for acute pICAOs has been addressed only in retrospective studies. Nikas et al. reported on 18 patients with moderate severity AIS (median National Institutes of Health Stroke Scale [NIHSS] of 8.5) receiving angioplasty with carotid artery stenting (CAS) within 6 h of symptom onset. Recanalization rates were 83.3% and median mRS at 30 days was 1, whereas stroke recurrence or death occurred in 11.1%. 56 Hauck et al. treated 22 patients with pICAOs presenting with severe strokes (mean NIHSS of 14). Poor outcomes (mRS > 2) were recorded in 50% of cases and were associated with the presence of atrial fibrillation, admission NIHSS scores ⩾ 20, and complete occlusion of the ICA in its entire course. 57 A larger case series comprising 264 patients with ICA occlusions pretreated with IVT, examined the efficacy of add-on endovascular treatment. In this cohort, there were 185 patients with extracranial ICA occlusions, of whom 76 received emergent CAS or thrombectomy. Endovascular treatment significantly improved the likelihood of achieving a favorable functional outcome at 3 months (OR 2.74, 95% CI: 1.65–4.56) and reduced mortality rates (OR 0.17, 95% CI: 0.08–0.38). 58
The study by Jadhav et al. focused exclusively on pICAOs. The median NIHSS was 8. The majority of patients had favorable baseline imaging profiles, with median Alberta Stroke Program Early CT Score (ASPECTS) of 9 and perfusion mismatch in 93% of cases. Moreover, clinical-imaging mismatch was present in 42% of patients. The decision to proceed with endovascular treatment was based either on the presence of a clinical-imaging mismatch, or on recurrent transient episodes or progressive neurological deterioration persisting ⩾24 h from symptom onset and despite appropriate conservative management. Successful recanalization with angioplasty and CAS occurred in 92% of cases leading to favorable 3-month outcomes in 65% of treated patients. Importantly, almost half of patients displayed a dramatic clinical improvement (NIHSS reduction of ⩾8 points) after the intervention. Rates of sICH were 6.5%, however, the most common complication, observed in 22% of cases and associated with early infarct growth, was distal embolization. These data underscore the importance of an individualized approach with careful selection of cases that might benefit from early recanalization. 59
In this context, a single center retrospective study of consecutive patients with acute ICA occlusion that did not undergo immediate endovascular treatment, aimed to explore the natural course the disease. Fifty-six patients, presenting with a relatively low median NIHSS of 3, were identified. Neurological deterioration within the first 7 days occurred in 11 patients (20%), and was associated with a baseline perfusion mismatch volume of >40 ml. Four patients received emergent endovascular treatment due to neurological deterioration, whereas at 3 months, 13 more patients had evidence of ICA patency. Although patients initially presented with relatively low severity strokes, functional independence was achieved in just 69% of the total cohort. 60 Apparently, in AIS patients presenting with mild neurological deficits due to acute extracranial ICA occlusion, deterioration or recurrence due to an underlying hemodynamic instability is not uncommon and should be ideally either predicted or aggressively treated when occurring.
A more recent study compared the outcomes between extracranial and intracranial ICA occlusions treated with MT (using stent retrievers or thromboaspiration) within 6–24 h after stroke onset. Rates of functional independence and mortality at 3 months were similar between the two groups (36% versus 40% and 7% versus 10%, respectively), whereas no sICH was observed after recanalization of pICAOs. 61 Similarly, Park et al. evaluated the efficacy of endovascular treatment in 29 patients with isolated pICAOs and compared outcomes with 46 cases presenting with tandem occlusions (concurrent extracranial ICA occlusion and intracranial LVO). Successful reperfusion was achieved in 96.6% and 84.0%, respectively. Favorable functional outcome was reported for 64% of total cases at 3 months follow-up, which was not different between the two groups. 62 These data support the concept that symptomatic acute isolated pICAOs, causing significant and critical hypoperfusion, should be perceived as equally important as intracranial occlusions, and early recanalization is both feasible and safe. Indeed, in several stroke centers endovascular treatment may be offered without perfusion imaging in patients presenting within 6 h of symptom onset with disabling neurological deficits due to isolated pICAO. Notable, the authors of a small case study with 9 individuals suffering from acute pICAOs with hemodynamic compromise suggest that in case ICA recanalization cannot be achieved, stenting of other cervical large arteries, such as the vertebral arteries, may be considered in order to alleviate brain ischemia through augmentation of collateral circulation. 63
Data from high-quality meta-analyses on urgent pICAO recanalization are lacking. A systematic review of 32 studies found that stenting compared with intrarterial thrombolysis resulted in higher recanalization (87% versus 48%, p = 0.001) and favorable outcome rates (68% versus 15%, p < 0.001) and lower mortality (18% versus 41%, p = 0.048). 55 A more recent study showed that compared with IVT, combined IVT plus endovascular treatment was associated with higher rates of favorable outcome (OR, 2.2; 95% CI: 1.3–3.7). Notably, compared with endovascular treatment alone, bridging therapy (IVT plus endovascular treatment) resulted in higher rates of favorable outcome (OR, 1.9; 95% CI: 1.1–3.4). However, the quality of analyzed studies was low, whereas no RCTs were included. 51
Angioplasty and stenting for dissection-related pICAOs is technically more challenging compared with atherosclerotic or embolic occlusions, hence it should be reserved for carefully selected patients, refractory to conservative treatment. Indeed, the risks of the endovascular procedure include the expansion of dissection due to accidental catheterization of the false lumen, and a sICH due to reperfusion injury. The latter might have a higher risk of developing in patients with dissections compared with those with atherosclerotic occlusions, because of the absence of leptomeningeal collateral recruitment in the acute phase. Indeed, a recent study of 22 patients treated with angioplasty assisted stenting for acute ICA dissections reported sICH rates of 18.2%. 64 Moreover, dissections typically involve a longer arterial segment than atherosclerosis, necessitating longer or multiple stent deployment. Nevertheless, several case series have reported high rates of recanalization and an overall technical success of the endovascular procedure for the treatment of ICA dissections, coupled with high functional independence rates of >80%, especially in the absence of tandem occlusions.64–67 On the contrary, the risk of distal embolization seems lower, and thus use of distal protection devices is not critical. 64 However, in these studies only subgroups were treated in an emergency LVO context due to dissection-related pICAO. The majority of the patients presented with non-occlusive extracranial dissections. Also, there was a low rate of IVT treatment and almost all patients received intravenous heparin and double antiplatelets before endovascular treatment, which are considerable elements in the acute onset stroke. Current European Stroke Organization (ESO) guidelines recommend endovascular therapy in selected patients with isolated extracranial ICA dissection based on expert opinion. 68
Carotid endarterectomy
Several small-scale case series have reported outcomes on emergent carotid endarterectomy for patients with acute isolated pICAOs. Notably, in these studies, surgery was performed within a few hours after stroke onset, whereas some patients were pretreated with IVT.69–71 Patient selection was largely based on the identification of salvageable brain tissue using perfuse imaging. Favorable outcomes were reported for the majority of patients, which, however, had undergone careful selection with the aim of identifying potential candidates that may benefit from early revascularization. A recent literature review of studies published after the year 2000 identified 175 patients that underwent emergency carotid endarterectomy. The study found high rates of recanalization (93%), early neurological improvement (66%), and favorable functional outcome (62%). Rates of symptomatic ICH (4%) and mortality (5%) were low. However, the time of surgery varied considerably within the studies, from hours to several days after symptom onset. 72
Although there are no studies comparing endarterectomy with endovascular revascularization in the setting of acute pICAOs, emergency surgery might be an alternative for patients with large penumbra or severe neurological deterioration, and technically challenging angioplasty/stenting for anatomical reasons or lack of expert interventionists. Nevertheless, surgery might be more hazardous compared with endovascular procedures for hemodynamically unstable patients, cases pretreated with IVT, and those with contralateral ICA severe stenosis or occlusion. Moreover, endovascular procedures are the only option for cases with tandem distal ICA or MCA occlusions. Importantly, a possible distal embolization during the interventional procedure, either surgical or endovascular, may be only recognized and potentially treated when patients undergo endovascular reperfusion therapies.73,74
Εxtracranial–intracranial bypass
Εxtracranial–intracranial (EC–IC) bypass surgery has been studied as a rescue intervention for cases with symptomatic ICA or MCA occlusion and subsequent subacute or chronic hemodynamic impairment. However, since two RCTs failed to show clinical benefit from EC–IC bypass surgery, this intervention is seldom used by most stroke experts. The first RCT recruited patients with stenosis or occlusion of the ICA or MCA, while the second with ICA occlusion only but with additional documentation of cerebral ischemia by positron emission tomography scan. Notably, both studies reported increased rates of early postoperative stroke in the intervention group, and in fact, the most recent Carotid Occlusion Surgery Study was terminated earlier for futility.75,76
EC–IC has been also investigated as an emergency treatment modality for hemodynamically unstable LVOs in the settings of non-randomized retrospective studies. A small case series comprising 8 patients operated within hours after clinical recurrence or deterioration reported improvement in MRI perfusion/diffusion mismatch in 50% of cases. 77 However, a larger study of 81 patients, the majority (85%) with ICA occlusions, showed that perioperative stroke rates were higher for cases operated early (within 7 days of the index event) compared with late surgery (31% versus 11.5%, p = 0.04). 16 Therefore, because of an unacceptably high, early postoperative risk but also because of lack of efficacy, EC–IC bypass surgery is currently not indicated for the acute management of patients with pICAOs.
Induced hypertension
Observational data from small pilot studies indicate that phenylephrine-induced hypertension may be associated with neurological improvement in patients with AIS due to large artery atherosclerotic extra- or intracranial steno-occlusive disease.78–80 The Safety and Efficacy of Therapeutic Induced HYPERTENSION (SETIN-HYPERTENSION) trial was a small phase II RCT conducted in Korea that provided preliminary evidence in favor of induced hypertension in AIS patients with major neurological deficits (NIHSS-score 4–18) from non-cardioembolic stroke etiology who were ineligible for endovascular reperfusion therapies. 81 Current European Stroke Organization (ESO) guidelines recommend careful use of vasopressor agents to increase blood pressure with close monitoring of blood pressure values in AIS not treated with systemic or endovascular reperfusion therapies and with clinical deterioration where a hemodynamic mechanism is suspected or shown to be directly responsible for the neurological deterioration. 82 This recommendation parallels our own clinical experience (Figure 2).

A 49-year-old man with a history of left intracranial ICA dissection 2 years ago, presented with an episode of amaurosis fugax of the right eye. Neurosonology examination showed pre-stenotic flow spectrum in the proximal right ICA (a), as well as an intimal flap (arrowhead) and intramural hematoma (arrow) (b). Blood flow reversal was noted only in the right PCoA (c), while the A1 segment of the left ACA was absent, precluding any possibility of collateralization via the ACoA. Mean blood flow velocity on the right MCA was 41 cm/s (d). Brain/cervical MRI verified the recurrence of a non-occlusive extensive ICA dissection, this time on the right side, by disclosing increased intramural ICA signal (arrow) in the FLAIR sequences (e). The patient was treated with low-molecular weight heparin and bed rest. Seven days after admission and 1 day after the patient was dismissed from the stroke unit, he was re-submitted due to an episode of dysarthria and right hemiparesis. Emergent brain DWI-MRI revealed acute infarcts in the internal MCA watershed area (f), whereas T1-Fat saturation sequences showed an intramural hematoma (arrow) causing near-occlusion of the right ICA (g). TCCDS verified the worsening of blood flow in the right MCA, with a mean flow velocity of 28.5 cm/s (h) and absence of vasoreactive response during the breath holding test. MRI-Perfusion using RAPID software study showed a critically hypoperfused area of 25 cc, without detectable infarct core volume, within the territory of the right MCA (i). The patient was treated conservatively, with blood pressure elevation and bed rest. After several transient brief episodes of dysarthria during the following days, the patient stabilized and was dismissed without further recurrences. Neurosonology follow up showed improvement in the blood flow of the right proximal ICA (j) and the right MCA (mean flow velocity of 39 cm/s) (k). NIHSS-score at discharge was 0.
Conclusion
Isolated pICAO is not an uncommon condition with variable clinical presentation, ranging from asymptomatic to severe hemispheric strokes. Progressive ICA occlusions often cause milder strokes due to progressive occlusion and augmentation of collaterals. Accurate and prompt diagnosis is critical in order to plan therapeutic strategies aiming to avert and/or prevent cerebral ischemia. Among the different diagnostic modalities, cervical and transcranial ultrasounds allow for the rapid diagnosis of pICAO, the potential etiologic differentiation, as well as the continuous real-time monitoring of ipsilateral intracranial blood flow and the estimation of cerebrovascular reserve.
There is low-quality data regarding treatment decisions for acute pICAOs. IVT administrated within the approved time windows is both safe and effective. Non-randomized data has shown that endovascular treatment might be feasible, safe and effective in averting neurological deficits and in preventing further clinical deterioration (Figure 3). An off-label acute interventional recanalization of pICAOs might be considered for cases with severe strokes at presentation or those with neurological deterioration. The detection of large volumes of salvageable brain tissue at risk coupled with the absence of large ischemic core through perfusion imaging, has been largely used by most studies and is highly recommended. Importantly, an individual approach is warranted with careful patient selection for treatment and close pre- and post-intervention monitoring by stroke experts in order to minimize the likelihood of severe complications following reperfusion (Figure 4). In Table 1 we present the theoretical advantages and disadvantages of the different therapeutic options for the acute treatment of pICAOs.

A 39-year-old woman presented with acute onset mild left hemiparesis, with a NIHSS-score of 4 points. She reported headache and an episode of right amaurosis fugax the day before admission. CTA showed a proximal right ICA near occlusion (a), CT-Perfusion using RAPID software showed a critically hypoperfused area of 36 ml volume in the internal watershed area of the right MCA (b), and brain DWI-MRI disclosed acute infarcts in watershed areas of the right MCA territory (c). Twelve hours later, significant clinical worsening was noted with left hemiplegia and NIHSS-score of 11 points. An emergent CTA-CT Perfusion study showed occlusion of the right ICA and extension of the critically hypoperfused area, with a Tmax >6 s, to 50 cc, without any ischemic core (rCBF < 30%) (d). Blood pressure augmentation partially improved patient’s clinical condition. The patient was transferred to the angiography suite, where angioplasty assisted stenting was performed. The intervention resulted in significant clinical improvement, and the patient was discharged with a NIHSS-score of 3. Brain DWI-MRI showing moderate infarct expansion (e, f).

A schematic treatment algorithm proposed for the management of cases with acute proximal internal carotid artery occlusions.
Theoretical advantages and disadvantages of the different therapeutic options for the acute treatment of proximal isolated internal carotid artery occlusions.
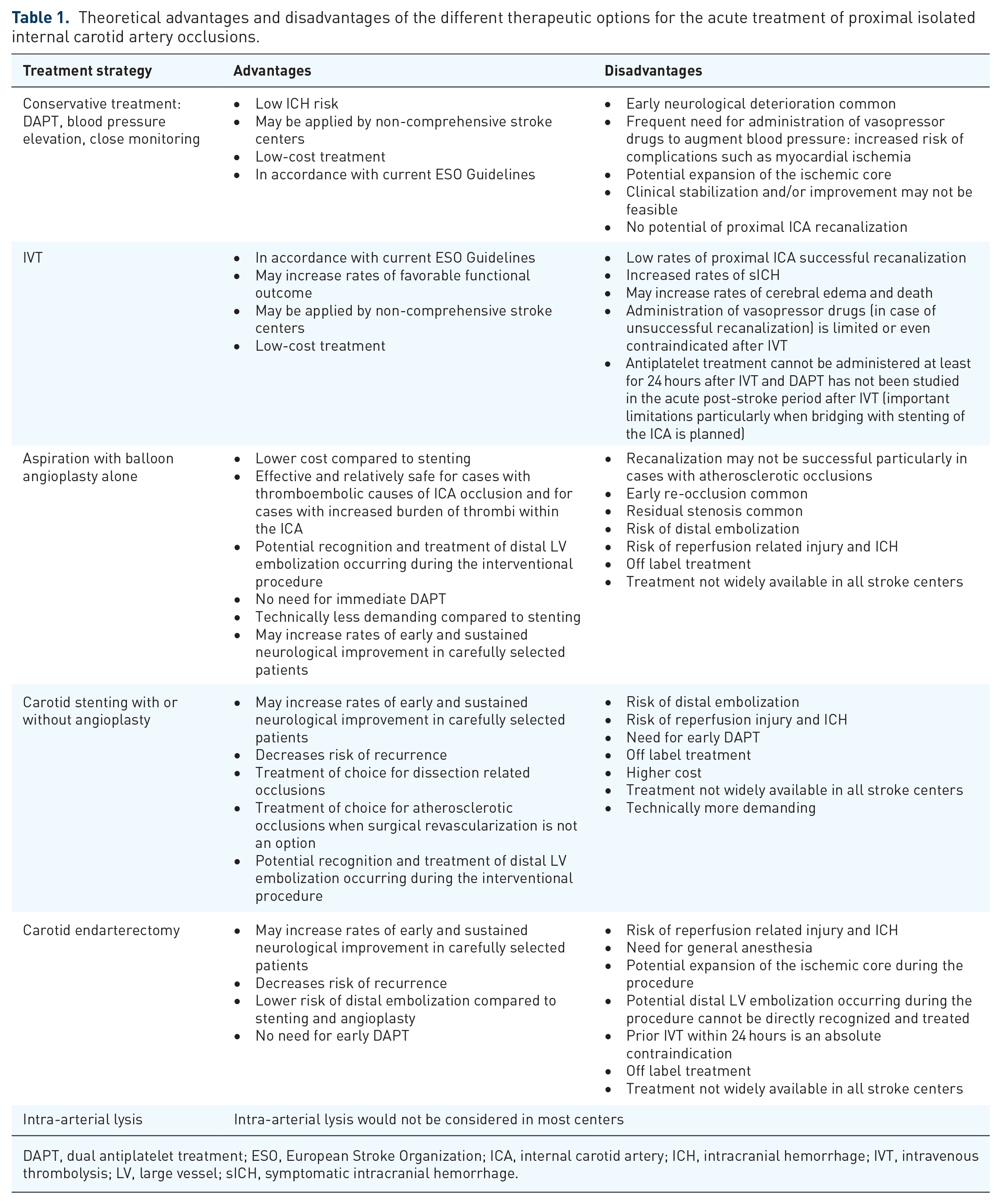
DAPT, dual antiplatelet treatment; ESO, European Stroke Organization; ICA, internal carotid artery; ICH, intracranial hemorrhage; IVT, intravenous thrombolysis; LV, large vessel; sICH, symptomatic intracranial hemorrhage.
On the contrary, the design of RCTs investigating the safety and efficacy of endovascular therapies for symptomatic isolated pICAOs is complicated and challenging. Heterogeneities in the etiology of ICA occlusion, clinical presentation, natural course, cerebrovascular reserve and collateral status are almost universal, and in conjunction with a technically demanding endovascular procedure, are all factors to consider in the design of future clinical trials. The implementation of data obtained from perfusion imaging and the evaluation of cerebrovascular reserve are of paramount importance. In respect to the former, the perfusion thresholds and/or the clinical-imaging mismatch requirements that have been successfully utilized in the recent RCTs on late time window MT for LVO-attributed AIS might serve as foundations to develop similar thresholds for patient selection in case of pICAOs.83,84